
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Mucorales-associated osteomyelitis in an immunocompetent child
Murat Sutcu1; Manolya Kara1; Niran Tekkeli2*; Kaya Turan3; Haluk Cabuk3
1Department of Pediatric Infectious Diseases, Faculty of Medicine, Istinye University, Turkey.
2Department of Pediatrics, Faculty of Medicine, Yeditepe University, Turkey.
3Department of Orthopedics and Traumatology, Faculty of Medicine, Istinye University, Turkey.
*Corresponding Author : Niran Tekkeli
Department of Pediatrics, Faculty of Medicine,
Yeditepe University, Turkey.
Tel: +90 5441132393.
Email: niran.tekkeli@yeditepe.edu.tr
Received : Feb 20, 2024
Accepted : Mar 12, 2024
Published : Mar 19, 2024
Archived : www.jcimcr.org
Copyright : © Tekkeli N (2024).
Citation: Sutcu M, Kara M, Tekkeli N, Turan K, Cabuk H. Mucorales-associated osteomyelitis in an immunocompetent child. J Clin Images Med Case Rep. 2024; 5(3): 2930.
Introduction
Mucormycosis is an opportunistic, aggressive, luckily rare fungal infection that most commonly causes pulmonary, sinoorbital, gastrointestinal, and skin disease [1]. Its incidence is 1.5% among invasive fungal infections [2]. But, the mortality from mucormycosis is significantly high (>30-50%), with disseminated disease accounting for 90% of deaths. Patients with localized cutaneous disease have a much lower mortality rate while it is still significant (10-30%) [3]. Although diabetic ketoacidosis and immunodeficiency are wellknown risk factors for the infection, cases of Cutaneous Mucormycosis (CM) in previously healthy subjects secondary to trauma have been reported [4]. Following inoculation of the fungus into the skin, the infection can progress to the subcutaneous tissue, muscle, and bone. Osteoarticular Mucormycosis (OAM) is extremely rare. Even so, if not diagnosed and treated promptly, it can have serious consequences, including amputation of extremities and death. Herein, we describe a rare instance of mucorales-associated osteomyelitis in an immunocompetent child who survived amputation with the combination of antifungal therapy and surgery.
Case report
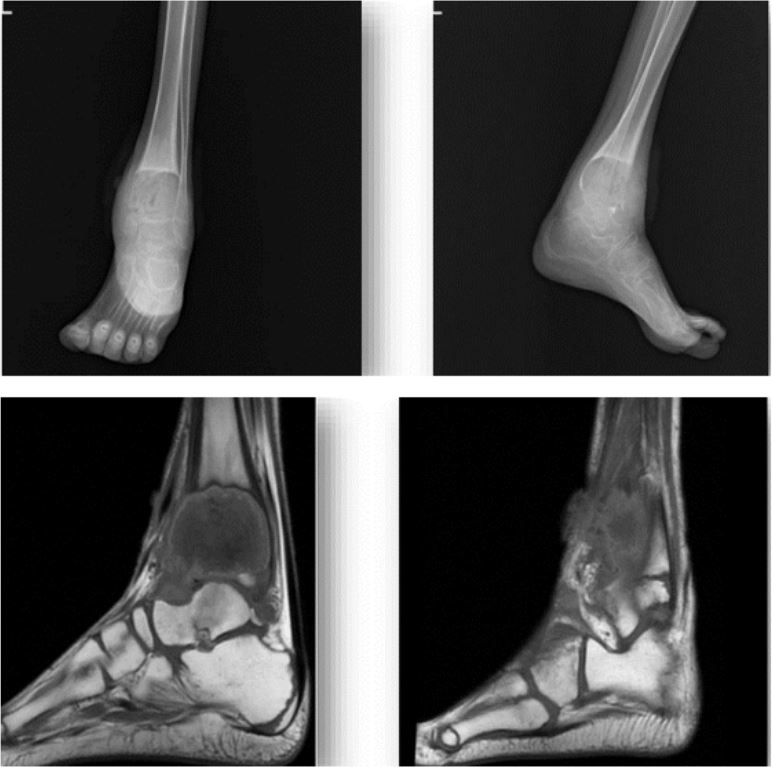
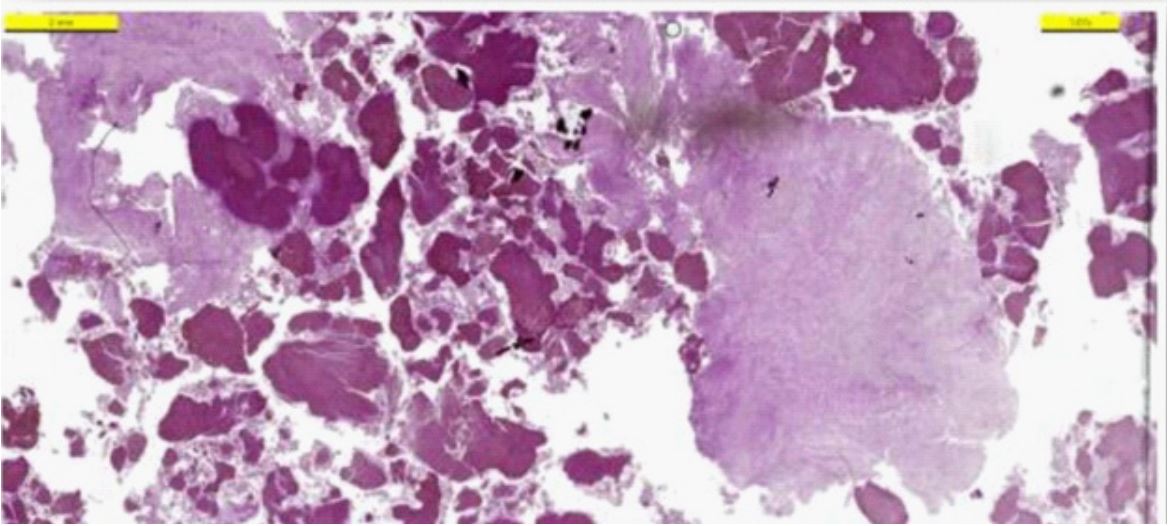
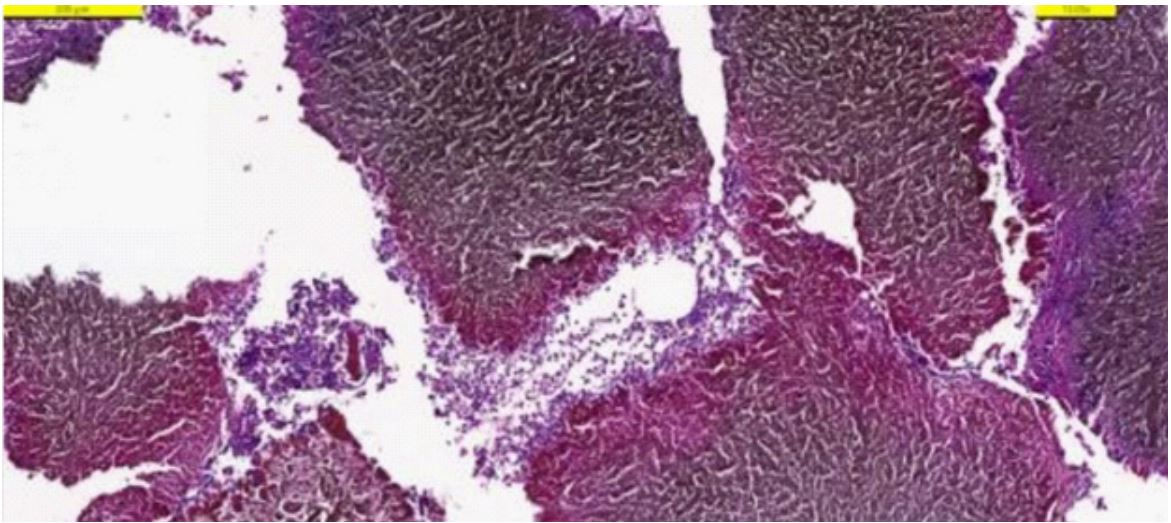
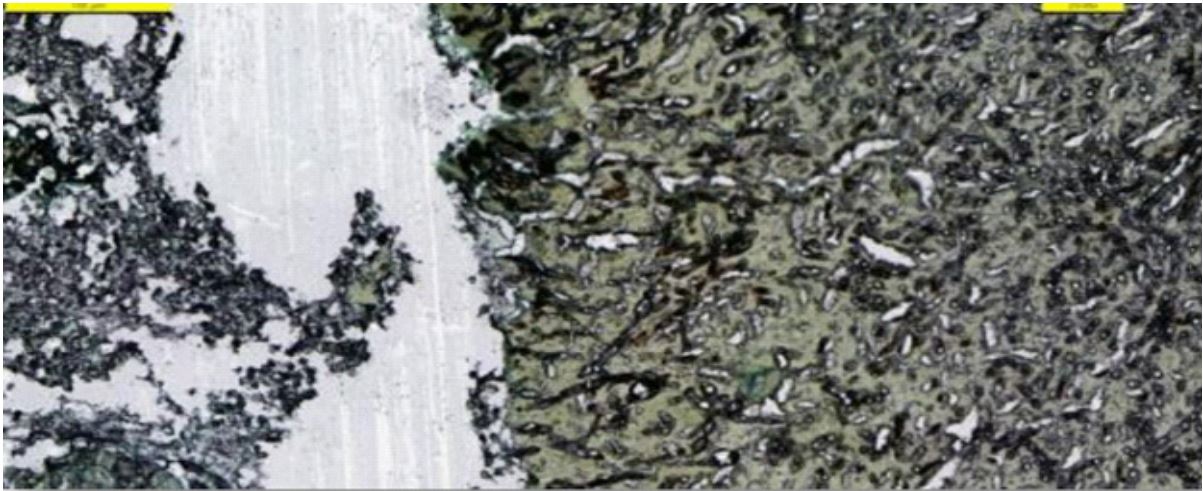
