
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
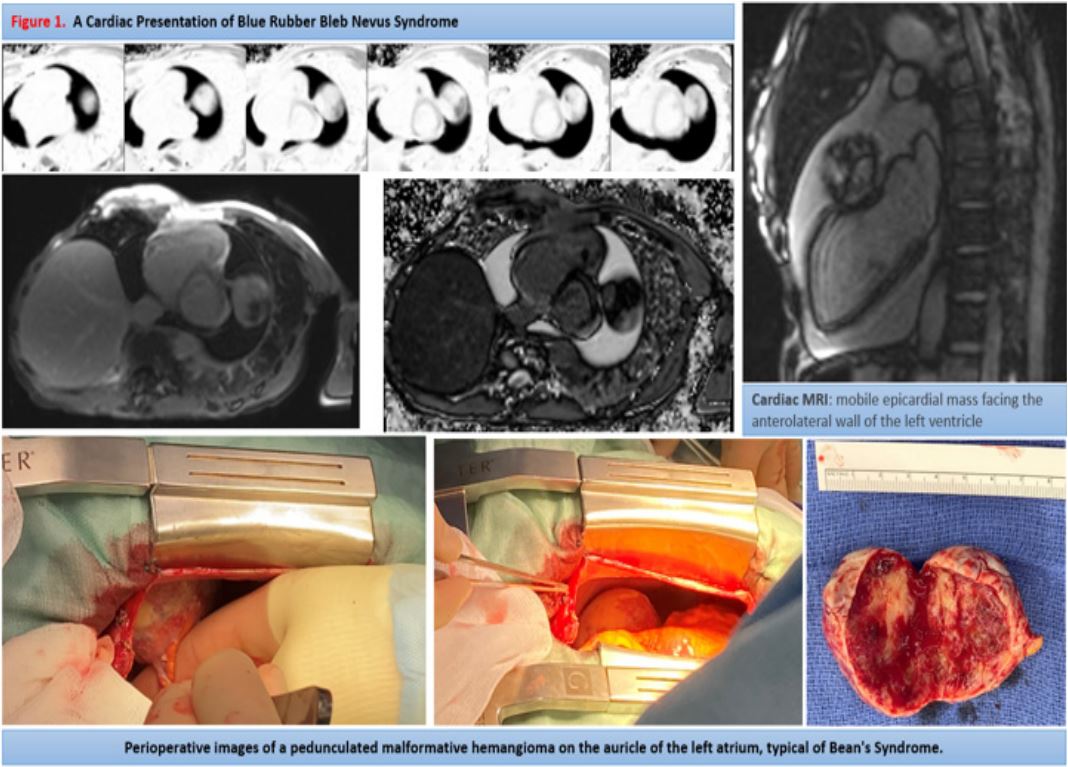
A cardiac presentation of Blue Rubber Bleb Nevus Syndrome
Scopetani G*; Anafack J; Kirsch M
Department of Cardiovascular Surgery, CHUV, Lausanne University Hospital, Lausanne, Switzerland.
*Corresponding Author : Scopetani G
Department of Cardiovascular Surgery, CHUV, Lausanne University Hospital, Lausanne, Switzerland.
Email: giulia.scopetani@chuv.ch
Received : Feb 28, 2024
Accepted : Mar 15, 2024
Published : Mar 22, 2024
Archived : www.jcimcr.org
Copyright : © Scopetani G (2024).
Citation: Scopetani G, Anafack J, Kirsch M. A cardiac presentation of Blue Rubber Bleb Nevus Syndrome. J Clin Images Med Case Rep. 2024; 5(3): 2937.
Description
Blue rubber bleb nevus syndrome (BRBNS) is a rare condition, who is characterized by numerous venous malformations in the skin and viscera, particularly in the gastrointestinal tract. The exact etiology of this syndrome is unknown, but on a molecular level, the elevated expression of c-kit has been demonstrated [1]. Cardiac involvement is not described in the literature.
We report a case of a 56-year-old patient, known for BRBNS, with multiple venous malformations, mainly in the head and neck. She has been followed for years for intracardiac and pericardial masses on the rise. She was admitted to our center to drain a pericardial effusion in augmentation. At the opening of the pericardium we drain 500 ml of serous liquid. We observed several epicardial vein malformations like ‘’Blue Rubber Bleb Naevus‘’ along the right ventricle infundibulum and several adventitial lesions on the ascending aorta. At exploration, we discover a pediculated mass on the auricle of the left atrium. The pedicle is clamps, ligatured with a Prolene 4.0, then the mass is excised (Figure 1).
The procedure was performed on a patient with the BRBNS that does not respond to treatment with Siverolimus, considered as the first-line therapy [2,3]. The intracardiac masses did not cause obstruction and we left them on site. The pericardial mass was the cause of the reactive pericardial effusion.
We herein report an extremely rare case of the combination of blue rubber bleb nevus syndrome with cardiac involvement. With our intervention we have avoided an urgent intervention for cardiac tamponade, but the pericardial effusion will continue to form if the patient will remain unresponsive to the only treatment known for this rare syndrome.
References
- Soblet J, Kangas J, Nätynki M, et al. Blue rubber bleb nevus (BRBN) syndrome is caused by somatic TEK (TIE2) mutations. J Invest Dermatol. 2017; 137: 207-16.
- Xin Lin Wong et al. Sirolimus in blue rubber bleb naevus syndrome: A systematic review. Journal of Paediatrics and Child Health. 2019; 55: 152-155.
- Bevacqua, M., Baldo, F., Pastore, S. et al. Off-Label Use of Sirolimus and Everolimus in a Pediatric Center: A Case Series and Review of the Literature. Pediatr Drugs. 2019; 21: 185-193.