
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
High-resolution intraoperative infrared thermography for the functional imaging and tumor resection maximization of a low-grade glioma: Technical case report
Diego Rodrigues Menezes1,2; William Cesar Fiorotti1; Lázaro de Lima1; Edson da Rocha Constantino1; Rafael Teixeira Magalhães Leal1; José Alberto Landeiro1; Aura Conci3; Marcus André Acioly1,2*
1Department of Surgical Specialties, Federal Fluminense University, School of Medicine, Niteroi, Brazil.
2Department of Neurosurgery, Pedro Ernesto University Hospital, Rio de Janeiro State University, Rio de Janeiro, Brazil.
3Federal Fluminense University (UFF), Niteroi, Brazil.
*Corresponding Author : Marcus André Acioly
Department of Surgical Specialties, Federal Fluminense University, School of Medicine, Niteroi, Brazil.
Email: marcusacioly@yahoo.com.br
Received : Feb 10, 2024
Accepted : Mar 13, 2024
Published : Mar 20, 2024
Archived : www.jcimcr.org
Copyright : © Acioly MA (2024).
Abstract
Currently, it is widely recognized the role of the extent of resection on overall and progression-free survival for gliomas surgery. Brain mapping and intraoperative image guidance are generally required to attain such an objective. Infrared Thermography (IRT) has a potential role in the identification of surgical margins, but it has not been consistently assessed in the literature. We aim to demonstrate the use of intraoperative IRT to detect superficial and deep tumoral margins of low-grade glioma, to identify adjacent functional motor cortex, and to maximize surgical resection in a 45-year-old lady with a long history of partial and secondary generalization seizures.
Keywords: Infrared thermography; Glioma; Intraoperative imaging.
Abbreviations: 5-ALA: 5-Aminolevulinic Acid; IRT: Infrared Thermography; MRI: Magnetic Resonance Imaging; FPS: Frame Per Second.
Citation: Menezes DR, Fiorotti WC, Lima LD, Constantino EDR, Acioly MA, et al. High-resolution intraoperative infrared thermography for the functional imaging and tumor resection maximization of a low-grade glioma: Technical case report. J Clin Images Med Case Rep. 2024; 5(3): 2933.
Introduction
Currently, it is widely recognized the role of the extent of resection on overall and progression-free survival for diffuse gliomas, regardless of the grade [1,3]. To achieve such an objective, functional-guided surgery is generally required [4]. The seminal meta-analysis by De Witt Hamer and colleagues demonstrated that intraoperative brain mapping mainly on local anesthesia in the awake setting was associated with fewer neurological complications and a greater extent of resection for all grades of diffuse gliomas [5]. For glioblastomas, the issue of functional preservation with awake mapping is somewhat controversial [6,7]. Besides brain mapping, intraoperative imaging based on fluorescence guidance by using several tracers has been increasingly used for glioma resection [8,9]. While 5-aminolevulinic acid (5-ALA) has become a new standard for high-grade glioma surgery, the impact of fluorescein-guided surgery is yet to be defined in terms of contributing to overall survival [8,9]. It is worth mentioning that positive 5-ALA fluorescence rates are rather low in low-grade gliomas, however [10]. Infrared Thermography (IRT) is a non-invasive imaging method used to detect surface temperature through naturally emitted radiation from the body. Regarding its application in brain tumors, IRT has a potential role in the identification of surgical margins, but it has not been consistently assessed in the literature. Herein, we aim to demonstrate the use of intraoperative IRT to detect superficial and deep tumoral margins of low-grade glioma, to identify adjacent functional motor cortex, and to maximize surgical resection.
