
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Metabolic-associated steatotic liver disease: A natural history from steatosis to hepatocellular carcinoma and liver transplantation: A case report
Helma P Cotrim¹*; Liana Codes²; Luiz Antonio Rde-Freitas³
1Graduate Program in Medicine and Health (PPgMS) and GNASH/CNPq-Faculty of Medicine-Federal University of Bahia (UFBA), Salvador-Bahia, Brazil.
2Portuguese Hospital of Bahia, Salvador, Brazil.
3Faculty of Medicine of Bahia (UFBA), Brazil, Gonçalo Moniz Research Center - Oswaldo Cruz Foundation, Salvador-Bahia, Brazil.
*Corresponding Author : Helma P Cotrim
Graduate Program in Medicine and Health (PPgMS) and GNASH/CNPq-Faculty of Medicine-Federal University of Bahia (UFBA), Salvador-Bahia, Brazil.
Email: helmacotrim@gmail.com
Received : Mar 05, 2024
Accepted : Mar 25, 2024
Published : Apr 01, 2024
Archived : www.jcimcr.org
Copyright : © Cotrim HP (2024).
Abstract
This case report follows a 67-year-old male with diabetes (T2DM) and Metabolic- Associated Steatotic Liver Disease (MASLD) over a two-decade. The patient progressed from hepatic steatosis to steatohepatitis (MASH) and cirrhosis from 2006 to 2009. Hepatocellular Carcinoma (HCC) was found via CT scan in 2012, leading to a Liver Transplantation (LT) in 2014. Explanted liver showed cirrhosis and five macro nodules. Histopathological evaluation identified well-differentiated HCCs with a trabecular and pseudo-acinar pattern and cholestasis. Unsuspected areas had small well-differentiated HCCs forming nodules or infiltrating non-neoplastic hepatocyte plates within cirrhotic nodules. The tumor was classified as an HCC of the diffuse/cirrhotomimetic type. Despite exceeding Milan criteria, the patient has 10 years of recurrence-free survival after LT. In conclusion, this case illustrates the natural history of MASLD form steatosis, MASH to cirrhosis and HCC and highlights successful outcomes in certain HCC types. A decade post-liver transplantation, the patient leads a normal life without any recurrence of HCC.
Keywords: Metabolic-Associated Steatotic Liver Disease (MASLD); Metabolic-Associated Steatohepatitis (MASH); Hepatocellular Carcinoma (HCC).
Citation: Cotrim HP, Codes L, Rde-Freitas LA. Metabolic-associated steatotic liver disease: A natural history from steatosis to hepatocellular carcinoma and liver transplantation: A case report. J Clin Images Med Case Rep. 2024; 5(4): 2955.
Introduction
Disease (MASLD), the new nomenclature to Non-Alcoholic Fatty Liver Disease (NAFLD) is estimated in 30%, and it is increasing worldwide [1,2]. MASLD encompasses a spectrum of diseases including steatosis, steatohepatitis, which can progress to cirrhosis and Hepatocellular Carcinoma (HCC). It is associated with obesity, diabetes mellitus (T2DM), hyperlipidemia, metabolic syndrome, and it is possible that the rates of MASLD-related HCC are increasing in parallel with the obesity epidemic [3].
Multiple factors (genetic, epigenetic, environmental, clinical) are involved in MASLD natural history and the disease progression, and the results are a variety of clinical phenotypes that require an individual approach. It is important to understand the natural history of MAFLD and identify risk factors that can modify the disease evolution [4].
The metabolic conditions such obesity and diabetes are the most frequent and main risk factors for progressive MAFLD, but the qualitative components of diet, physical activity, and genetic factors also play a significant role.
This report aims to describe the natural progression of MASLD through the case of a patient who survived over a 20-years period, encompassing the stages of steatosis, steatohepatitis (MASH), cirrhosis, HCC, culminating in the necessity for liver transplantation.
Case presentation
A man, 67 years old Caucasian, technical accountant, who had diagnosis of type T2DM in 2002 and hepatic steatosis in 2006.
The patient was investigated for major liver diseases, including infection by hepatitis B and C viruses (negative for HBsAg and anti-HCV), autoimmune hepatitis (negative for anti-nuclear antibodies, anti-smooth muscle antibodies, anti-LKM, and anti-mitochondrial antibodies), hemochromatosis (normal ferritin and transferrin saturation), liver disease related to alcohol consumption (both the patient and their family denied alcohol consumption), and drug-induced liver injury (negative history for the use of illicit drugs, medications, supplements, and herbal teas). All investigations yielded negative results.
