
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Extra nasopharyngeal angiofibroma: A deviant clinical presentation of angiofibroma
Sheelia Ouseph*; Kranti Bhavana; Arun Srinivaasan S; Bhartendu Bhart
Department of ENT, AIIMS, Patna, India.
*Corresponding Author : Sheelia Ouseph
Department of ENT, AIIMS, Patna, India.
Tel: +91 9745915069.
Email: sheelia.ouseph@gmail.com
Received : Feb 08, 2024
Accepted : Mar 14, 2024
Published : Mar 21, 2024
Archived : www.jcimcr.org
Copyright : © Ouseph S (2024).
Abstract
Nasopharyngeal angiofibroma is a benign vascular locally aggressive lesion that arises from a hamartomatous nidus, with nasopharynx being the most common and earliest site of presentation. However deviance to such presentation have been reported although rare, such as turbinates, nasal septum and retroantral space.
Classical nasopharyngeal angiofibroma routinely presents with chief complaints of nasal obstruction and characteristic painless, recurrent and spontaneous epistaxis with choanal banking effect.
Our case depicts the unique and rare presentation of angiofibroma as a progressive cheek swelling in an adolescent male without any nasal symptoms. Diagnostic nasal endoscopy revealed a normal bilateral nasal cavity and nasopharynx. Contrast Enhanced Computed Tomography (CECT) of PNS and face aided the diagnosis. Complete surgical clearance was achieved post embolization via maxillary swing approach. Diagnosis was confirmed on histopathology. Extra nasopharyngeal angiofibroma may be a rare entity however must be considered as a differential diagnosis in vascular skull base tumours.
Keywords: Angiofibroma; JNA; Extra nasopharyngeal angiofibroma; Skull base surgery; Vascular tumours; Maxillary swing approach.
Citation: Ouseph S, Bhavana K, Srinivaasan SA, Bharti B. Extra nasopharyngeal angiofibroma: A deviant clinical presentation of angiofibroma J Clin Images Med Case Rep. 2024; 5(3): 2935.
Introduction
Angiofibroma are rare benign locally aggressive vascular tumours accounting for 0.5% of all head and neck neoplasms [1,2]. The tumour predominantly affects adolescent males, with nasopharynx being the most common site of presentation. The tumour being highly vascular, locally invasive and its proximity to skull base often proposes a surgical challenge. Angiofibroma located outside nasopharynx are extremely rare. They often have variety of presentations and can often be misdiagnosed. This case report discusses in detail about an adolescent male who presented with extra nasopharyngeal angiofibroma. Etiology of JNA is still unclear.
Pathogenesis and genetics
Osborn in 1959 suggested that the tumour may be a hamartoma or a growth of lower erectile tissue hormonal stimulation. Girgis and Fahmy regard the tumour as a paraganglioma based on the history of isolated epithelioid cells at the edges of JNA. Schick et al suggested that JNA represents the growth of the remaining plexus of arteries from the impact of the first branchial artery [3,4]. JNA is on the verge of promoting growth during adolescence. This may explain the temporary vascular contribution from the internal carotid artery. One theory holds that JNA derives from a steroid-stimulated hamartomatous turbinate, which will explain the natural effects of JNA after puberty. To date, the widely accepted view of the JNA genesis appears to be the result of repeated episodes of microhaemorrhages and correction by tissue formation in the sphenopalatine foramen, rich in erectile glandular tissue that is scattered due to increased production of sex hormones during adolescence in formation [4]. Among the various theories proposed recent years have seen the evidence of genetic factors in etiopathogenesis. The factor of male sex predominance, spontaneous regression and recurrences indicate a potential genetic mechanism in its etiopathogenesis. Studies by Shick et al. and Heinrich et al. suggested the evidence of chromosomal imbalances, specifically the increase of chromosomal regions X, 4q, 6q, 8q, 12 and losses at Y, 17 and 22q [3,5]. They evidently supported the chromosomal imbalance between endothelial cells and stromal markers. Supportive evidence of the role of C-myc oncogenes, Kit proto-oncogene receptor tyrosine kinase (c-kit) and frameshift mutations in β – catenin binding region of APC gene have been confirmed [5]. Molecular alterations are significant in pathogenesis of JNA. Angiogenesis activators like Vascular Endothelial Growth Factor (VEGF) is currently the most potent growth factor in JNA5. Recent studies have shown a second potent angiogenic factor after VEGF as basic Fibroblast Growth Factor (bFGF), supporting the possible targeted therapy in JNA population.
