
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Sarcoidosis mimicking lung cancer: Clinical image
Saori Nishizawa1*; Kazunori Tobino1; Yuka Hiraki2; Kosuke Tsuruno1
1Department of Respiratory Medicine, Iizuka Hospital 3-83 Yoshiomachi, Iizuka, Fukuoka 820-0018, Japan.
2Department of Pathology, Iizuka Hospital, 3-83 Yoshiomachi, Iizuka, Fukuoka 820-0018, Japan.
*Corresponding Author : Saori Nishizawa
Department of Respiratory Medicine, Iizuka Hospital 3-83 Yoshiomachi, Iizuka, Fukuoka 820-0018, Japan.
Email: saori0219mimumimu@gmail.com
Received : Mar 08, 2024
Accepted : Mar 25, 2024
Published : Apr 01, 2024
Archived : www.jcimcr.org
Copyright : © Nishizawa S (2024).
Citation: Nishizawa S, Tobino K, Hiraki Y, Tsuruno K. Sarcoidosis mimicking lung cancer: Clinical image. J Clin Images Med Case Rep. 2024; 5(4): 2956.
Case presentation
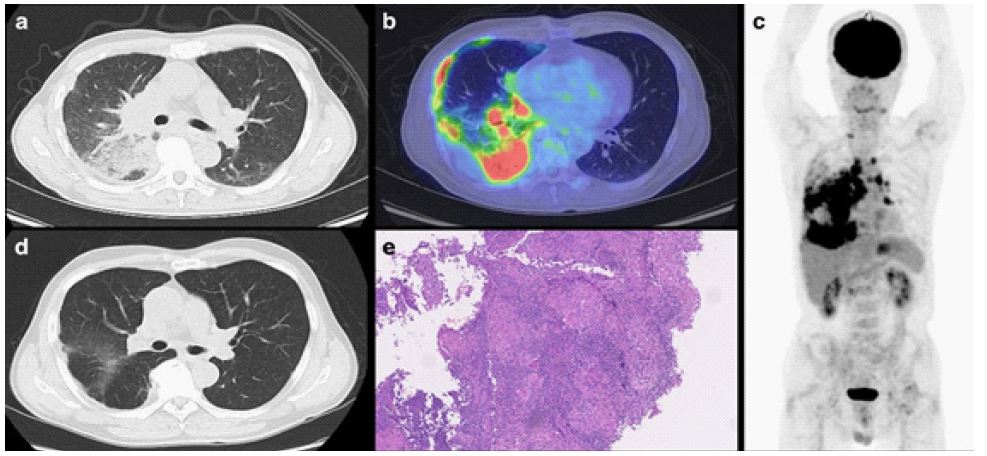
A 64-year-old Japanese male with no medical history presented with night sweats and fatigue for two weeks. Chest computed tomography showed multiple mediastinal and right hilar lymphadenopathy, right lower lobe consolidation, right pleural effusion, and right pleural thickening (Figure 1a). Considering lung cancer and malignant lymphoma, a thorough examination was conducted. Blood tests showed elevated soluble interleukin 2 receptors (2421 U/ml; normal, 121-621). 18-fluorodeoxyglucose positron emission/ computed tomography showed increased uptake in lesions seen on chest computed tomography and left hilar lymph nodes (Figures 1b and 1c). Endobronchial ultrasound-guided transbronchial needle aspiration was used to perform mediastinal lymph node biopsy and pathological examination revealed a non-necrotizing epithelioid cell granuloma. Surgical biopsies of the lymph nodes and right parietal pleura were performed to exclude malignancy, and both were histologically confirmed to be non-necrotizing epithelioid cell granulomas (Figure 1e). After examination of the heart, eyes, and nerves showed no sarcoidosis, pulmonary sarcoidosis was diagnosed. Symptoms resolved without treatment after a surgical biopsy and there was a marked reduction of lesions on computed tomography five months later (Figure 1d).
Since there have been case reports of sarcoidosis or sarcoid-like reactions complicating lung cancer [1,2], a definitive diagnosis should be made as carefully as possible.
Declarations
Acknowledgments: We thank Mr. Wade for the English language editing.
Funding: The authors have nothing to declare.
Conflict of interest: The authors declare that they have no competing interests.
Informed consent: The patient provided consent for the publication of this case report after the removal of all identifying information to retain anonymity and privacy.
Ethical approval: In this case report, ethical approval from the Institutional Review Board was not deemed necessary at our institution, and therefore, only an application was submitted. This study was conducted by the principles outlined in the Helsinki Declaration.
References
- Srinivasan M, Thangaraj SR, Arzoun H, Govindasamy Kulandaisamy LB, Mohammed L. The Association of Lung Cancer and Sarcoidosis: A Systematic Review. Cureus. 2022; 14(1): 21169.
- Yamaguchi M, Odaka M, Hosoda Y, Iwai K, Tachibana T. Excess death of lung cancer among sarcoidosis patients. Sarcoidosis. 1991; 8(1): 51-55.