In 2009 during a cholecystectomy and liver biopsy had diagnosis of MASH and cirrhosis. The patient was followed with T2DM control, MASH treatment with pioglitazone and E vitamin, and he was included in screening for HCC with abdominal ultrasound and alpha- fetoprotein measurement every 6 months.
He did not exhibit any obesity-related issues. His BMI consistently ranged between 24 and 25 kg/m², and he and his family have consistently maintained a healthy lifestyle, incorporated daily walks, and adhered to a balanced diet, which is overseen by an endocrinologist.
In 2011, he was diagnosed by ultrasound and a Magnetic Resonance Image (MRI) of the abdomen three hyper vascular nodules with wash-out with the following locations and sizes: Sec VI - 1.4 cm, sec VIII - 1.3 cm, sec VIII/V - 1.0 cm compatible with HCC. The patient was placed on the transplant waiting list and in 2014 he underwent Liver Transplantation (LT).
During the wait on the liver transplant list, the patient began to develop liver failure manifested by jaundice, ascites, and edema (managed with albumin replacement and diuretics). Subsequently, the patient developed spontaneous bacterial peritonitis, which was treated with antibiotics and resolved. At the time of transplantation, there was no infection present. Edema and ascites were under control, as was diabetes.
The laboratory results at the time of transplantation are as follows: Hemoglobin (Hb): 4/dL; Leukocytes (leuco): 13,630/mm³; Platelets (plaq): 130,000/mm³, cRP-serum level 0, 3 a 1 mg/Dl; Glucose: 92 md/dl; glycated hemoglobin 5, 4. Blood Type (BT): 12.6 seconds (International Normalized Ratio [INR] 1.3); Creatinine (Cr): 1.4 mg/dL; Sodium (Na): 135 mEq/L; Potassium (K): 4.4 mEq/L; AST: 144 U/L; ALT: 55 U/L; GGT: 208 U/L; Albumin (alb): 2.0 g/dL; Bicarbonate (HCO3): 17 mEq/L; Lactate (lact): 2.5 mmol/L; MELD score: 30; Acute Physiology and Chronic Health Evaluation (APACHE) score: 12. HBs Ag e anti HCV were negatives. Autoimmune hepatitis (negative for anti-nuclear antibodies, anti-smooth muscle antibodies, anti-LKM, and anti-mitochondrial antibodies), hemochromatosis (normal ferritin and transferrin saturation).
Anatomopathological evaluation: In 2009, the first liver biopsy showed cirrhosis parenchymal nodules of varying sizes with areas of macro vesicular hepatocellular steatosis, hepatocyte ballooning with frequent Mallory-Denk bodies, and per sinusoidal fibrosis. These findings were consistent with remnants of a steatohepatitis associated with the patient’s metabolic disorder (Figures 1A-D). Additionally, there was mild hepatocytic iron overload and some foci of hepatocellular dysplasia of small and large cells (Figure 1E-F). In 2010, during cholecystectomy, a new liver biopsy revealed findings like the previous one and an increased iron overload. In 2014, one year after the suspicion of three HCCs in imaging studies and worsening of hepatic insufficiency, the patient underwent liver transplantation.
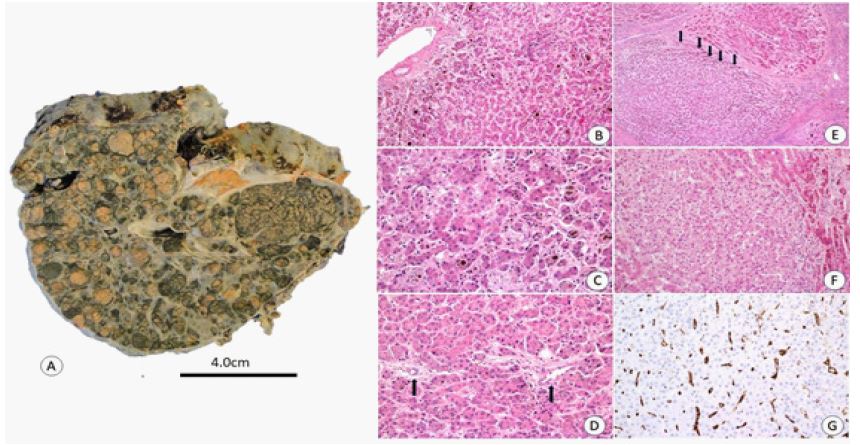
The explanted liver revealed a cirrhotic appearance with nodules ranging from 0.5 to 2.5 cm, displaying a variegated appearance, with shades of green and yellow. Five macro nodules were identified in segments III, IV, V, VI, and VII. The largest nodule measured 4.0x2.5 cm, and the smallest measured 1.0x1.0 cm (Figure 2A). Histopathological evaluation showed that all of them were well-differentiated hepatocellular carcinomas according to the WHO classification (grades 1 and 2 in the Edmondson & Steiner classification), with a trabecular and pseudo-acinar pattern and intense cholestasis (Figure 2B-D). No vascular invasion was detected. Multiple sections taken from areas previously unsuspected of tumors revealed the presence of dozens of small HCCs, many of them forming well-defined isolated nodules and others growing within cirrhotic nodules, permeating non-neoplastic hepatocytes (Figure 2E-F). Immunostaining with CD 34 revealed sinusoidal capillarization within the tumors (Figure 2G) All tumors were well differentiated trabecular/pseudoacinar HCC. The gross and microscopic aspects are consistent the cirrhotocmimetic type of HCC.
