
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Case report: Klebsiella oxytoca aortitis
Abed Al Hadi Krisht1*; Remi Espenel1; Claire Dupuis1,2; Bertrand Souweine1,3
1Medical Intensive Care Unit, University Hospital Gabriel Montpied, 63000, Clermont-Ferrand, France.
2Unit of Human Nutrition, CRNH Auvergne, INRAe, University of Clermont Auvergne, 63000, Clermont Ferrand, France.
3University of Clermont Auvergne, UMR CNRS 6023 LMGE, 63000, Clermont-Ferrand, France.
*Corresponding Author : Abed Al Hadi Krisht
Medical Intensive Care Unit, University Hospital Gabriel Montpied, 63000, Clermont-Ferrand, France.
Email: dr.hadi.kresht@gmail.com
Received : Feb 27, 2024
Accepted : Mar 19, 2024
Published : Mar 26, 2024
Archived : www.jcimcr.org
Copyright : © Krisht AAH (2024).
Abstract
Background: Aortitis is the inflammation of the aorta wall secondary to infectious and non-infectious etiologies. It is a rare but potentially life-threatening condition.
Case Presentation: A 86-year-old diabetic male patient, treated by metformin, was admitted to the Intensive Care Unit (ICU) for septiccardiogenic shock, acute kidney injury, severe hyperkalemia and lactic acidosis. He was administered systemic antibiotics with cefotaxime and aminoglycosides, fluid resuscitation, vasopressor therapy and hemodialysis. A transthoracic echocardiography showed a pericardial effusion with cardiac tamponade. Pericardial drainage was performed in emergency at the bedside resulting in hemodynamic improvement. A chest angio-CT scan showed a false aneurysm of the horizontal aorta and a periaortic collection containing bubbles with peripheral enhancement. Cardiovascular surgery and endovascular aortic stenting were not carried out because of the patient’s frailty, advanced age and patient’s will for end-of-life care. Pericardial fluid culture yielded wild type Klebsiella oxytoca. Systemic antibiotics were continued.
Conclusion: We reported a septic-cardiogenic shock associated with cardiac tamponade and infected aortitis with mycotic aneurysm due to klebsiella Oxytoca. The CT imaging and cultures are the cornerstone of diagnosis. Antibiotic therapy and surgery are crucial and must be discussed to improve the very poor prognostic of the patients.
Keywords: Aortitis; Klebsiella; Intensive care; Case report.
Citation: Krisht AAH, Espenel R, Dupuis C, Souweine B. Case report: Klebsiella oxytoca aortitis. J Clin Images Med Case Rep. 2024; 5(3): 2943.
Introduction
Aortitis is the inflammation of the aorta wall secondary to infectious and non-infectious etiologies. It is a rare but potentially life-threatening condition, but its actual incidence may be underestimated. Infectious aortitis may be localized to isolated aortic segments but may involve the entire length of the vessel. It is more common among older patients with preexisting comorbidity, clinical presentation is often unspecific depending on the site of the infection, sepsis severity, aneurysm evolution and rupture. Early diagnosis and prompt management is mandatory to prevent fatal outcome. We present the case of an elderly patient admitted to the hospital with a septic and cardiogenic shock associated with cardiac tamponade, and infected aortitis with mycotic aneurysm with documented infection with Klebsiella oxytoca. To our knowledge, such a clinical presentation has been previously reported but not with K. Oxytoca pericarditis associated with infectious aortitis.
