
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Atezolizumab-induced encephalitis in a patient with metastatic small cell lung cancer: A clinical case and literature review
Khachaturyan EA*; Pokataev IA; Antonova TG
Department of Health, Moscow State Budgetary Healthcare Institution “City Clinical Oncology Hospital No. 1” of the Moscow, Russia.
*Corresponding Author : Khachaturyan EA
Department of Health, Moscow State Budgetary Healthcare Institution “City Clinical Oncology Hospital No. 1” of the Moscow,
Russia.
Email: dr.elinaonco@mail.ru
Received : Feb 27, 2024
Accepted : Mar 19, 2024
Published : Mar 26, 2024
Archived : www.jcimcr.org
Copyright : © Khachaturyan EA (2024).
Abstract
The emergence of immunotherapeutic drugs for the treatment of cancer has become a breakthrough in the clinical practice of oncologists. Immunotherapeutic drugs include checkpoint inhibitors, cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) inhibitor. However, their widespread use directly correlates not only with the rate of positive responses to therapy, but also with the rate of immune-mediated adverse events. The main mechanism of which is hyperactivation of T lymphocytes.
Citation: Khachaturyan EA, Pokataev IA, Antonova TG. Atezolizumab-induced encephalitis in a patient with metastatic small cell lung cancer: A clinical case and literature review. J Clin Images Med Case Rep. 2024; 5(3): 2945.
Introduction
Atezolizumab is the first and only PDL-1 inhibitor registered in Russia for the treatment of small cell lung cancer, non-small cell lung cancer, metastatic triple-negative breast cancer and hepatocellular carcinoma [1]. Although atezolizumab is the immunotherapeutic agent with the lowest incidence of Immunemediated adverse events, cases of CNS involvement have been reported in the literature [2-4]. Neurological complications of immunotherapy include myasthenia gravis, autonomic neuropathy, aseptic meningitis and encephalitis [5-7]. However, encephalitis induced by atezolizumab therapy is a relatively rare adverse event. In this clinical case, we will look at immune-mediated encephalitis in a patient with metastatic small cell lung cancer.
Clinical case
This clinical case presents a 56-year-old woman diagnosed with stage IV metastatic small cell lung cancer cT2N1M1, who underwent 4 courses of combination therapy according to the regimen Carboplatin AUC5 + Etoposide 100 mg/m2 days 1-3 + Atezolizumab 1200 mg. According to computed tomography data, a large central formation in the left lung is not visualized (previously 46x35 mm), in S10 of the right lung a solitary lesion of 10x11.5 mm is determined. In the peripheral parts of both lungs, polysegmentally, there are zones of consolidation like ground glass. Intrathoracic lymph nodes with a tendency to decrease to 6 mm according to KO (previously 20 mm). Partial response according to RECIST 1.1 criteria Next, the patient received maintenance therapy according to the regimen of Atezolizumab 1200 mg intravenously once every 21 days. A total of 6 courses of maintenance immunotherapy were carried out. On the 2nd day after the 6th course of immunotherapy, the patient’s condition worsened, she noted a constant low-grade fever with episodes of rising to 39C, fever was accompanied by nausea, vomiting and headaches, retrograde amnesia, sudden changes in blood pressure from 70 and 40 mm Hg to 180 and 110 mm. Hg, fainting. The patient was hospitalized in the infectious diseases department.
