
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Off-label use of therapeutic plasma-exchange in postasymptomatic covid-19 autoimmune encephalopathy
Annamaria Petrungaro*; Paolo Sciarrone; Eugenia Quartarone
Department of Service, University Hospital G. Martino of Messina, Italy.
*Corresponding Author : Annamaria Petrungaro
Department of Service, University Hospital G. Martino of Messina, Italy.
Email: annamaria.petrungaro@polime.it
Received : Mar 09, 2024
Accepted : Mar 22, 2024
Published : Mar 29, 2024
Archived : www.jcimcr.org
Copyright : © Petrungaro A (2024).
Abstract
Hypertensive tetraventricular hydrocephalus in association with polyradiculoneuritis and leptomeningitis in patients are very unusual conditions that can be related to viral infections. We report the case of a patient with severe post-covid 19 encephalopathy who underwent Therapeutic Plasma Exchange (TPE) as an “off-label” use.
Keywords: Post Covid-19; Autoimmune encephalopathy; Hypertensive tetraventricular hydrocephalus; Therapeutic plasma-exchange.
Citation: Petrungaro A, Sciarrone P, Quartarone E. Off-label use of therapeutic plasma-exchange in post-asymptomatic Covid-19 autoimmune encephalopathy. J Clin Images Med Case Rep. 2024; 5(3): 2953.
Background
In 30-80% of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-Cov-2)’s various clinical manifestations, central nervous system involvement occurs as a severe persistent encephalopathy lasting for weeks after resolution of the acute viral infection [1]. This unknown pathophysiology involves different mechanisms, such as direct viral invasion of microvascular endothelium, microvascular thrombosis, toxic neuronal effects of inflammatory products, vasoactive pathology at arteriolar level or leptomeningeal inflammation, and autoimmune damage. There are no established specific treatments for post-COVID-19 encephalopathy. Herein, we report a case of a patient affected by severe both central and peripheral post-Covid 19 encephalopathy who underwent Therapeutic Plasma Exchange (TPE) with salinized albumin that suggests a positive therapeutic effect.
Case report
48-year-old female patient, Caucasian, height 160 cm, weight 60 kg, underwent tonsillectomy surgery at the age of 10 and appendectomy at the age of 19. She reported anaphylactic shock after taking ranitidine.
Hashimoto’s thyroiditis has been in replacement therapy for about 17 years. In 2015, surgery for exeresis of right upper eyelid melanoma in follow-up. In July 2022 paucisymptomatic SARS-CoV-2 infection. Covid-19 vaccination not performed. After 30 days, reported onset of paresthesias and dysesthesias in lower limbs, followed by progressive loss of strength and inability to maintain upright position. For this reason, in October 2022, she was admitted to the Neurology Unit, where she underwent Electromyography (EMG), Evoked Motor Potentials (EMPs) and Lumbar Puncture (albumin - cytological dissociation), Magnetic Resonance Imaging (MRI )of the brain and spine in its entirety with contrast agents (Arnold Chiari malformation type I with modest chronic hydrocephalic dilatation of the supratentorial system). On that occasion she performed a course of intravenous immunoglobulins (Ivigs) with little benefit. She was discharged with a “polyradiculoneuritis” diagnosis and continued rehabilitation until November 2022, with reported benefit.
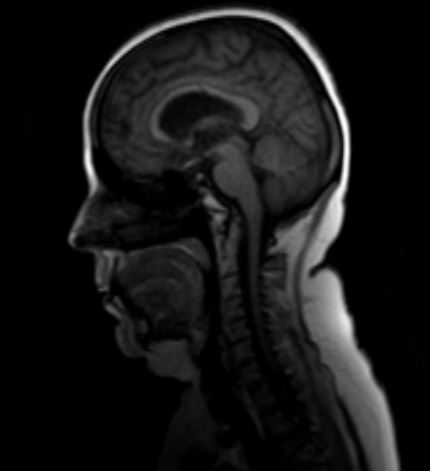
In December 2022, the patient experienced repeated “absence” type episodes in the course of an algic crisis for which she went to the General Emergency Room (ER), where she had a Computed Tomography (CT) scan of the brain (picture of dilatation of the ventricular system) and a specialist neurosurgical evaluation by telemedicine, which did not indicate any urgent treatment. Therefore, she was moved to the neurology unit. During her hospital stay, the patient fell to the ground twice, sustaining a compound fracture of the right peroneal malleolus, which was treated with plaster casts. She was discharged against doctor’s advice. On 13/12/2022, due to the reappearance of “absence” type episodes, she was admitted to the ER, where she underwent serial encephalic CT scans that showed evidence of dilation of the ventricular system with signs of transependymal transudation. For this reason, she was transferred to the Neurosurgery Unit, where she underwent placement of ventricle-peritoneal shunt with Codman Certas programmable valve calibrated at 4. She was discharged with the diagnosis of “hypertensive tetraventricular hydrocephalus, undetermined polyradiculoneuritis and leptomeningitis”. In January 2023, new admission to the Neurosurgery Unit for soporific state and appearance of numerous “absence” type seizures. MRI revealed tetraventricular hydrocephalus with diffuse meningeal impregnation of all the cerebral meninges, cranial nerve course, spinal nerve roots and cauda equina (Figure 1).