Case presentation
A 86 years old patient with history of diabetes mellitus type II, benign hypertrophy of prostate, treated with metformin, visited the general practitioner for asthenia, lethargy and anorexia of few days duration without fever, associated with hypotension 90/60 mmHg. Azithromycin was prescribed by GP for possible bronchitis with bacterial superinfection. Blood laboratory tests revealed a leukocytosis (14 G), elevated serum values of proBNP 1875 µg/l and of troponin 22 ng/l, and other laboratory data were unremarkable. Two days later, the patient was referred to the emergency department because of a systolic blood pressure of 60 mmHg. At hospital admission, physical examination showed hypotension: 70/45 mmHg, hypothermia (35.6°C); heart rate was 75 bpm; respiratory rate, 27 /min; coma Glasgow scale, 15. He presented mottling of the knees, cold extremities, jugular turgescence, muffled heart sounds; but a bilateral and symmetrical vesicular murmur. The electrocardiogram was in sinus rhythm with ST elevation in lateral leads V4-V5-V6 and lead II. The transthoracic echocardiography showed a pericardial effusion of 18 mm without signs of tamponade. Blood results showed severe lactic acidosis, hyperkalemia and acute kidney injury (Table 1). Crystalloids were given and the patient transferred to the intensive care unit. Upon admission, fluid resuscitation was continued, cefotaxime, spiramicyn, gentamycin, vasopressors administered, and amiodarone begun for new onset atrial fibrillation. A hemodialysis session was started. Because of worsening of the shock, transthoracic echocardiography was performed and displayed large pericardial effusion, right ventricular collapse, and paradoxical septum motion. Bedside echo-guided paracentesis was performed in emergency; 250 cc of pericardial purulent fluid were removed resulting in a significant hemodynamic improvement. A pericardial drain was left in place. The sinus rhythm was restored. Next day, a chest angioCT scan was performed and showed a bulky false aneurysm of horizontal aorta (25 mm) (Figure 1a), and a periaortic collection, measuring 65 mm, containing bubbles with peripheral enhancement (Figure 1b). Cardiovascular surgery and endovascular aortic stenting were not carried out because of the patient’s frailty, elderly age, and expressed wishes. Pericardial fluid, but also urinary cultures yielded wild type K. oxytoca. Spiramycine and gentamycin were stopped, and antibiotics switched to cefotaxime and ofloxacin. A week after, the patient was transferred to the infectious disease department, and three weeks later home discharged in accordance with his end-of-life decisions. Antimicrobial therapy was changed for sulfamethoxazole/trimethoprim and ofloxacin based on antibiogram susceptibilities. He ultimately died at home 7 days later.

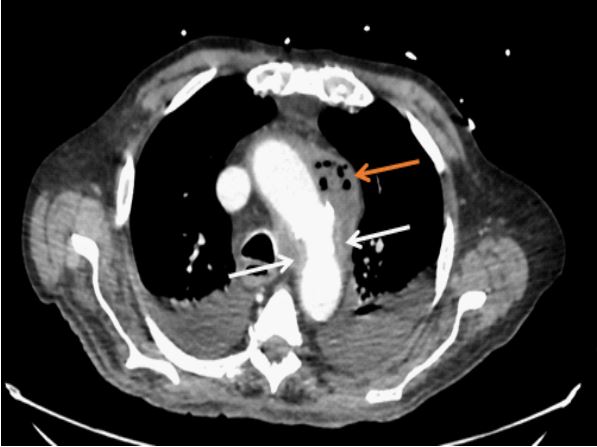
Table 1: Main laboratory features on emergency department admission.
| Lab | Value | Reference range |
|---|---|---|
| WBC | 15.8 | 4.00-10.00 giga/L |
| Hb | 9.9 | 13.0-16.5 g/dl |
| Ht | 29.7 | 36.2-49.0 % |
| MCV | 76.5 | 79.0-97.7 fl |
| Platelets | 161 | 150-400 giga/L |
| INR | 2.7 | |
| PTT | 36 | Seconds |
| Fibrinogen | 6.7 | 2.0-4.0 g/l |
| DDimer | 3991 | <500 ng/mL (FEU) |
| Sodium | 126 | 136-145 mmol/L |
| Potassium | 5.3 | 3.5-5.1 mmol/L |
| Chloride | 90 | 98-107 mmol/L |
| Bicarbonate | 11 | 21-32 mmol/L |
| Anion gap | 30 | 12-16 mmol/L |
| Phosphorus | 3.32 | 0.81-1.58 mmol/L |
| Creatininemia | 287 | μmol/L |
| CRP | 281 | <3 mg/L |
| Procalcitonin | 3.53 |
Severe bacterial
infection, sepsis:>2 μg/L |
| SGOT/SGPT | 7131/3263 | 15-37/ 16-61 U/L |
| Lactate | 11.6 | <1.3 mmol/L |
| Pro-BNP | 1875 | ng/l |
| Troponin | 22 | μg/l |
WBC: White Blood Cell; Hb: Hemoglobin; Ht: Hematocrit; MCV: Mean corpuscular Volume; INR: International Normalized Ratio; PTT: Partial thromboplastin Time.
Discussion
We reported the first case of infective aortitis with pericarditis due to K. oxytoca.
There are many bacteria implicated in infective aortitis. The most prevalent are gram positive cocci including Staphylococcus and Streptococcus. Aortitis secondary to Enterococcus species are most of the time diagnose in the setting of endocarditis. Salmonella-associated aortitis is also commonly seen in individuals with Salmonella enterica serotype Typhi infection, particularly in endemic regions [1]. Less frequently, other gram-negative bacteria, such as Escherichia coli, Klebsiella pneumoniae, and Pseudomonas aeruginosa can also cause infective aortitis, often observed in individuals with risks factors like intravenous drug use or indwelling catheters. Cases of infective aortitis due to P. aeruginosa were commonly reported in hospitalized patients, post cardiothoracic surgery, immunocompromised patients, and donor derived infection with heart transplant.