Site of origin
The proposed various sites of origin of JNA include the pterygoid wedge, sphenopalatine foramen or pterygopalatine fossa, nasopharynx. While those angiofibroma appearing outside the nasopharyngeal pterygopalatine fossa and its surrounding tissue are referred to extra nasopharyngeal angiofibroma. It has been acknowledged as an extremely rare and different entity, although they are histologically similar to JNA.
Case presentation
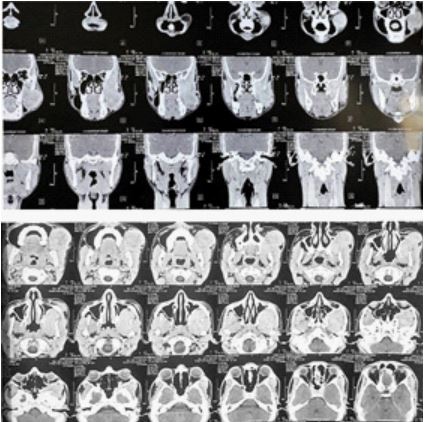
A 20-year-old male was referred to our centre with chief complaints of left sided cheek swelling for the past one and a half years. Patient had complaints of gradually progressive cheek swelling that was referred to our centre, with an FNAC report from the swelling that was suggestive hemangioma. Patient underwent thorough clinical and radiological evaluation. Clinical examination revealed a soft compressible non tender swelling of left cheek, approx. 8x6 cm, globular in shape, with smooth surface, well defined margins and not fixed to overlying skin. Intra oral examination revealed fullness of left gingiva buccal sulcus with bulging of left buccal mucosa. The overlying buccal mucosa appeared normal. Nasal endoscopy was performed which appeared normal. The contrast enhanced computed tomography of face revealed a solid vascular lesion involving the left masticator space and buccal space with superolateral extension to involve the temporalis muscle, anteriorly, bulging into left maxillary sinus causing anterior bowing of the posterolateral wall of maxillary sinus and obliteration of right retro maxillary space. Medially, the lesion was extending into the sphenopalatine foramen, inferolaterally the lesion is extending into left cheek region via retromolar trigone and inferomedially it is bulging into oral cavity, compressing the left buccinators muscle, with no evidence of bone erosion. The working diagnosis was concluded to be extra nasopharyngeal angiofibroma and the patient was planned for surgical resection and biopsy.



Discussion
Angiofibroma is a locally invasive benign vascular neoplasm, occurring most commonly in nasopharynx, predominantly involving adolescent males [6]. Primary tumours can classical present as dumbbell tumours involving the nasopharynx, sphenoid sinus, pterygopalatine fossa, infratemporal fossa with the constriction at the sphenopalatine foramen. Early Stage 1 tumors can exclusively present as a nasopharyngeal mass alone. Extra nasopharyngeal angiofibroma, histologically similar to nasopharyngeal angiofibroma is known for its rarity and varying origins and clinical presentation [1,2]. Classically patient with nasopharyngeal angiofibroma present with complaints of nasal obstruction and painless recurrent spontaneous epistaxis as the chief complaints with additional symptoms depending upon the extent into the orbit, buccal space and intracranial involvement. However, in our case, the patient had only a progressively increasing cheek swelling without other symptoms, making it grossly difficult to postulate extra-nasopharyngeal angiofibroma as a differential diagnosis. However, the subsequent good radiological imaging aided to the diagnosis. The sites of presentation of these angiofibroma makes it difficult at times, to achieve a complete pre-operative embolization.