Case report
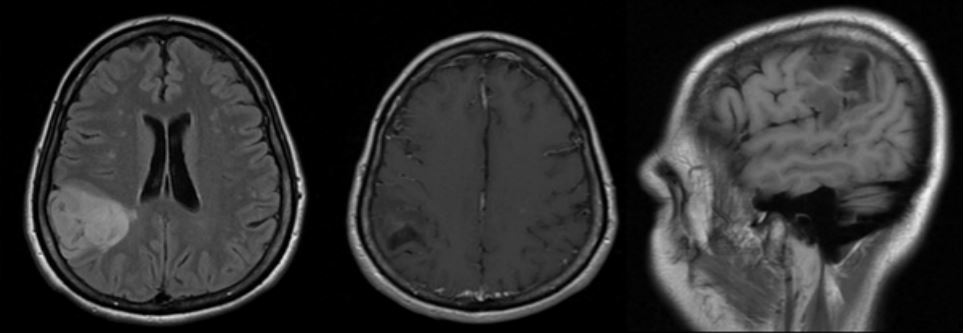
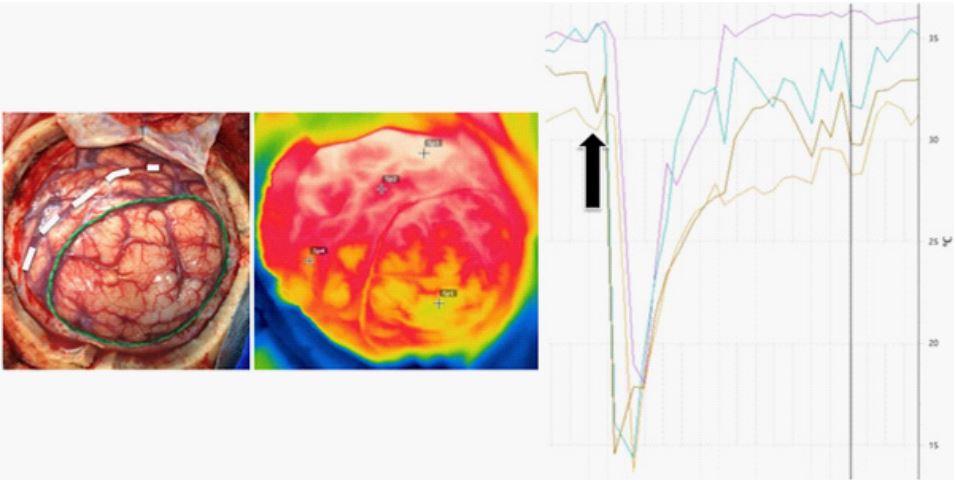
A 45-year-old lady with a long history of partial and secondary generalization seizures was admitted to our department. She experienced an increase in seizure frequency during the last year. Her physical examination was otherwise normal. Magnetic Resonance Imaging (MRI) revealed an expanding lesion located on the right inferior parietal lobule consistent with low-grade glioma (Figure 1). Surgical resection was then recommended. The patient underwent a right fronto-parieto-temporal craniotomy under mild sedation (dexmedetomidine plus remifentanil) and local anesthesia (solution of epinephrine, lidocaine, and bupivacaine) to permit intraoperative brain mapping [11]. After dural opening, the FLIR Systems’ SC620 thermal camera (FLIR Systems, USA) was brought to the surgical field (30-50 cm) to record tumor thermal profile before tumor resection and during voluntary motor tasks. The camera was attached to a tripod to prevent camera mobilization and positioned perpendicular to the exposed brain for spontaneous and sequential digital imaging. SC620 uses a 640x480 pixels detector with thermal sensitivity of 0.02°C. Before image acquisition, the camera was set with operating room and patient temperature, humidity, and distance from the exposed brain. Surgical lights were redirected from the surgical field during infrared measurements. Spontaneous infrared emissions were taken as baseline images. Then, tumor margins at the cortical surface were outlined with neuronavigation and ultrasound and a silk thread was placed over the cortex of the affected area. Thermal gradients revealed tumoral hypothermia (range, 1.7 to 3.9o C) in comparison to the surrounding cortex. Sequential digital images were obtained with irrigation-induced hypothermia as described by Gorbach et al. with slight modifications [12]. Uniform irrigation with saline at room temperature caused abrupt hypothermia of the exposed cortex and created a recovery gradient, which can detect tumoral from nontumoral tissues. The effect was most prominent by analyzing the recovery curves (Figure 2). Approximately 140 images were obtained at intervals of 1 second (1 frame per second [fps]) starting 10-15 seconds before irrigation and continued for 1 minute thereafter.