Treatment post: It included corticosteroids, tacrolimus, and mycophenolate. On the follow up the patient developed cholestatic enzymes alterations, with normal hepatic artery doppler and cholangio-MRI. He was discharged from hospital four months after LT in use of small dose of tacrolimus, mycophenolate.
Evolution: After twenty-two years of the steatosis diagnosis and a decade of Liver Transplantation (LT), the patient is now leading a regular and fulfilling life. They are actively engaged in their occupation, with no reported instances of HCC recurrence. The functioning of their liver remains within normal parameters, and other health conditions, including diabetes, arterial hypertension, dyslipidemia, and renal function, are well- managed.

Discussion
This case involves interesting points for discussion, and it is related to clinical aspects and the progression of Metabolic-Associated Steatotic Liver Disease (MASLD), as well as the histopathological aspects and the patient outcome.
We present a case of a patient with T2DM, who initially received a diagnosis of isolated steatosis. This condition progressed to steatohepatitis, cirrhosis, and eventually HCC over a period of 10 years. The patient underwent Liver Transplantation (LT). Upon evaluating the liver explant, not only were the three nodules seen in imaging studies observed, but also a diffuse and infiltrative HCC, outside the Milan Criteria recommended for selecting patients with HCC for liver transplantation [5]. Despite this challenging diagnosis and the expectation of a poorer prognosis, the patient, after more than a decade of follow-up, remains clinically well and without tumor recurrence.
Patients with MASLD and T2DM have an elevated risk of HCC, which is the fourth- leading cause of cancer death worldwide. The estimated annual incidence of HCC ranges from 0.5% to 2.6% among patients with MASH cirrhosis, and for patients with non-cirrhotic MASLD, it is 0.1 to 1.3 per 1,000 patient-years. However, even though the incidence of MASLD-related HCC is lower than that of HCC caused by other factors such as hepatitis C, the prevalence of MASLD is higher compared to other diseases like alcohol-related and autoimmune liver disease [6-8].
Another point is that the patient was 57 years old when diagnosed with HCC, which is a younger age compared to cases typically associated with MASLD-related HCC. In such instances, HCC is more prevalent in individuals with an average age of 73 years in patients with hepatitis C virus infection and 70 years in patients with hepatitis B virus infection [6-9]. Patients with MASLD-related HCC, when diagnosed at a more advanced stage, also have a post-transplant survival rate associated with a poorer prognosis compared to HCC related to viral hepatitis. However, in this case, the patient with HCC and cirrhosis, undergoing liver transplantation, demonstrates an excellent prognosis in the 10-year follow-up.
Liver Transplantation is the treatment of choice for patients with early-stage HCC and/or liver failure. It is a curative treatment for both the tumor and the underlying liver disease. Patients who meet the widely accepted Milan Criteria (i.e., a single nodule of 5 cm or 2-3 nodules, each 3 cm, with no macroscopic vascular invasion) have shown 4-year survival rates of up to 70%. The number and size of nodules, microscopic vascular invasion, and microscopic satellite nodules are the main risk factors for recurrence.
Based on previous reports, being outside the Milan Criteria was a factor associated with a higher risk of HCC recurrence and poorer survival [10-13].