Our patient exhibited positive cultures in pericardial fluid and urine returned positive for K. oxytoca, making the first reported case of infected aortitis due to K. oxytoca.
K. Oxytoca, a member of the Enterobacteriaceae family, is known for causing a wide range of infections in humans, with the respiratory and urinary tracts being the most common sites of infection [2].
K. Oxytoca is far less prevalent that K. pneumoniae and represent less than 5% of the isolate of klebsiella genus. [3]. K. Oxytoca is an ubiquitous, facultatively anaerobic, Gramnegative bacillus, routinely distinguished from K. pneumoniae by its production of indole. In humans, K. Oxytoca colonizes mucosa membranes, particularly the gastrointestinal tract. K. Oxytoca produces naturally chromosomal β-lactamases, which confer resistance to penicillins. It can acquire several types of resistance, including production of Extended-Spectrum B-Lactamases (ESBLs), AmpC lactamases, Klebsiella Pneumonia Carbapenemase (KPC) and aminoglycosides-modifying enzymes. K. oxytoca can therefore be challenging to treat [4].
K. Oxytoca is associated with virulent factors including tilivalline and kleboxymycin, that play roles as cytotoxins.
K. Oxytoca is a human commensal but also an opportunistic pathogen causing various infections [4]. They can occur in immunocompromised and debilitated ICU patients. Many of them are polymicrobial, hospital-associated and several neonatal and Intensive Care Unit (ICU) outbreaks have been reported [5]. K. Oxytoca has been reported a causative organism of antibioticassociated hemorrhagic colitis [6,8], and more recently, to cause a wide spectrum of severe diseases such as pneumonia, urinary tract infection, soft tissue infection, and septicemia [9]. For instance, K. Oxytoca have been reported as an organism causing pleural infection [10], sepsis with myocardial failure leading to driving to extracorporeal membrane oxygenation [11], liver abscess [12] and acute infectious purpura fulminans [13].
In our patient K. xytoca aortitis was due to a wild strain.
While bacteria are commonly linked to infective aortitis, fungal and atypical bacterial species can also contribute. Antibiotic therapy choice depends on the identified pathogen and its susceptibility. Timely diagnosis and appropriate treatment are crucial to prevent complications and improve patient outcomes.
Various risk factors, such as intravenous drug use, aortic surgery, structural anomalies, and immunocompromised status, increase the likelihood of infective aortitis [14]. In our case, an elderly patient with insulin-dependent diabetes and untreated urinary tract infection developed septicemia and aortitis.
We did a literature review for myopericarditis associated aortitis, and found that the majority of the reported cases are due to systematic inflammatory diseases (non-infectious etiology) except for few cases reported, we mention two of them, the first was the case of 42 year old patient with history of untreated HIV, advanced liver cirrhosis due to chronic hepatitis C infection diagnosed with purulent pericarditis and false aneurysmof ascending aorta with positive blood cultures for methicillin susceptible Staphylococcus aureus. The patient underwent a surgical replacement of ascending aorta with antibiotics coverage for 6 weeks post-op and was discharged home [15] .
The second case was a-79 year old woman on chemotherapy for lung cancer presented with abdominal pain and diarrhea with positive blood cultures positive for Campylobacter fetus. Positron emission tomography was performed and revealed focal hypermetabolism of aortic arch and left ventricle bases with unremarkable echocardiography and cardiac enzymes. The patient underwent surgical repair for rapidly growing aortic aneurysm and antibiotics for 6 weeks, with follow up positron emission tomography scan after 5 months showing no signs of active infection [16].
Management options for infective aortitis include endovascular repair and open surgical procedures, depending on infection extent, complications, patient health, and physician expertise. Endovascular repair offers a less invasive option for select cases, while open surgery is often necessary for extensive infections. In our patient, due to a high surgical risk, a decision was made to transition to comfort care after discussion with the patient and family.
Conclusion
We present a case of aortitis attributed to K. Oxytoca. K. Oxytoca is an emerging virulent pathogen often encountered in Intensive Care Unit (ICU) patients, exhibiting various acquired mechanisms of resistance that can complicate its treatment. Aortitis may manifest with nonspecific clinical symptoms and poses a life-threatening condition. Immediate diagnostic workup, including laboratory investigations, cultures, and, notably, CT imaging, is essential for diagnosing, localizing, and assessing the characteristics of aneurysms, as well as monitoring treatment efficacy.