A previously healthy 10-year-old boy was attended to our clinic with a non-healing wound on the frontal surface of his left ankle. Ten months ago, he suffered a sharp-penetrating injury in the location of the lesion. He complained of swelling, discharge, and redness 15 days after the insult. He was internalized with the preliminary diagnosis of cellulitis and osteomyelitis and was given parenteral antibiotics for 2 weeks, and then continued with oral antibiotics. Although the redness and the discharge subsided, the lesion did not resolve completely. Due to the lack of improvement and the enlargement of the swelling at the 6-month follow-up, X-ray imaging was performed and revealed cystic lesions. Then, he underwent a bone biopsy. Histopathology was evaluated as chronic osteomyelitis and non-specific findings. Since he was recommended to undergo an amputation, he was brought voluntarily to our unit for a second opinion and further research. On examination, he was afebrile and hemodynamically stable. His systemic examination was unremarkable other than a localized 8×10 cm area of erythematous swelling over the distal anterior surface of his left leg just proximal to the ankle. The wound emitted an extremely foul odor. There was a necrotic center and a purulent discharge from the lesion (Figures 1A-C). Laboratory examination revealed a white blood cell count of 7,12×109 /L with predominant neutrophilia. C-reactive protein and erythrocyte sedimentation rate (ERS) were increased (4.2 mg/dL (normal <0.5) and 42 mm/hour (normal< 20), respectively). The patient was started on parenteral teicoplanin (12 mg/kg/loading dose, 3 times, 12 hours apart; then 10 mg/kg/day] and meropenem (60 mg/kg/day, 3 times) treatment after taking wound and blood culture samples. No growth was observed in blood culture, though wound culture yielded polybacterial growth. X-ray and Magnetic Resonance Imaging (MRI) revealed a cystic lytic lesion on the distal tibia expending and eroding the distal physis of the tibia and ankle joint (Figures 2A-D). During surgery, it was observed that the medial cortex of the distal tibia was completely destroyed and fistulized from there. Abundant necrotic tissue was removed from the bone and surrounding tissues (Figures 3A-B). The sinus tracts were excised, and the material was sent to the pathology. At the first stage of the surgery, an antibiotic (vancomycin) embedded chain was placed into the defected intramedullary area. Histopathological examination of the removed tissue was found to be compatible with mucormycosis (Figures 4A-C). The patient was started on liposomal amphotericin B (L-AMB; 5 mg/kg/day), afterward. Broad-spectrum antibiotic therapy, which was started empirically, was discontinued on the 10th day of treatment. In the 8th week of the