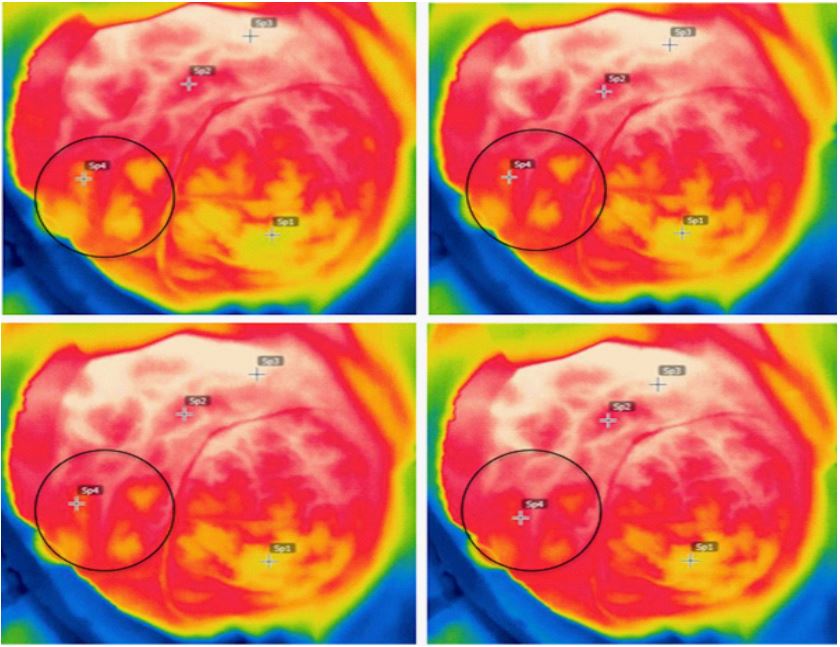
Motor tasks comprised serial finger tapping initiated 10-15 seconds after the beginning of infrared imaging acquisition and lasted 10-15 seconds, also at 1 FPS. Repetitive motor tasks elicited temperature increase in the primary somatosensory cortex mainly dependent on augmented pial vascularization, which was confirmed by mapping (Figure 3). We used bipolar electrodes with a stimulus from 1.5 mA increased to a maximum of 8.0 mA until the neurological function was established. The stimulator device delivered biphasic waves of constant current in 4-s trains at 60 Hz (Leal) [11]. No stimulation-induced seizure was documented. Spatial cognition mapping was additionally performed, but not confirmed with IRT.
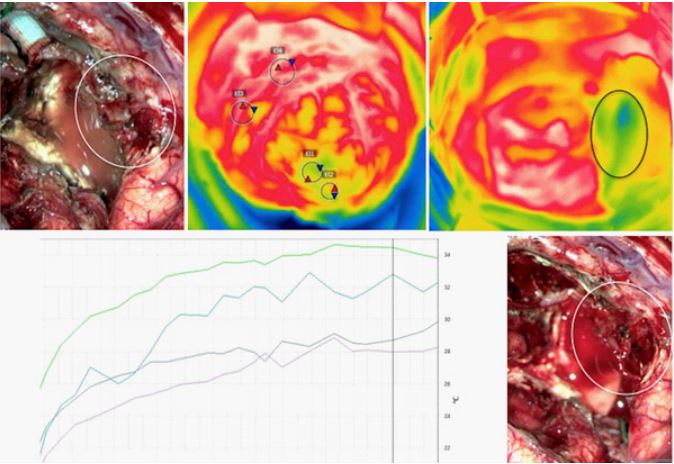
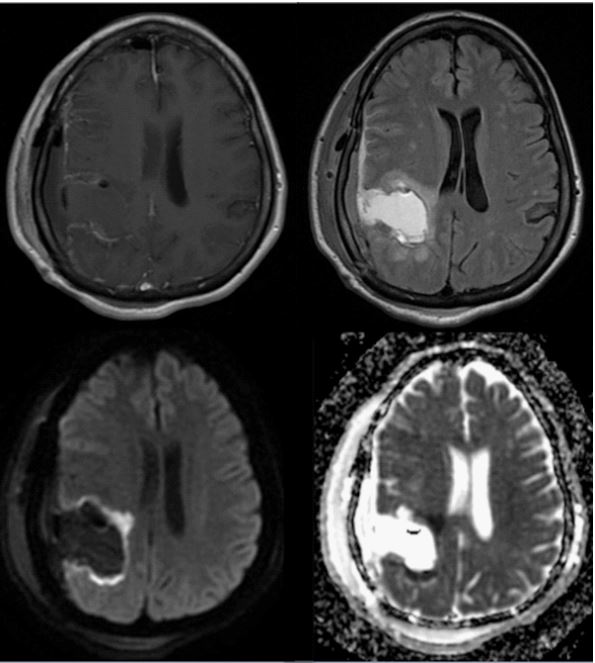
Surgical resection was taken to the anatomical and functional boundaries both in cortical and subcortical levels with the help of brain mapping. When resection was deemed complete by the surgical team, the thermal camera was positioned again for spontaneous and sequential infrared imaging using the same protocol. After resection, the temperatures at the tumor bed and the posterior/inferior margins were cooler than the surrounding cortex. Irrigation-induced thermal gradients revealed suspicion areas of late temperature recovery in comparison to the exposed cortex (Figure 4). So, some samples were taken from these areas for frozen sections. Histologic examination confirmed residual tumor cells and resection was expanded in such proven areas. The patient experienced an uneventful postoperative recovery with no functional deficits. Postoperative MRI demonstrated complete resection of the tumor. Also, areas of restricted diffusion at the tumor bed were identified without clinical correlates (Figure 5). Histopathological analysis confirmed the diagnosis of an oligodendroglioma WHO grade II. The patient provided informed consent for the publication of this manuscript.