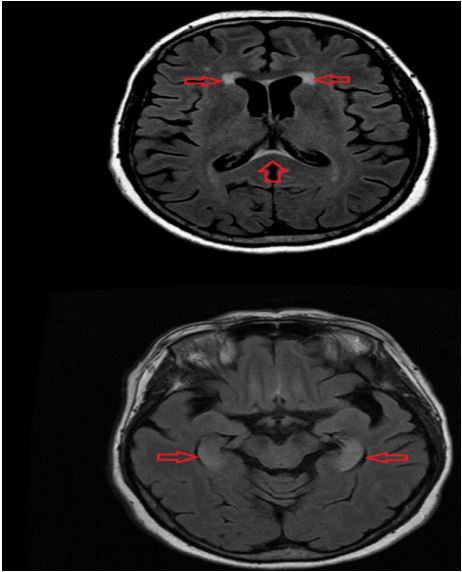
Serological blood test for parvovirus, cytomegalovirus and Epstein-Barr virus is negative, LBC culture of urine and blood is negative. A spinal cord puncture was performed. Clinical analysis of the cerebrospinal fluid showed a slightly increased protein level of 1 g/l (reference 0.22-0.33 g/l), red blood cells 7 ml, cytosis 10.0 (reference 2.0-3.0). According to MRI of the brain with contrast:
Based on the examination, a diagnosis of immuno - mediated limbic encephalitis was made. The patient received pulse therapy with methylprenisolone 1000 mg per day intravenously for 5 days without a positive clinical effect. In this connection, the patient underwent plasmapheresis with positive dynamics - normalization of temperature, blood pressure, partial regression of impaired consciousness. Given the development of grade 3 Immune-mediated adverse events further therapy with Atezolizumab is contraindicated. The patient was transferred to dynamic observation.
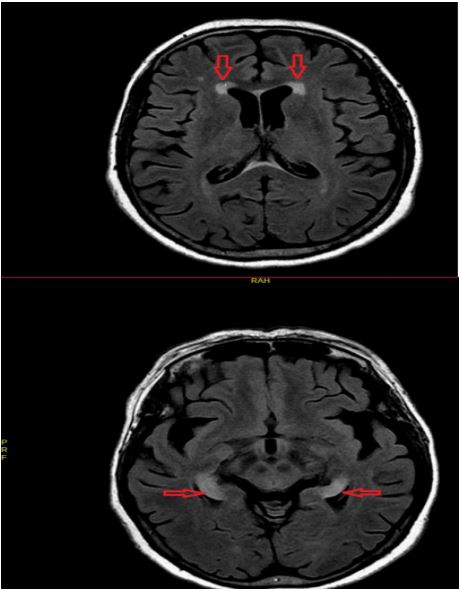
According to the control examination after 3 months: MRI of the brain with IV contrast: no MR signs of pathological changes in the brain were detected at the time of the study. CT scan of the chest, abdomen, and pelvis with IV contrast: In S10 of the right lung, a formation is detected, irregular in shape, with tuberous contours with heterogeneous accumulation of, dimensions 10x14 mm (previously 9x8 mm). Due to the fact that the lesion in the right lung was the only manifestation of the disease. By decision of the oncology council, stereotactic therapy was carried out with positive dynamics. The patient was under dynamic observation. At the time of writing, 15 months have passed since the development of limbic encephalitis. The patient died in February 2023 from decompensated heart failure.
Discussion and conclusions
Immune-mediated damage to the central nervous system is the rarest adverse event and accounts for 2-4%. Of all reported clinical cases, grade 3-4 toxicity occurs in <1%. A review of 59 clinical studies, including more than 9000 patients, showed the following frequency of IONEs: anti-CTL4 (3.8%), antiPD-1 (6.1%), a combination of drugs of these groups (12%) [5]. The literature describes only 4 clinical cases of the development of encephalitis during the administration of Atezolizumab [2-4]. No cases of immune-mediated CNS disease were reported in the phases I and II POPLAR study, but in the phase III OAK study, 5 of 609 patients developed immune-mediated encephalitis [8]. As checkpoint inhibitors are increasingly used in the treatment of cancer, cases of atezolizumab-induced encephalitis will increase and, as we see from the clinical case, this complication does not always respond to high doses of steroids [9]. Based on the above, it is necessary to develop more thorough instrumental and laboratory monitoring in order to timely diagnose immune-mediated damage to the central nervous system.
