
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 5
An unusual localization of an Abrikossoff tumor
Kaoutar Mejjati1*; Sara Elloudi1; Rasha Moumna1; Zakia Douhi1; Meriem Soughi1; Hanane Baybay1; Leyla Tahiri Elousrouti2; Fatima Zahra Mernissi1
1Department of Dermatology, University Hospital Hassan II, Fez, Morocco.
2Pathology Department, University Hospital Hassan II, Fez, Morocco.
*Corresponding Author : Kaoutar Mejjat
Department of Dermatology, University Hospital
Hassan II, Fez, Morocco.
Tel: +21 2618332322.
Email: kaoutarme@hotmail.fr
Received : Feb 08, 2024
Accepted : Mar 13, 2024
Published : Mar 20, 2024
Archived : www.jcimcr.org
Copyright : © Mejjati K (2024).
Abstract
Abrikossoff’s tumor, also known as Granular Cell Tumor (GCT), is a rare benign neoplasm commonly found in the cervicofacial region, particularly the oral cavity. Here, we present a case of GCT occurring in an atypical location on the left flank of a 43-year-old patient. The lesion presented as an erythematous ovoid nodule with central ulceration, accompanied by white structures and polymorphic vascularization on dermoscopy. Initially considered as Darrier-Ferrand’s dermatofibrosarcoma, histopathological examination of a cutaneous biopsy revealed granular cells and eosinophils in the dermis, suggestive of GCT. Immunohistochemical analysis confirmed the diagnosis, expressing S100 protein and CD68. Complete surgical excision with safety margins was performed, with no recurrence observed after 1 year of follow-up. This case highlights the importance of considering GCT in the differential diagnosis of flank lesions and emphasizes the need for clinicians to remain vigilant for uncommon presentations of this rare tumor.
Keywords: Granular cell tumor; Abrikossoff’s tumor; Immunohistochemistry; Surgical excision.
Citation: Mejjati K, Elloudi S, Moumna R, Douhi Z, Soughi M, et al. An unusual localization of an Abrikossoff tumor. J Clin Images Med Case Rep. 2024; 5(3): 2932.
Introduction
Abrikossoff’s tumor, or Granular Cell Tumor (GCT), is a rare tumor, most often benign, with a ubiquitous distribution and a predilection for the cervicofacial region, particularly the oral cavity. Through this new observation, we report a case of GCT occurring in the flank region. This represents an atypical localization for this tumor type, emphasizing the need for clinicians to consider GCT in the differential diagnosis of flank lesions.
Case presentation
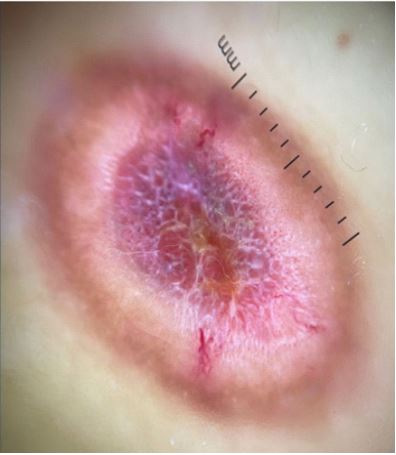
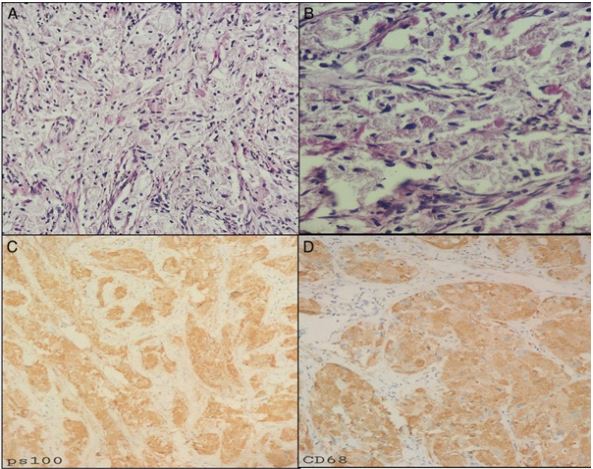
A 43-year-old patient, treated for an adrenal incidentaloma, consulted for a skin lesion that had been evolving for 6 months. Dermatological examination revealed an erythematous ovoid nodule, ulcerated in the center located in the left flank (Figure 1). Dermoscopy showed white structures and polymorphic vascularization (Figure 2). The rest of the examination found no associated abnormalities, in particular no palpable adenopathies. In the light of the clinical and dermoscopic data, we discussed a Darrier-Ferrand’s dermatofibrosarcoma first. A cutaneous biopsy was performed, showing a proliferation in the dermis dissociating collagen fibers containing granular cells and eosinophils (Figure 3A,3B), suggestive of a granular cell tumor or a histiocytofibroma. The immunohistochemical study concluded that it was a GCT, expressing protein S100 and CD68 (Figure 3C,3D). Surgical excision with safety margins was performed with no recurrence after 1 year of follow-up.