antifungal therapy, the second stage of the surgery was performed. The antibiotic chain was removed, and remnant mucormycotic tissues were debrided extensively. The tibial surface of the tibiotalar joint was destructed. The articular surface of the talus and distal femurand medial malleoli were excised and the bony defect was measured. There was a total of 4 cm bone loss. Then a 9 cm long ipsilateral fibular strut graft was harvested in a non-vascularized manner. One side of the strut was placed into the tibial intramedullary area, and the other side was inserted directly into the 1 cm deep cavity, which was created by an autologous cartilage harvester at the talus. Tibiotalar arthrodesis was completed by a lateral malleolus anatomical plate which is placed medially from talus to tibia. Stability was assessed before closure, and no additional external fixation was required. The clinical findings of the patient showed significant improvement with surgical debridement and L-AMB therapy. He started to put on weight on his feet in the first week of treatment with a walking cast. ESR decreased to 22 mm/h. We did not consider amputation because the patient responded very well to surgical debridement and antifungal treatment. We decided to switch to oral posaconazole (300 mg twice daily for 2 doses, then 300 mg once daily) therapy and close clinical follow-up because the patient wanted to return to his country for social reasons.



Discussion
Mucor spp. are filamentous fungi with typically broad, thinwalled septate hyphae. They are fast-growing opportunistic pathogens that can lead to invasive infections, especially in immunocompromised patients and diabetics [3]. These organisms are ubiquitous in nature, including putrefying plants and soil [5]. The most common clinical syndromes include rhino orbital-cerebral, pulmonary, gastrointestinal, and Cutaneous Mucormycosis (CM) [6]. In a French study of 101 patients with mucormycosis, hematologic malignancy was the most common Figures 1(A-C): A 10-year-old boy with an 8x10 cm area of swelling over the distal anterior surface of his left leg just proximal to the ankle. Figures 2: The anteroposterior and lateral X-ray view of the ankle, note a cystic lytic lesion on the distal tibia expending and eroding the distal physis of the tibia and ankle joint (A and B). T1 MRI secs of the same lesion, showing a uniform solid pattern, with eroding the distal tibia and subcutaneous tissue on the anterior part of the ankle (C and D). risk factor, occurring in 50% of