
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Refractory focal epilepsy as a rare clinical presentation of systemic lupus erythematosus
Sachin Sureshbabu1* ; Ashique Hamza2 ; Krishnadas NC3 ; Poornima Narayanan3 ; Deep P Pillai3
1Fellowship in Epilepsy, Fellowship in Sleep Medicine, India.
2General Medicine, DNB General Medicine, Senior Resident, Neurology, India.
3Fellowship in Stroke and Neuro Vascular Interventions from King Edward Memorial Hospital, India.
*Corresponding Author : Sachin Sureshbabu
HOD, Senior Consultant, The Center of Excellence in
Neuroscience, Meitra Hospital, India.
Email: Sachin.s@meitra.com
Received : Feb 29, 2024
Accepted : Mar 21, 2024
Published : Mar 28, 2024
Archived : www.jcimcr.org
Copyright : © Sureshbabu S (2024).
Abstract
Systemic Lupus Erythematosus (SLE) is a chronic autoimmune multisystem disease with prominent neuropsychiatric manifestations. Neuropsychiatric features are seen early in the course of disease with seizures forming one of the most frequent manifestations of Neuro Psychiatric Systemic Lupus Erythematosus (NPSLE). The mechanism of seizure is contemplated to be immune mediated. Both generalised and focal seizures are seen in SLE. They can sometimes be the only symptom marking the onset of disease in the absence of other commonly encountered clinical features of the disease. We report cases of two young females who were diagnosed and treated as drug resistant focal onset seizures with impaired awareness which later turned out to be NPSLE. Both patients showed dramatic response when initiated on immunotherapy. These cases highlight the importance of considering an immune mediated process when a young female presents with pharmacoresistant localisation related epilepsy.
Keywords: Refractory focal epilepsy; Systemic lupus erythematosus (SLE); Autoimmune disorder; Antiepileptic drugs (Aeds).
Citation: Sureshbabu S, Hamza A, Krishnadas NC, Narayanan P, Pillai DP. Refractory focal epilepsy as a rare clinical presentation of Systemic Lupus Erythematosus. J Clin Images Med Case Rep. 2024; 5(3): 2949.
Introduction
Systemic Lupus Erythematosus (SLE) is a multisystem autoimmune disorder with prominent neuropsychiatric manifestations. The prevalence of Neuropsychiatric SLE (NPSLE) is estimated to be between 37% and 95% [1]. Seizures are seen in 2-8% of SLE patients [2]. Seizures can sometimes occur alone as the sole clinical manifestation of NPSLE and usually occur within the first year of diagnosis of SLE [3]. We report two patients who were initially diagnosed and treated as refractory focal epilepsy before they developed other features of SLE.
Case report
Case 1: A 22-year-old female presented with 6-year history of episodes of nausea, abnormal breathing and hypersalivation followed by tonic seizures involving all limbs and altered consciousness. These events lasted around 2 minutes and occurred usually at night with a frequency of 3 episodes per day. Neurological examination was normal. She was initially evaluated and treated as a case of focal onset epilepsy . However, she showed poor response to multiple Antiepileptic Drugs (AED). Interictal Video Electroencephalogram (EEG) showed focal slowing and occasional sharp waves in the left anterior temporal region. (Supplementary file 1) The clinical event was characterised by sudden arousal from sleep, retching sensation, attempt to cover her mouth with the left hand and suggestion of left upper limb automatisms. (Video 1) Ictal EEG was not very contributory except for some fast activity in the midline channels. (Supplementary file 1) Primary hypothesis was an insulo-frontal epileptic network. Magnetic Resonance Imaging (MRI) brain showed subcortical Fluid-Attenuated Inversion Recovery (FLAIR) hyperintensities in bilateral posterior parietal lobes (right>left), left frontal lobe, right posterior temporal and occipital lobes with punctate susceptibility artifacts in bilateral frontal, parietal white mater and left thalamus, which led to a suspicion of an underlying vasculitis. Cerebrospinal fluid study showed elevated protein (124 milligram per decilitre) with no cells or hypoglycorrhachia. Anti-nucleosome and anti ku antibodies were positive. So, an immune mediated vasculitis presenting as focal onset epilepsy was considered. SLE was diagnosed as these antibodies were highly specific. Patient was treated with intravenous methylprednisolone followed by mycophenolate mofetil and oral steroids. She became seizure free and was asymptomatic on follow up (Figure 1).