The survival of patients with HCC undergoing liver transplantation is estimated to be around 6 months, given the elevated risk of recurrence associated with this neoplasm. This patient, despite unfavorable findings in the explant analysis, exhibited excellent clinical outcomes, related to the tumor’s biological behavior. Currently, there are still lacking markers to reliably predict recurrence. Molecular characteristics have been studied with the aim of identifying predictive factors for early HCC recurrence after liver transplantation [14].
In association with the clinical and evolutionary aspects of this patient, another point deserves discussion. This patient presented with a rare type of HCC and deserve several considerations. In the 2009 biopsy, cirrhosis associated with MESH was diagnosed, along with mild hepatocyte iron overload. Both small and large cell changes were observed in the hepatocytes. Small cell changes are considered a direct precursor to HCC, while large cell change carry a risk [15-17]. In 2013, imaging confirmed nodules consistent with HCC. In 2014 the explanted liver revealed multiple HCC, with most going unnoticed during gross examination. These findings resemble the diffuse/cirrhotomimetic HCC, a rare type comprising 1-3% of cases [18-20]. Despite exceeding Milan criteria, this case has had 10 years of recurrence-free survival after transplantation, the longest reported in this type of HCC. The multicentric and asynchronous development of tumors points to the importance of field cancerization in the pathogenesis of this HCC type [21]. Reliable biomarkers are needed for risk prediction. The presence of small and large cell changes in the initial biopsy suggests a field cancerization effect leading to tumor development. Further studies are warranted to understand the biological behavior of this peculiar HCC variant, which is less aggressive with its low histological grade and bile-containing pseudo-acini resembling the histopathological findings described in tumors with the non-proliferative molecular signature pattern proposed by Calderaro, J et al. [22,23].
Conclusion
This case report illustrates the long and favorable progression of DEF-MET in a patient with type 2 Diabetes Mellitus (DMT2). Over two decades after the diagnosis of steatosis, it advances to the more severe forms of the disease, namely cirrhosis and HCC. The patient undergoes liver transplantation, with the expectation of tumor recurrence and a grim prognosis. However, the patient exhibits exceptional and rare survival with an excellent quality of life.
Declarations
Authors’ contributions: Conceived and designed the manuscript: Helma P Cotrim; Wrote the manuscript: Helma P Cotrim; Liana Codes; Luiz Antonio R de- Freitas. Critically revised the manuscript: Helma P Cotrim; Liana Codes; Luiz Antonio R de- Freitas.
Financial support and sponsorship: None.
Conflict of interest: All authors declared that there no conflicts of interest.
Ethical approval and consent to participate: The patients sign an informed consent which comprehends data collection in anonymized form, so no external ethical approval was necessary in this case.
Consent for publication: Written informed consent was obtained from the patient.
Acknowledgment: The authors would like to thank all clinical and surgical doctors who participated in the clinical evolution and liver transplant of the patient.
References
- Rinella ME, Lazarus JV, Ratziu V, Francque SM, Sanyal AJ, et al. A multisociety Delphi consensus statement on new fatty liver disease nomencla ture. J Hepatol. 2023; 79(6): 1542-1556. doi: 10.1016/j.jhep.2023.06.003.
- Younossi ZM, Golabi P, Paik JM, Henry A, Van Dongen C Henry. The global epidemiology of Nonalcoholic Fatty Liver Disease (NAFLD) and nonalcoholic steatohepatitis (NASH): A systematic review. Hepatology. 2023; 77(4): 1335-1347. doi: 0.1097/HEP.0000000000000004.
- McGlynn KA, Petrick JL, El-Serag HB. Epidemiology of hepatocellular carcinoma. Hepatology 2021; 73(Suppl 1): 4-13. doi: 10.1002/hep.31288.
- Pais R, Maurel T. Natural History of NAFLD. J. Clin. Med. 2021; 10: 1161. https://doi.org/10.3390/ jcm10061161.
- Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti A, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996; 334(11): 693-9. doi: 10.1056/NEJM199603143341104.
- Huang DQ, El-Serag HB, Loomba R. Global epidemiology of NAFLD-related HCC: trends, predictions, risk factors and prevention. Nat Rev Gastroenterol Hepatol. 2021; 18(4): 223-238. doi:10.1038/s41575-020-00381-6.
- Kim H, Lee DS, An TH, Park HJ, Kim WK, et al. Metabolic Spectrum of Liver Failure in Type 2 Diabetes and Obesity: From NAFLD to NASH to HCC. Int J Mol Sci. 2021; 22(9): 4495. doi: 10.3390/ijms22094495.