Discussion
Currently, intraoperative imaging methods mainly include neuronavigation, intraoperative MRI, intraoperative ultrasound, and fluorescence-guided surgery [13,14]. Imaging methods are largely based on the anatomical characteristics of the brain and CNS tumors, while fluorescence methods depend on the degree of contrast uptake by tumor cells [14,15]. The location of relevant functional areas and the dynamic changes in Cerebral Blood Flow (CBF) in tumors and adjacent brain tissue are characteristics not evaluated by any of the abovementioned methods [12,14]. The application of IRT for the analysis of temperature gradients in brain tissue has been previously studied in experimental models and humans [12]. The first intraoperative description of IRT use in brain tumors was made in 1987 by Koga and colleagues [16]. Since then, IRT has been predominantly used for tumor location and prediction of histological diagnosis [12,14,18].
In 2003, Gorbach and colleagues hypothesized that it would be possible to identify cortical activation through the use of high-resolution infrared imaging as a consequence of local changes in CBF induced by increased metabolism due to motor or language tasks. They concluded that the distribution observed in infrared mapping matched perfectly with the complex distribution of the cortical representation obtained with brain mapping. In this way, IRT could be an extremely useful tool for studying intraoperative brain functions. Temperature increase in the functional cortex was generally mild (0.04-0.08o C), though [17].
Kateb and colleagues were the first to apply IRT to estimate the degree of tumor resection in a patient with metastatic melanoma. Postoperative MRI revealed subtotal resection, which was not identified in their final thermographic image [19]. Our study is unique since we were able to identify primary somatosensory cortex temperature changes as a result of motor tasks with a greater temperature range than previously demonstrated by using a thermal camera with twice the resolution. Also, surgical resection was expanded by identifying residual tumors in the area of late recovery of the thermal maps after irrigationinduced hypothermia. IRT might have several advantages over the aforementioned intraoperative imaging methods since it is cost-effective, non-invasive, and allows localization of subcortical tumors [18,19].
Conclusion
During the last 30 years, intraoperative IRT has been mostly used for diagnostic purposes in brain tumors. The study of the vascular relationships of brain tumors and the impact on the maximization of surgical resection have been poorly addressed in the literature. Our study demonstrates the application of IRT in the detection of surgical margins and functional areas during low-grade glioma resection suggesting its utility as an additional method for maximizing surgical resection while preserving function. Our findings lend support to future investigations in the field.
Declarations
Conflict of interest: All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Ethical approval: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent: Informed consent was obtained from all individual participants included in the study.
References
- Ferracci F-X, Duffau H. Improving surgical outcome for gliomas with intraoperative mapping. Expert Rev Neurother. 2018; 18(4): 333-341. doi:10.1080/14737175.2018.1451329.
- Brown TJ, Brennan MC, Li M, et al. Association of the Extent of Resection With Survival in Glioblastoma: A Systematic Review and Meta-analysis. JAMA Oncol. 2016; 2(11): 1460. doi:10.1001/jamaoncol.2016.1373.
- Brown TJ, Bota DA, van Den Bent MJ, et al. Management of lowgrade glioma: a systematic review and meta-analysis. NeuroOncol Pract. 2019; 6(4): 249-258. doi:10.1093/nop/npy034.