Case 2: A 23-year-old lady presented with episodes of auditory hallucinations (musical sounds), left oculocephalic version accompanied by impaired awareness lasting 15-20 seconds since the age of 13 years. She continued to have seizures with a frequency of up to three episodes per month despite on multiple AEDs. Ten years later, she developed polyarthralgia with recurrent oral ulcers, hair loss and photosensitivity prompting evaluation for an underlying Connective Tissue Disease (CTD). She had cognitive impairment affecting her routine activities. MRI brain was normal. VEEG showed right anterior and mid temporal sharp waves (Supplementary file 2). Clinical event was characterised by non forceful head adversion to the left side and impaired awareness. Ictal EEG showed a theta rhythm in the left anterior temporal channels, following which there was an ictal switch to rhythmic theta activity over the right frontotemporal regions followed by diffuse slowing. A localization related epilepsy involving temporal neocortical region (in view of the auditory aura) with bilateral epileptogenicity was considered. Autoimmune work up showed positive anti-doublestranded DNA, anti-nucleosome and anti-ribosomal P antibodies confirming the diagnosis of NPSLE. She also had features of lupus nephritis. As she had refractory and disabling focal epilepsy with renal involvement, she was treated with 6 months of cyclophosphamide pulse therapy, followed by azathioprine as maintenance treatment. There was a remarkable reduction in her seizure frequency and her cognitive issues also improved on follow up (Figure 2).
Discussion
Patients with SLE have a 4.5-fold increased risk of epilepsy and this has been attributed ischemic vascular disease or auto-antibody mediated neuronal damage [5,9]. Seizures usually develop early after the onset of SLE, except in rare instances reported where the initial presentation was status epilepticus or epilepsy preceded years before the diagnosis [6-8]. SLE patients are predisposed to having recurrent seizures if they have nephritis, antiphospholipid antibodies, seizures at disease onset or interictal epileptiform abnormalities on EEG [5]. The most common seizure type is tonic-clonic followed by seizure with impaired awareness , and seizure with retained awareness [2]. In a study by Toyota et al., all patients who had presented with focal onset seizures had mesial temporal lobe epilepsy [4]. The prevalence of MTLE in SLE was 2.9% which was much greater in comparison to the general population. This was an indicator of increased predisposition for focal onset epilepsies involving temporal lobe or limbic networks in SLE. Focal onset seizures involving the limbic network other than the mesial temporal lobe in SLE have not been described previously.
Absence of the classical systemic symptoms of SLE and negative autoimmune markers can result in misdiagnosis or delay in diagnosis. In both these cases, onset of seizures preceded the diagnosis of SLE by several years, unlike in previous studies where seizures generally occurred after the onset of disease [4]. Initiation of immune suppressants resulted in significant improvement with reduction in seizure frequency, thereby confirming the speculation of immune mediated insult. The age of onset of focal epilepsies involving the limbic network in SLE was late when compared to the general population. Later age of onset and sero positivity for antibodies also suggests an immune mechanism. Our cases highlight the clinical implication of the rare association between SLE and drug refractory focal epilepsies of the limbic system. The diagnosis can be challenging when there is a slow temporal evolution of the primary disease.
Conclusion
In conclusion, the cases presented underscore the importance of recognizing refractory focal epilepsy as a potential rare clinical manifestation of Systemic Lupus Erythematosus (SLE), particularly when neurological symptoms precede the typical systemic manifestations of the disease. These instances shed light on the complexity of diagnosing autoimmune-related epilepsies, especially when patients present with seizures resistant to conventional antiepileptic drugs. The observed dramatic responses to immunotherapy further emphasize the significance of considering immune-mediated mechanisms in the pathogenesis of such epilepsy, particularly when other autoimmune markers are present. The delayed onset of focal epilepsies involving the limbic network in SLE patients, along with the presence of specific antibodies, suggests a unique immunological pathway underlying these neurological manifestations. These cases highlight the need for a high index of suspicion and comprehensive autoimmune workup in young females presenting with drug-resistant focal epilepsy, particularly when atypical neurological features are present, to ensure timely diagnosis and initiation of appropriate treatment strategies.