Once infectious aortitis is identified, prompt initiation of antibiotic therapy and consideration of surgical intervention are crucial. Despite early diagnosis and intervention, the mortality rate remains elevated. Interdisciplinary collaboration plays a pivotal role in the early detection and personalized selection of treatment modalities, providing valuable insights into the patient’s prognosis.
References
- Septimus EJ. Principles and Practice of Infectious Diseases Edited by Gerald L. Mandell, John E. Bennett, and Raphael Dolin. 4th ed. New York: Churchill Livingstone, 1995. 2,803 pp., illustrated. $249.95. Clin Infect Dis. 1995; 20: 1444.
- Zumla A. Mandell, Douglas, and Bennett’s principles and practice of infectious diseases. Lancet Infect Dis. 2010; 10: 303-4.
- Singh L, Cariappa MP, Kaur M. Klebsiella oxytoca: An emerging pathogen? Med J Armed Forces India. 2016; 72: 59-61.
- Yang J, Long H, Hu Y, Feng Y, McNally A, Zong Z. Klebsiella oxytoca Complex: Update on Taxonomy, Antimicrobial Resistance, and Virulence. Clin Microbiol Rev. 2022; 35: 00006-21.
- Liébana-Rodríguez M, Recacha-Villamor E, Díaz-Molina C, PérezPalacios P, Martín-Hita L, Enríquez-Maroto F, et al. Outbreaks by Klebsiella oxytoca in neonatal intensive care units: Analysis of an outbreak in a tertiary hospital and systematic review. Enfermedades Infecc Microbiol Clin Engl Ed. 2023; 2529-993X(23)00157-0.
- Högenauer C, Langner C, Beubler E, Lippe IT, Schicho R, Gorkiewicz G, et al. Klebsiella oxytoca as a causative organism of antibiotic-associated hemorrhagic colitis. N Engl J Med. 2006; 355: 2418-26.
- Zollner-Schwetz I, Högenauer C, Joainig M, Weberhofer P, Gorkiewicz G, Valentin T, et al. Role of Klebsiella oxytoca in antibiotic-associated diarrhea. Clin Infect Dis Off Publ Infect Dis Soc Am. 2008; 47: 74-78.
- Nagamura T, Tanaka Y, Terayama T, Higashiyama D, Seno S, Isoi N, et al. Fulminant pseudomembranous enterocolitis caused by Klebsiella oxytoca: an autopsy case report. Acute Med Surg. 2019; 6: 78-82.
- Heda RP, Savage Y, Nair SP, Verma R. Enterococcus casseliflavus, Streptococcus equinus and Klebsiella oxytoca septicaemia associated with perinephric haematoma in a post-liver transplant patient with allograft cirrhosis. BMJ Case Rep [Internet]. 2019; 12. Available from: https://www.embase.com/search/results?subaction=viewrecord&id=L629123368&from=export.
- Suthers E, Rosenstengel A, Hart J, Lewis JR, Kay I, Waterer G, et al. Pleural empyema caused by Klebsiella oxytoca: a case series. Respirol Carlton Vic. 2015; 20: 507-9.
- Hagiwara S, Murata M, Aoki M, Kaneko M, Oshima K. Septic shock caused by Klebsiella oxytoca: An autopsy case and a survival case with driving Extracorporeal Membrane Oxygenation. Hippokratia. 2013; 17: 171-3.
- Iwadare T, Kimura T, Sugiura A, Takei R, Kamakura M, Wakabayashi S-I, et al. Pyogenic liver abscess associated with Klebsiella oxytoca: Mimicking invasive liver abscess syndrome. Heliyon. 2023; 9: 21537.
- Tsubouchi N, Tsurukiri J, Numata J, Sano H. Acute Infectious Purpura Fulminans Caused by Klebsiella oxytoca. Intern Med. 2019; 58: 1801-2.
- Sidawy AN, Perler BA. Rutherford’s Vascular Surgery and Endovascular Therapy, 2-Volume Set, E-Book. Elsevier Health Sciences. 2022.
- Meier D, Kirsch M, Qanadli SD, Muller O, Fishman D, Trana C. Case report of an unusual combination of purulent pericarditis and false aneurysm of the ascending aorta. J Cardiothorac Surg. 2018; 13: 15.
- Lenherr A, Boughdad S, Prior JO, Lalonde MN, Filippidis P. Infective aortitis and subacute myocarditis due to Campylobacter fetus. Int J Infect Dis IJID Off Publ Int Soc Infect Dis. 2024; 138: 113-4.