
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Gross hydronephrosis secondary to pelviureteric junction structure, complicated with caliceal rupture
Assyifaa Nik Mazian*; Siti Soraya Ab Rahman
Radiology Unit, Faculty of Medicine and Health Sciences, University Sains Islam Malaysia (USIM), Malaysia.
*Corresponding Author : Assyifaa Nik Mazian
Radiology Unit, Faculty of Medicine and Health
Sciences, Universiti Sains Islam Malaysia (USIM),
Malaysia.
Email: nm.syifaa@usim.edu.my
Received : Feb 26, 2024
Accepted : Mar 19, 2024
Published : Mar 26, 2024
Archived : www.jcimcr.org
Copyright : © Mazian AN (2024).
Citation: Mazian AN, Rahman SSA. Gross hydronephrosis secondary to pelviureteric junction structure, complicated with caliceal rupture. J Clin Images Med Case Rep. 2024; 5(3): 2944.
Description
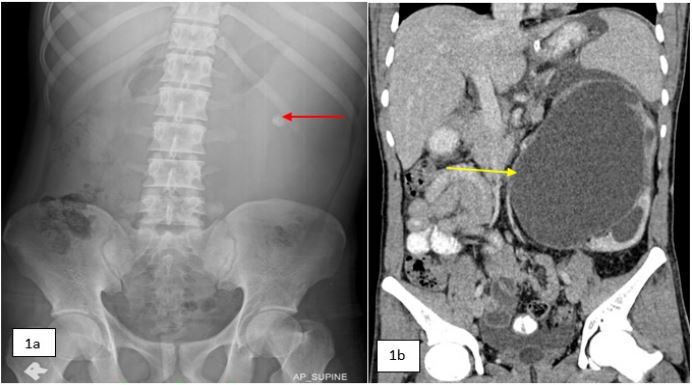
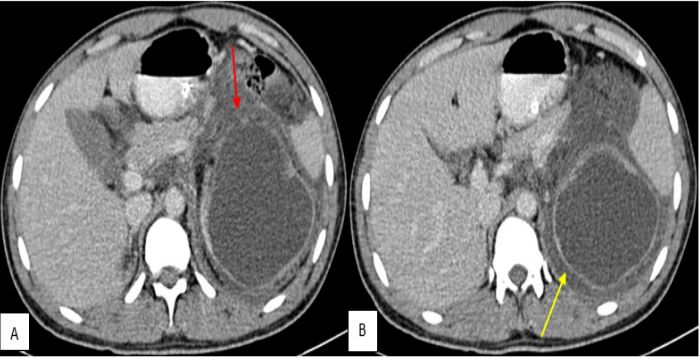
A 23-year-old Myanmar male with previous history of percutaneous nephrolithotomy was presented with acute abdominal pain for 2 days. The pain was pricking in nature and started at left lumbar region and later became generalized. There was no fever, vomiting or history of trauma. The bowel and urinary output were normal. On examination, he was alert and mildly dehydrated. The vital signs were stable. Per abdomen revealed generalized guarding and tender mostly over the left lumbar region. Abdomen radiograph showed left abdominal homogenous opacity with bowel displacement to the right. A round calculus was appreciated at the left lumbar region (Figure 1a). Urgent contrast enhanced CT abdomen revealed gross hydronephrosis with stricture at the left pelviureteric junction (Figure 1b). There was caliceal wall defect at the upper pole calyx (Figure 2a) with perirenal free fluid (Figure 2b). Patient underwent urgent ultrasound-guided left nephrostomy insertion and was discharged well.
Hydronephrosis is dilatation of the renal pelvicalyceal system due to obstruction distal to the renal pelvis. In this case, the obstruction is due to stricture secondary to previous renal surgery. The concurrent renal calculus is non obstructive. Calyceal rupture is a rare complication of obstructive uropathy [1]. A study showed that only 1.9% caliceal rupture were caused by ureteropelvic junction obstruction [2]. In the absence of vascular or abdominal trauma, caliceal rupture can be safely managed non-operatively with resolution greater than 90% [3].
Declarations
Competing interest: The authors have no competing interests to declare.
Funding statement: Not applicable.
Consent: Informed patient consent was obtained.
References
- Mukaya JE, and Waters C. Calyceal rupture and acute renal failure secondary to obstructive uropathy. Consultant. 2016; 56: 1098-1099.
- F Yanaral, A Ozkan, NC Cilesiz, B Nuhoglu. Spontaneous rupture of the renal pelvis due to obstruction of pelviureteric junction by renal stone: a case report and review of the literature. Urol Ann. 2017; 3: 293-295.
- NF Alsikafi, JW McAninch, SP Elliott, M Garcia Nonoperative management outcomes of isolated urinary extravasation following renal lacerations due to external trauma. J Urol. 2006; 176(6): 2494-2497. 10.1016/j.juro.2006.08.015.