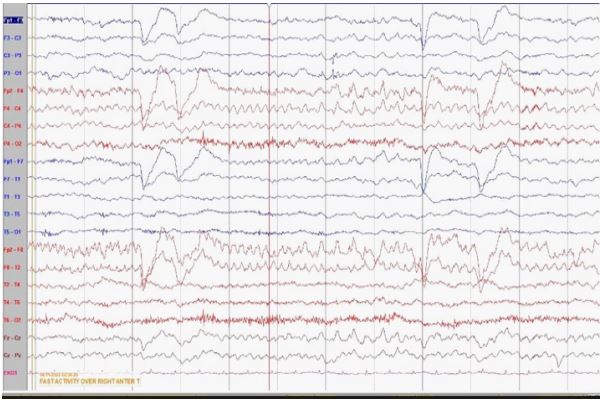
Supplementary file 1
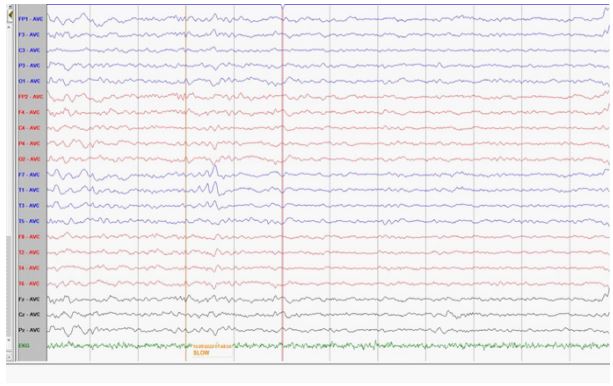
A. Interictal EEG showing sharp waves in the left anterior temporal region.
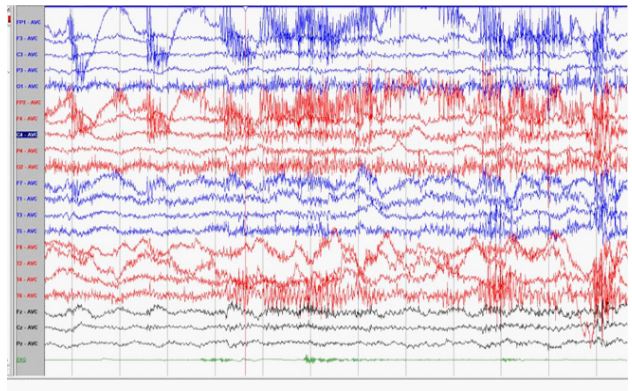
B. Ictal EEG marred by myogenic artifacts and onset showing no lateralising or localizing features
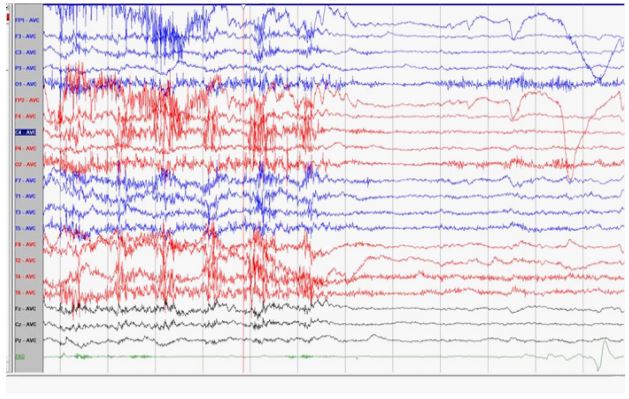
C. Evolution of ictal EEG showing a fast activity in the midline channels (Fz, Cz)
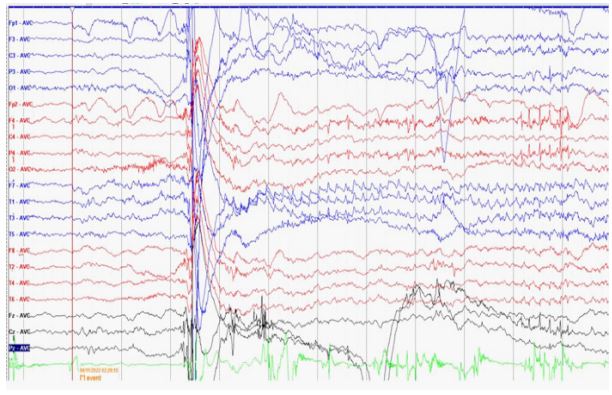
D. Ictal EEG offset showing post ictal attenuation
Video 1
Clinical event of patient 1 characterised by sudden arousal from sleep, retching sensation, attempt to cover her mouth with the left hand and suggestion of left upper limb automatisms.
