
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Antimalarial drug retinopathy: About a case
Anass Boujaada*; Younes Tlemçani; Lobna Robbana; Zahira Hazil; Louay Serghini; Abdallah Elhassan
Ophtalmology “B” Department, Specialties Hospital –IBN SINA Hospital University Center, Rabat, Morocco.
*Corresponding Author : Anass Boujaada
Ophtalmology “B” Department, Specialties Hospital –IBN SINA Hospital University Center, Rabat, Morocco.
Email: anass.boujaada@gmail.com
Received : Mar 05, 2024
Accepted : Mar 22, 2024
Published : Mar 29, 2024
Archived : www.jcimcr.org
Copyright : © Boujaada A (2024).
Abstract
Antimalarial drugs are widely used for the treatment of various systemic diseases. They can cause toxic retinopathy, which can lead to blindness. We report the case of a 35-year-old male with a systemic lupus erythematosus treated with hydroxychloroquine 400 mg per day. Sixteen months after his latest visual examination fundus examination revealed a bull’s eye maculopathy. Additional tests including multifocal electroretinogram showed severe bilateral functional impairment in the parafoveal area leading to diagnosis of severe toxic retinopathy induced by antimalarial drugs.
Keywords: Retinopathy; Antimalarial drug; systemic disease; Macular disease.
Citation: Boujaada A, Tlemçani Y, Robbana L, Hazil Z, Serghini L. et al. Antimalarial drug retinopathy: About a case. J Clin Images Med Case Rep. 2024; 5(3): 2951.
Introduction
Antimalarials drugs are widely prescribed since the 1950s with more than 30,000 patients treated over time courses in France for systemic diseases, such as lupus with effectiveness in reducing the risk of flare-ups, relapse and death [1]. Toxic retinopathy is one of the main side effects of this drug class. It is a dose-dependent effect responsible for an often bilateral, irreversible loss of the retinal pigment epithelium with no therapeutic possibility. It concerns approximately 0.08 to 0.5% of patients under treatment, which can even go up to 2% for certain authors [2].
Clinical case
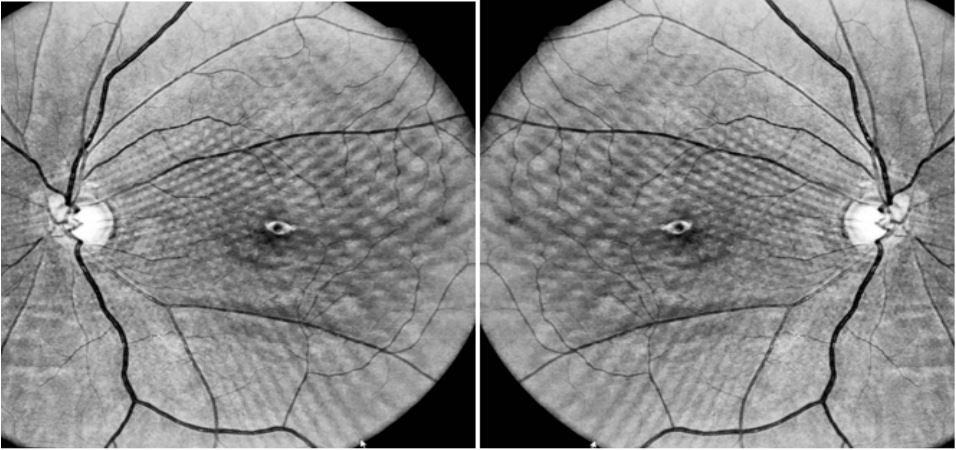
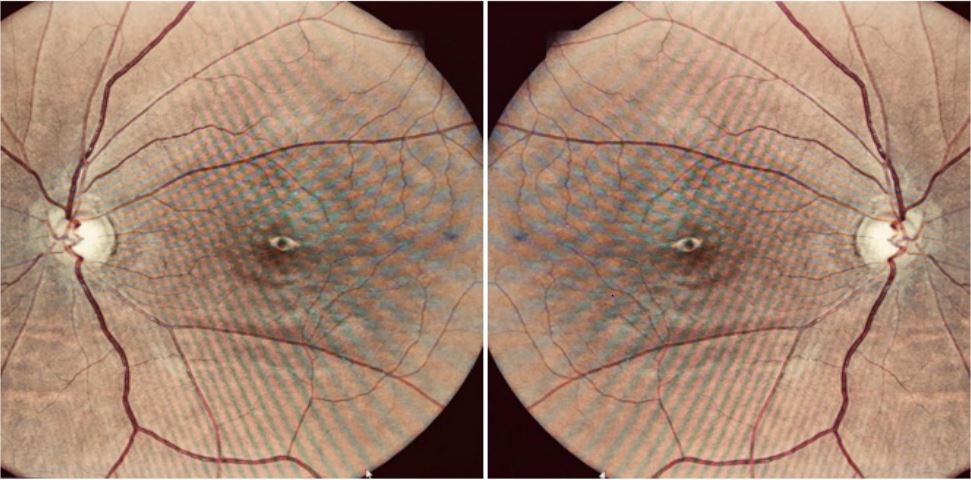
A 35-year-old patient weighing 65 kg, presenting since 2008 with systemic lupus erythematosus treated for 8 years with hydroxychloroquine 400 mg/day, i.e. on average 5.9 mg/kg/day. The initial ophthalmological assessment including visual field, vision color and global Electroretinogram (ERG), did not show any anomaly. He then benefited from an ophthalmological follow-up with fundus, visual field, color vision and global ERG every 12 to 18 months without any abnormality detected at the last follow-up in July 2022. Sixteen months later, the patient reported visual disturbances such as a reduction in bilateral visual acuity gradual installation over 6 months. The ophthalmological examination regains normal visual acuity in both eyes without correction. The fundus reveals pigmentary changes macular with a typical “bull’s eye” appearance. Spectral domain optical coherence tomography (SD-OCT), highlights a frank “flying saucer” sign with a disappearance of the interdigitation zone and the ellipsoid line,as well as a thinning of the outer nuclear layer, in an annular perifoveal zone, indicating atrophy at the expense of the photoreceptor layer (Figure 1). Autofluorescence images show hypoautofluorescence in this area. There was a Bull’s eye macular showing retinal atrophy, associated with hypoautofluorescent lesions along the arches temporal vascular peripapillary (Figure 2).