patients, followed by diabetes in 23% of cases [7]. Trauma-related mucormycosis was observed in 18%. The same study revealed that the lungs (28%; 79% in hematology patients) and rhinocerebral (25%; 64% in diabetic patients) involvement were the leading sites of infection [7]. CM infection can occur after any condition that disrupts the skin barrier integrity. This situation can range from major trauma such as war, earthquake, or traffic accident tosomething as minor as a mosquito bite, or a skin abrasion to surgical intervention [8,9]. Penetrating trauma in our previously healthy case provided access to the development of mucor infection. Mucorales have a strong proclivity toinvade blood vessels, resulting in thrombosis, necrosis, and tissue infarction [10]. In most cases with CM, fungi can further spread to the bone and articular structure, resulting in Osteoarticular Mucormycosis (OAM). Fortunately, OAM cases are very rare, but the mortality can be as high as 30% [3]. Unless promptly diagnosed and aggressively treated, the infection can lead to a catastrophic event potentially necessitating extremity amputation [11]. Despite the fact that mucor could not be the final diagnosis in his country, amputation was recommended due to existing bone involvement. The osteolytic lesion, bone erosion, and MRI T2 weighted signal intensity are diagnostic imaging features that are consistent with the infection process but not specific to OAM [11]. Therefore, biopsy for culture and histopathology should be included in the evaluation of suspected mucormycosis of bone and joint. However, diagnosis may be delayed in cases where histopathology is not guiding. In the present case, a bone biopsy was performed before, but the findings were consistent with nonspecific inflammation. Although the clinical situation partially improved after broad-spectrum antibiotics, he was not given antifungal therapy. The invasive mucor infection progresses rapidly in most cases. However, in the case of cutaneous and bone involvement, the progression of the disease may follow a relatively chronic course. The average time to diagnosis for OAM was reported as 73 days in the previous case series [11]. There was a period of approximately 10 months before the diagnosis in the present case. The management of OAM includes surgical intervention with antifungal therapy. Mucorales are resistant to many antifungal agents. L-AMB has been the cornerstone of mucormycosis treatment [3]. In some cases, combination therapy with azoles may be required. After