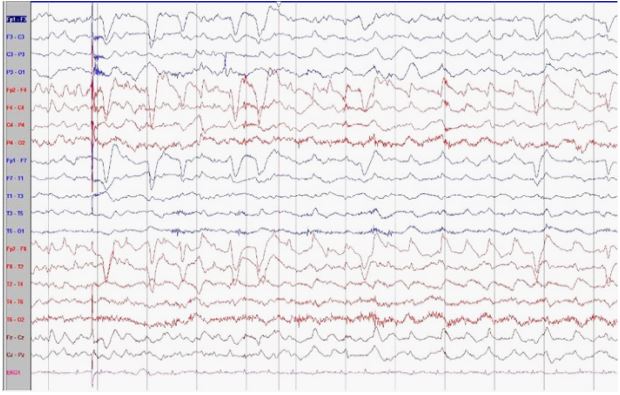
Supplementary file 2
A. Interictal EEG showing sharp waves in the right anterior and mid temporal regions.
B. Ictal EEG onset revealing an initial theta rhythm in the left anterior temporal channels,
C. Evolution of ictal EEG showing an ictal switch to rhythmic theta activity over the right frontotemporal regions
D. Post ictal slowing
Acknowledgement: None.
References
- Carrión-Barberà I, Salman-Monte TC, Vílchez-Oya F, Monfort J. Neuropsychiatric involvement in systemic lupus erythematosus: a review. Autoimmunity Reviews. 2021;,20(4):,102780.
- Rodriguez-Hernandez A, Ortiz-Orendain J, Alvarez-Palazuelos LE, Gonzalez-Lopez L, Gamez-Nava JI, Zavala-Cerna MG. Seizures in systemic lupus erythematosus: A scoping review. Seizure. 2021; 86: 161-7.
- González-Duarte A, Cantú-Brito CG, Ruano-Calderón L, GarcíaRamos G. Clinical description of seizures in patients with systemic lupus erythematosus. European neurology. 2008; 59(6): 320-3.
- Toyota T, Akamatsu N, Tanaka A, Shouzaki T, Tsuji S, Saito K, Tanaka Y. Mesial temporal lobe epilepsy as a neuropsychiatric syndrome of systemic lupus erythematosus. Epilepsia. 2013; 54(3): e33-6.
- Appenzeller S, Cendes F, Costallat LT. Epileptic seizures in systemic lupus erythematosus. Neurology. 2004; 63(10): 1808-12.
- Mackworth-Young CG, Hughes GR: Epilepsy: an early symptom of systemic lupus erythematosus . J Neurol Neurosurg Psychiatry. 1985; 48: 185. 10.1136/jnnp.48.2.185 13.
- İncecik F, Herguner MO, Yilmaz M, Altunbasak S: Systemic lupus erythematosus presenting with status epilepticus: a case report. Turk J Rheumatol. 2012; 27: 205-7. 10.5606/tjr.2012.034 14.
- Iftikhar PM, Munawar M, Hasan CA, FaisalUddin M, Cohen A: A challenging diagnosis of systemic lupus
- Lin Z, Si Q, Xiaoyi Z. Association between epilepsy and systemic autoimmune diseases: A meta-analysis. Seizure. 2016; 41: 160-6. doi: 10.1016/j.seizure.2016.08.003. Epub 2016 Aug 23. PMID: 27592469.