- Ye F, Chen L, Zheng X. Diabetes and the risk of cirrhosis and HCC. An analysis of the UK Biobank. Hepatol Commun. 2023; 7(11): e 0280. doi: 10.1097/HC9.0000000000000280.
- Ioannou GN. Epidemiology and risk-stratification of NAFLD-associated HCC. J Hepatol. 2021; 75(6): 1476-1484. doi: 10.1016/j.jhep.2021.08.012.
- Plessier A, Codes L, Consigny Y, Sommacale D, Dondero F, et al. Underestimation of the influence of satellite nodules as a risk factor for post- transplantation recurrence in patients with small hepatocellular carcinoma. Liver Transpl. 2004; 10(2 Suppl 1): S86-90. doi: 10.1002/lt.20039.
- Sotiropoulos GC, Molmenti EP, Lösch C, Beckebaum S, Broelsch CE, et al. Meta-analysis of tumor recurrence after liver transplantation for hepatocellular carcinoma based on 1,198 cases. Eur J Med Res. 2007; 12(10): 527-34.
- Maccali C, Chagas AL, Boin I, Quiñonez E, Marciano S, et al. Recurrence of hepatocellular carcinoma after liver transplantation: Prognostic and predictive factors of survival in a Latin American cohort. Liver Int. 2021; 41(4): 851-862. doi: 10.1111/liv.14736
- Chagas AL, Mattos AA, Diniz MA, Felga GEG, Boin IFSF, et al. Impact of Brazilian expanded criteria for liver transplantation in patients with hepatocellular carcinoma: A multicenter study. Ann Hepatol. 2021; 22: 100294. doi: 10.1016/j.aohep.2020.100294.
- Badwei N. Molecular Clues for Prediction of Hepatocellular Carcinoma Recurrence after Liver Transplantation. J Clin Exp Hepatol. 2023; 13(5): 804-812. doi: 10.1016/j.jceh.2023.02.006.
- Borzio M, Bruno S, Roncalli M, Mels GC, Ramella G, et al. Liver cell dysplasia is a major risk factor for hepatocellular carcinoma in cirrhosis: a prospective study. Gastroenterology. 1995; 108(3): 812-7. doi: 10.1016/0016- 5085(95)90455-7.
- Marchio A, Terris B, Meddeb M, Pineau P, Duverger A, et al. Chromosomal abnormalities in liver cell dysplasia detected by comparative genomic hybridisation. Mol Pathol. 2001; 54(4): 270-4. doi: 10.1136/mp.54.4.270.
- Park YN, Roncalli M. Large liver cell dysplasia: A controversial entity. J Hepatol. 2006; 45(5): 734-43. doi: 10.1016/j.jhep.2006.08.002.
- Clayton EF, Malik S, Bonnel A, Mu Y, Olthoff K, et al. Liver transplantation and cirrhotomimetic hepatocellular carcinoma: Classification and outcomes. Liver Transpl. 2014; 20(7): 765-74. doi: 10.1002/lt.23876.
- Jakate S, Yabes A, Giusto D, Naini B, Lassman C, et al. Diffuse cirrhosis-like hepatocellular carcinoma: a clinically and radiographically undetected variant mimicking cirrhosis. Am J Surg Pathol. 2010; 34(7): 935-41. doi: 10.1097/PAS.0b013e3181ddf52f.
- Xiong MJ, Patel CR, Manne U, Al Diffalha S. Cirrhotomimetic hepatocellular carcinoma: experience of a single institution and review of the literature. Hepat Oncol. 2020; 8(1): HEP28. doi: 10.2217/hep-2020-0015.
- Huang L, Songyang Z, Dai Z, Xiong Y. Field cancerization profile-based prognosis signatures lead to more robust risk evaluation in hepatocellular carcinoma. I Science. 2022; 25(2): 103747. doi: 10.1016/j.isci.2022.103747.
- Calderaro J, Couchy G, Imbeaud S, Amaddeo G, Letouzé E, et al. Histological subtypes of hepatocellular carcinoma are related to gene mutations and molecular tumour classification. J Hepatol. 2017; 67(4): 727-738. doi: 10.1016/j.jhep.2017.05.014.
- Calderaro J, Ziol M, Paradis V, Zucman-Rossi J. Molecular and histological correlations in liver cancer. J Hepatol. 2019; 71(3): 616-630. doi: 10.1016/j.jhep.2019.06.001.