control with intravenous induction, oral agents (posaconazole or isavuconazole) may be employed to continue treatment. Unfortunately, there are no evidence based treatment recommendations, particularlyfor pediatric OAM patients. While managing our case, we initially preferred L-AMB in light of literature data. Since he showed dramatic improvement with surgical debridement and antifungal therapy, we agreed with the orthopedists that no amputation was necessary. Our patient had to return to his country for social reasons. Thus, we tapered to posaconazole therapy on an outpatient basis, providing that close follow-up is maintained.
Conclusion
To summarize, OAM is a rare but dreadful disease that can also be seen in healthy individuals. The diagnosis can be challenging, particularly when it follows an indolent course. Prompt aggressive surgical debridement and antifungal agents remain the cornerstones of management.
References
- Roden MM, Zaoutis TE, Buchanan WL, et al. Epidemiology and outcome of zygomycosis: a review of 929 reported cases. Clin Infect Dis. 2005; 41: 634-53.
- Bitar D, Lortholary O, Le Strat Y, et al. Population-based analysis of invasive fungal infections, France, 2001-2010. Emerg Infect Dis. 2014; 20: 1149-55.
- Reid G, Lynch JP, Fishbein MC, Clark NM. Mucormycosis. Semin Respir Crit Care Med. 2020; 41: 99-114.
- Singla K, Samra T, Bhatia N. Primary cutaneous mucormycosis in a trauma patient with MorelLavallée lesion. Indian J Crit Care Med. 2018; 22: 375-7.
- Spellberg JE, and Ibrahim A. Novel perspectives on mucormycosis: pathophysiology, presentation, and management. Clin Microbiol Rev. 2005; 18: 556-69.
- Cox GM, Mucormycosis (zygomycosis). 2022. https://www.uptodate.com.
- Lanternier F, Dannaoui E, Morizot G, et al. A global analysis of mucormycosis in France: the RetroZygo Study (2005-2007). Clin Infect Dis. 2012; 54(1): 35.
- Shingde R, Cui R, Perera R. Cutaneous Mucormycosis in an Immunocompetent Child following a Minor Skin Trauma. Case Rep Surg. 2022; 2022: 7005024.
- Hubbard DC, Fleenor JW, Su MG, Tsai JH. A 47-year-old man with a necrotic wound after trauma. Digit J Ophthalmol. 2021; 17(27): 33-7.
- Petrikkos G, Skiada A, Lortholary O, et al. Epidemiology and clinical manifestations of mucormycosis. Clin Infect Dis. 2012; 54: 23-34.
- Taj-Aldeen SJ, Gamaletsou MN, Rammaert B, et al. International Osteoarticular Mycoses Consortium. Bone and joint infections caused by mucormycetes: A challenging osteoarticular mycosis of the twenty-first century. Med Mycol. 2017; 55: 691-704.