Discussion
Abrikossoff’s tumor or Granular Cell Tumor (GCT) is a rare benign tumor, first described by the Russian pathologist Abrikossoff in 1926, hence its name Abrikossoff’s tumor [1]. It occurs between the second and sixth decade of life, and is more common in females [2]. It can appear in several soft-tissue and visceral sites, but the most common localizations are the head and neck (45%-65%), more than half of which are located in the oral cavity, mainly in the tongue [3,4]. However, other sites can also be affected, such as the esophagus, larynx, trachea, parotid gland, thyroid, lungs, breast, chest wall and genitals. GCT is usually single and asymptomatic, although, multi-focal forms are possible. Clinically, GCT presents as a firm, polyploid or sessile papule or nodule, with a smooth, granular or warty surface, pinkish, greyish or yellowish in color [5,6]. The diagnosis is histological. The tumor consists of a proliferation of large, polygonal cells with abundant eosinophilic cytoplasm and hyperchromatic nuclei. On immunohistochemistry, tumor cells express neurogenic markers, notably S100 protein, CD 68 and enolase, confirming the neuronal origin of the tumor. The differential diagnosis is mainly with dermatofibromas and neurofibromas. Treatment is based on complete surgical excision with safety margins to prevent recurrence.
Conclusion
Granular Cell Tumor (GCT) is typically a singular and benign neoplasm, with histopathological diagnosis being crucial for confirmation. Surgical removal continues to be the primary approach for managing GCT. The uniqueness of our observation lies in the unusual localization of this tumor, emphasizing the importance of considering GCT even in atypical anatomical sites. This underscores the need for clinicians to maintain a broad differential diagnosis and remain vigilant for uncommon presentations of GCT.
Conflict of interest: None.
References
- Bernat Gili A, Ayerbe TV, Baena AA, Rivares EJ, Oncins TR. Abrikosoff’s tumor of the soft palate: A case report. An Otorrinolaringol Ibero Am. 1999; 26: 47-53.
- Gürsoy B, Energin K. Granular cell tumor: A case report. J Marmara Univ Dent Fac. 1997; 2: 6313.
- Kim HJ, Lee MG. Granular cell tumors on unusual anatomical locations. Yonsei Med J. 2015; 56: 1731-4. 10.3349/ ymj.2015.56.6.173.
- Pushpa G, Karve PP, Subashini K, et al. Abrikossoff’s tumor: an unusual presentation. Indian J Dermatol 2013; 58: 407. 10.4103/0019-5154.117335.
- Ayadi L, Khabir A, Fakhfakh I, Abdelmoula MH, Makni S, Sellami Boudawara T. Tumeur à cellules granuleuses. Rev Stomatol Chir Maxillofac. 2008; 109: 158-62.
- Sousa FB, Verde Osterne RL, Matos Brito RG, Negreiros Nunes Alves AP, Studart Soares EC, Gurgel Costa FW. Oral granular cell tumor: a study of twelve cases in a Brazilian population. J Clin Exp Dent. 2010; 2: 178-82.