The origin of these tumours have been most disputed, recently many theories have been postulated that includes hormonal sensitivity of the tumour, pathogenic β catenin mutations among other theories [2,5,7]. The eccentric nature of extra nasopharyngeal tumour in terms of its varied locations and presentations have been attributed to migration error of fascia basalis, supporting its heterogeneity of locations [1,5]. The most common site of extra nasopharyngeal angiofibroma was maxillary sinus, while other sites included cheek, inferior turbinate and septum. The diagnostic delay owing to its rarity and the origin site, can be avoided with heightened index of suspicion and clinical acumen. Treatment of choice is surgical excision. Various open surgical approaches preferred include lateral rhinotomy by Moure’s incision, Weber – Fergusson incision and midfacial degloving, based on extent and involvement of tumour. The new endoscopic instruments can be combined with open approach for better surgical clearance and as an aid for optimised visualisation. The extra nasopharyngeal location of the tumour usually facilitates complete and wide local excision of tumour in comparison to JNA where residual cell rests can be remaining. Tumour recurrent rates have been attributed to be 6% to 27% in nasopharyngeal angiofibroma, but extra nasopharyngeal tumour usually does not recur owing to its location that facilitates total resection [1].
Conclusion
The significance of our case report lies in the rarity of the origin of angiofibroma and the varying nature of its presentation. Extra nasopharyngeal angiofibroma should be considered a differential diagnosis among the vascular skull base tumours.
Surgical consideration: Patient underwent pre-operative Digital subtraction angiography and pre-operative tumour embolization. DSA revealed a hyper vascular tumour supplied by multiple branches of left External Carotid artery. Tumour embolization performed using PVA particles and coils and complete devascularization was achieved, with parent artery remaining patent, post procedure. The patient underwent open surgical resection of the tumour under GA in supine position via Left Maxillary swing approach with a Weber Fergusson incision–36 hours post tumour embolization. The osteotomies were performed, tumour was released from surrounding structures via blunt dissection and delivered in toto. The tumour had extension into the deep temporal space, ITF, masticator space and seen inferiorly extending up to buccal space. The specimen was sent for histopathological examination post operatively which was confirmatory of angiofibroma.
Declarations
Conflict of interest: None.
Acknowledgement: This is a non-funded non supported academic article. Would like to thank the entire team of department of ENT, Radiodiagnosis team, Anaesthesia and critical care team members of AIIMS Patna.
References
- Correia FG, Simões JC, Mendes-Neto JA, de Seixas-Alves MT, Gregório LC, Kosugi EM. Extranasopharyngeal angiofibroma of the nasal septum - uncommon presentation of a rare disease. Brazilian Journal of Otorhinolaryngology. 2013; 79(5): 646.
- Amini-Salari A, Glomski K, Ahn D, Tannyhill RJ. Mandibular Intraosseous Angiofibroma—A Rare Clinical Entity. Journal of Oral and Maxillofacial Surgery. 2020; 78(8): 1343-8.
- Schick B, Plinkert PK, Prescher A. [Aetiology of Angiofibromas: Reflection on their Specific Vascular Component]. Laryngorhinootologie. 2002; 81(4): 280-4.
- Alshaikh NA, Eleftheriadou A. Juvenile Nasopharyngeal Angiofibroma Staging: An Overview. Ear Nose Throat J. 2015; 94(6): 12-22.
- Li W, Ni Y, Lu H, Hu L, Wang D. Current perspectives on the origin theory of juvenile nasopharyngeal angiofibroma. Discov Med. 2019; 27(150): 245-54.
- Kim HD, Choi IS. Extranasopharyngeal angiofibroma mimicking choanal polyp in patients with chronic paranasal sinusitis. Auris Nasus Larynx. 2019; 46(2): 302-5.
- Garcia-Rodriguez L, Rudman K, Cogbill CH, Loehrl T, Poetker DM. Nasal septal angiofibroma, a subclass of extranasopharyngeal angiofibroma. American Journal of Otolaryngology. 2012; 33(4): 473-6.