Although various Cerebrospinal Fluid (CSF) examinations were performed, the cells always resulted normal except for a single finding of pleiocytosis (400 mmc, blood sample) not confirmed on subsequent blood sample (10 mmc) and slight hyperproteinorrachia (approx. 60 mg/dl). At EMG, neurogenic pain with aspects of collateral reinnervation on all the muscles examined, prevalent on the distal muscles of the lower limbs, with obvious signs of denervation on the dorsal I interosseous muscles of the right and left hand, right and left anterior tibial. Electroencephalogram (EEG): Altered cerebral electrical activity due to the presence of theta activity trains and slow spikes on the temporal regions of both hemispheres, clearly prevailing on the left. Neurological examination on admission to the ward: Patient alert, oriented, collaborating. Complaints of pains in the pelvis and lower limbs. Speech is Normal. Nystagmus in lateralised gaze to the right. Standing and walking not assessable. Hyposthenia in the limbs, increased in the lower ones. Deep Tendon Reflexes (DTR) absent in all four limbs. Hypoesthesia and hypopallesthesia, no Babinski.
Therapy performed: Ivigs HD 2 g/kg for 5 days Methylprednisone HD 1 g for 5 days followed by maintenance dose 40 mg/day + gastric protection, anticonvulsant, antiepileptic and broad-spectrum antibiotics, slow-release pain relief therapy, rehydration and colloid therapy, heparin therapy.
Temporary improvement of neurological symptomatology with worsening of symptoms at day + 15: appearance of paresthesias and tactile and nociceptive hypoesthesia at the hemiface. Mild distal hyposthenia in the right hand. Deficit of strength in dorsiflexion in both feet Medical Research Council Scale 2 (MRC- 2), can lift right knee off bed surface. Maintained Mingazzini II on the left for less than 5 seconds, algic bilateral symptoms from pelvis to feet. TPE was considered as an experimental option with the patient.
After discussion of the potential risks and unknown benefits of TPE, an informed consent was obtained [2].
A 12 Fr 20 cm bilumen Central Venous Catheter (CVC)is placed in right femoral veins, echo-guided using the Seldinger technique.
The Fresenius COM. TEC cell separator was used. Patient’s height was 160 cm and she weighed 60 kg.
Treated blood’s entire volume was on average 2300 ml and consistent of 1-1.5 plasma volume exchange with salinized albumin, performed on alternative days for a total of 3 treatments over 7 days, neurological status significantly improved after TPE, both clinically and on EEG EMG and MRI. Anticoagulant Citrate Dextrose Solution, Solution A (ACD-A) was used as an anticoagulant, while ACD-A related hypocalcemic syndrome was treated according to guidelines.
Discussion and conclusion
Covid-19 infection can be associated with various forms of autoimmune encephalopathy both in the acute phase and after the resolution of the infection with a variable timing (range 6-36 months from onset): including both central limbic and brainstem encephalitis, Acute Disseminated Encephalomyelitis and Myelitis (ADEM) and peripheral diseases (Guillain–Barré and Miller Fisher syndrome) [3].
The pathogenesis underlying this association is uncertain. Multiple studies do not support the hypothesis of a direct neurotropism by the Covid-19 virus [4].
However, Covid-19 infection generates a ‘dysregulation of the immune system’ that alters and damages the nervous system at neuronal synapses, neuromuscular and myelin levels.
The Cytokine storm generated in Sars-Cov-2 results in an increase in the permeability of the BBB blood-brain barrier with direct invasion of the virus causing cell death and endotheliitis with a brain biopsy picture suggestive of immune-mediated encephalitis (increased microglia and increased cytotoxic T lymphocytes) [5].
In the Central Nervous System (CNS), the presence of interleukin-1β, interleukin-6, IP-10, TNF, interferon-γ, Macrophage Inflammatory Protein (MIP) 1α and 1β, and VEGF, leads to an increase in the innate immune response in cells expressing the Toll receptor and an increase in autoantibodies, through cross-reactivity and ‘molecular mimicry’ directed against neurons, glia and extra-neural tissue (anti-NMDAR, Anti -Yo, AntiCaspr2, Anti-MOG, Anti-GD1b) [6].
Therapy of these forms of post-Covid autoimmune encephalopathy is based on immunosuppressive, anti-inflammatory, immunomodulatory and neurotropic drugs. The rationale for the use of TPE is linked to its use with indication I-II-B American Society of Apheresis (ASFA) 2023 in Myasthenia Gravis, Guillain Barre’ and chronic inflammatory demyelinating polyneuropathy linked to its ability to remove antibodies, inflammatory mediators and cytokines from the patient’s plasma [7].
References
- Ariño H, Heartshorne R, Michael B, Nicholson T, Vincent A, Pollak T, Vogrig A.Neuroimmune disorders in COVID-19.J Neurol. 2022; 269(6): 2827-2839.
- Ranganathan C, Fusinski S, Obeid I, Ismail K, Ferguson D, Raminick M et al. Therapeutic plasma exchange for persistent encephalopathy associated with Covid-19. eNeurologicalSci. 2021; 22: 100327.
- Liotta E, Batra A, Clark JR, Shlobin N, Hoffman S, Orban Z et al. Frequent neurologic manifestations and encephalopathy-associated morbidity in Covid-19 patients. Ann Clin Transl Neurol. 2020; 7(11): 2221-2230.
- Iadecola C, Anrather J, Kamel H Effects of COVID-19 on the nervous system. 2020; 183(1): 16-27.e1.
- Kreye J, Reincke SM, Kornau H-C, Sánchez-Sendin E, Corman V, Liu H et al. A therapeutic nonself-reactive SARS-CoV-2 antibody protects from lung pathology in a COVID-19 hamster model. 2020; 183(4): 1058-1069.e19.
- Franke C, Ferse C, Kreye J, Reincke SM, Sanchez-Sendin E, Rocco A,High frequency of cerebrospinal fluid autoantibodies in COVID-19 patients with neurologicalsymptoms.Brain Behav Immun. 2021; 93: 415-419.
- Ginikopoulou E. Plasma exchange and COVID 19 Transfus Apher Sci. 2022; 61(6): 103598.