References
- MA Socinski, RM Jotte, F Cappuzzo, F Orlandi, D Stroyakovskiy, N Nogami, D Rodríguez-Abreu, D Moro-Sibilot, CA Thomas, F Barlesi, G Finley, C Kelsch, A Lee, S Coleman, Y Deng, Y Shen, M Kowanetz, A Lopez‐Chavez, A Sandler, and M Reck. Atezolizumab for First-Line Treatment of Metastatic Nonsquamous NSCLC. The new england journal of medicine. DOI: 10.1056/NEJMoa1716948. nejm.org
- Justin C Kao, Bing Liao, Svetomir N. Markovic, Christopher J Klein, Elie Naddaf, Nathan P Staff, Teerin Liewluck, Julie E Hammack, Paola Sandroni, Heidi Finnes, PharmD, Michelle L. Mauermann. Neurological Complications Associated with Anti–Programmed Death 1 (PD-1) Antibodies. JAMA Neurol. doi: 10.1001/jamaneurol.2017.1912. http://archneur.jamanetwork.com/.
- Jeffrey J. Levine, Robert A. Somer, Hitomi Hosoya, Christian Squillante. Atezolizumab Induced Encephalitis in Metastatic Bladder Cancer: A Case Report and Review of the Literature. Clinical Genitourinary Cancer 1558-7673(17): 30063-0. 10.1016/j.clgc.2017.03.001.
- Filipe Martins, Latifyan Sofiya, Gerasimos P. Sykiotis4, Faiza Lamine, Michel Maillard, Montserrat Fraga5, Keyvan Shabafrouz, Camillo Ribi7, Anne Cairoli, Yan Guex-Crosier, Thierry Kuntzer, Olivier Michielin, Solange Peters, Georges Coukos, Francois Spertini, John A. Thompson and Michel Obeid. Adverse effects of immune-checkpoint inhibitors: epidemiology, management and surveillance. CliniCal OnCOlOgy. 41571-019-0218-0. https://doi.org/10.1038/.
- Ahwon Kim, Bhumsuk Keamb, Hyeon Cheunc, Soon-Tae Leea Hyung Seok Gooka, Moon-Ku Hand. Immune-Checkpoint-Inhibitor-Induced Severe Autoimmune Encephalitis Treated by Steroid and Intravenous Immunoglobulin. Clin Neurol. 2019; 15(2): 259-261. https://doi.org/10.3988/jcn.2019.15.2.259.
- S Cuzzubbo, F Javeri, M Tissier, A Roumi, C Barlog, J Doridam, C Lebbe, C Belin, R Ursu, AF Carpentier. Neurological adverse events associated with immune checkpoint inhibitors: Review of the literature. European Journal of Cancer. 2017; 73: 1-8. http://dx.doi.org/10.1016/j.ejca.2016.12.001.
- Osvaldo Arén Frontera, Filippo De Marinis, Hande Turna, JongSeok Lee, Marcus Ballinger, Marcin Kowanetz, Pei He, Daniel S Chen, Alan Sandler, David R Gandara. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): a phase 3, openlabel, multicentre randomised controlled trial. The Lancet. http://dx.doi.org/10.1016/S0140- 6736(16)32517-X.
- Osvaldo Arén Frontera, Filippo De Marinis, Hande Turna, JongSeok Lee, Marcus Ballinger, Marcin Kowanetz, Pei He, Daniel S Chen, Alan Sandler, David R Gandara. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): a phase 3, openlabel, multicentre randomised controlled trial. The Lancet. http://dx.doi.org/10.1016/S0140- 6736(16)32517-X.
- J. Williams, PhD; David R. Benavides, Kelly-Ann Patrice, MBBS; Josep O. Dalmau, Alexandre Leon Ribeiro de Ávila, Dung T Le, Evan J Lipson, John C Probasco, Ellen M Mowry Association of Autoimmune Encephalitis With Combined Immune Checkpoint Inhibitor Treatment for Metastatic Cancer. JAMA Neurol. doi:10.1001/jamaneurol.2016.1399. http://archneur.jamanetwork.com.