- Yordanova YN, Duffau H. Supratotal resection of diffuse gliomas – an overview of its multifaceted implications. Neurochirurgie. 2017; 63(3): 243-249. doi: 10.1016/j.neuchi.2016.09.006.
- De Witt Hamer PC, Robles SG, Zwinderman AH, Duffau H, Berger MS. Impact of Intraoperative Stimulation Brain Mapping on Glioma Surgery Outcome: A Meta-Analysis. J Clin Oncol. 2012; 30(20):.2559-2565. doi:10.1200/JCO.2011.38.4818.
- Clavreul A, Aubin G, Delion M, Lemée J-M, Ter Minassian A, Menei P. What effects does awake craniotomy have on functional and survival outcomes for glioblastoma patients? J Neurooncol. 2021; 151(2): 113-121. doi:10.1007/s11060-020-03666-7.
- Gerritsen JKW, Klimek M, Dirven CMF, et al. The SAFE-trial: Safe surgery for glioblastoma multiforme: Awake craniotomy versus surgery under general anesthesia. Study protocol for a multicenter prospective randomized controlled trial. Contemp Clin Trials. 2020; 88: 105876. doi: 10.1016/j.cct.2019.105876.
- Stepp H, Stummer W. 5‐ALA in the management of malignant glioma. Lasers Surg Med. 2018; 50(5): 399-419. doi:10.1002/lsm.22933.
- Acerbi F, Cavallo C, Broggi M, et al. Fluorescein-guided surgery for malignant gliomas: a review. Neurosurg Rev. 2014; 37(4): 547-557. doi:10.1007/s10143-014-0546-6.
- Almekkawi AK, El Ahmadieh TY, Wu EM, et al. The Use of 5-Aminolevulinic Acid in Low-Grade Glioma Resection: A Systematic Review. Oper Neurosurg. 2020; 19(1): 1-8. doi:10.1093/ons/opz336.
- Leal RTM, da Fonseca CO, Landeiro JA. Patient’s perspective on an awake craniotomy for brain tumors—single-center experience in Brazil. Acta Neurochir (Wien). 2017; 159(4): 725-731. doi:10.1007/s00701-017-3125-0.
- Gorbach AM, Heiss JD, Kopylev L, Oldfield EH. Intraoperative infrared imaging of brain tumors. J Neurosurg. 2004; 101(6): 960-969. doi:10.3171/jns.2004.101.6.0960.
- Barone DG, Lawrie TA, Hart MG. Image guided surgery for the resection of brain tumors. Cochrane Gynaecological, Neuro-oncology and Orphan Cancer Group, ed. Cochrane Database Syst Rev. Published online. 2014. doi: 10.1002/14651858.CD009685.pub2.
- Ecker RD, Goerss SJ, Meyer FB, Cohen-Gadol AA, Britton JW, Levine JA. Vision of the future: initial experience with intraoperative real-time high-resolution dynamic infrared imaging: Technical note. J Neurosurg. 2002; 97(6): 1460-1471. doi:10.3171/jns.2002.97.6.1460
- Kastek M, Piatkowski T, Polakowski H, et al. Intraoperative application of thermal camera for the assessment of during surgical resection or biopsy of human’s brain tumors. In: Colbert FP, Hsieh S-J (Tony), eds; 2014: 910508. doi: 10.1117/12.2050306.
- Koga H, Mori K, Ono H, Kuwahara M, Matsuse E. [Intraoperative regional thermography during surgery of brain tumors]. Neurol Med Chir (Tokyo). 1987; 27(11): 1033-1038. doi:10.2176/nmc.27.1033.
- Gorbach AM, Heiss J, Kufta C, et al. Intraoperative infrared functional imaging of human brain. Ann Neurol. 2003; 54(3): 297-309. doi:10.1002/ana.10646.
- Naydenov E, Minkin K, Penkov M, Nachev S, Stummer W. Infrared Thermography in Surgery of Newly Diagnosed Glioblastoma Multiforme: A Technical Case Report. Case Rep Oncol. 2017; 10(1): 350-355. doi:10.1159/000470832.
- Kateb B, Yamamoto V, Yu C, Grundfest W, Gruen JP. Infrared thermal imaging: A review of the literature and case report. NeuroImage. 2009; 47: 154-162. doi: 10.1016/j.neuroimage.2009.03.043.