The visual field shows a bilateral absolute annular scotoma extended to the area of the central 10 degrees and associated with an enlargement of the blind spot but respecting the foveolar zone, which constitutes a serious functional impairment. Severe APS retinopathy is then suspected; a multifocal ERG is performed in addition and reveals a typical appearance of bilateral perifoveal deficit. The diagnosis of severe APS retinopathy is made, treatment with APS is stopped and contraindicated for life. In order to limit possible worsening even after stopping, precautions are taken: stopping smoking, eating a diet rich in fatty fish and green vegetables, wearing filter lenses to protect the retina from UV rays. A follow-up every 6 months is set up with visual field, SD-OCT, and auto fluorescence pictures.
Discussion
Retinal toxicity to antimalarial drugs has been known since the 1960s but its pathophysiology is not yet well understood. The affinity chloroquine and hydroxychloroquine for melanin would be the cause of an alteration of lysosomes, in particular of those of the pigment epithelium, and photoreceptors. This degenerative process begins at the level of ganglion cells but it is the photoreceptors which are the most severely attack leading to retinal damage [3]. We distinguish two affected: asymptomatic preclinical attack characterized by abnormalities visible only on additional examinations and clinical involvement characterized by signs irreversible visual functional disorders such as a scotoma, visual bluror a decrease in visual acuity associated with objective clinical abnormalities such as a “bull’s eye” image on the FO and paraclinics. Thus, systematic screening of patients under antimalarial drugs is recommended in order to detect this damage at the pre-stage clinical and avoid its evolution towards a symptomatic attack irreversible.
Recommendations regarding treatment monitoring to the antimalarial drugs were the subject of updates in 2011 then 2016 by the American Academy of Ophthalmology (AAO) due to new data on the prevalence of retinal deficiency and the onset new diagnostic techniques. This monitoring included in 2011 an ophthalmological examination with measurement of visual acuity, study of the cornea to search for vertical cornea, FO, production of an automated CV 10.2 associated with a multifocal ERG which should be preferred or failing that a SD-OCT and/or auto fluorescence images [4].
Conclusion
The use of antimalarial drugs is increasingly frequent with prescription increased by 30% compared to the 90s [5], mainly for the treatment of systemic lupus erythematosus. This case reminds us that, although rare, severe retinopathy to APS may occur. It allows the recall of recommendations recently updated which are sometimes little known by practitioners and to insist both on an adaptation of the dose used to the patient’s weight, a frequent reassessment of this dose, and on the need for annual ophthalmological monitoring. The latter makes it possible to detect the attack in an asymptomatic phase.
References
- Costedoat-Chalumeau N, Ingster-Moati I, Leroux G, Fardeau C, Benveniste O,Simon C, et al. Critical review of the new recommandations on screening forhydroxychloroquine retinopathy. Rev Med Interne. 2012; 33: 265-7.
- Ingster-Moati I, Crochet M, Manchon E, Anquetil D, Lestrade C, Jacob A,et al. Analysis of 925 patients on long-term hydroxychloroquine or chlo-roquine treatment: results of ophtalmological screening. J Fr Ophtalmol. 2004; 27: 367-73 [4].
- Tzekov R. Ocular toxicity due to chloroquine and hydroxychlor oquine:electrophysiological and visual function correlates. Doc Ophthalmol. 2005; 110: 111-20.
- Ingster-Moati I, Orssaud C. Ophtalmological monitoring protocol forpatients treated with long-term antimalarials or vigabatrin. J Fr Ophtalmol. 2009; 32: 83-8 [3]
- Guiot A, et al. Rétinopathie sévère aux antipaludéens de synthèse. Rev Med Interne. 2017.