
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Emphysematous kidney due to reno-duodenal fistula: An unusual cause of polymicrobial sepsis in a lung cancer patient
Nikhil Vojjala1*; Rishab Rajendra Prabhu1; Ibrahim Azar2; Geetha Krishanmoorthy1
1Department of Internal Medicine, Trinity Health Oakland/Wayne State University School of Medicine, Pontiac, Michigan, USA.
2Department of Hematology-Oncology, Trinity Health Oakland Hospital, Pontiac, Michigan, USA.
*Corresponding Author : Nikhil Vojjala
Department of Internal Medicine, Trinity Health Oakland/Wayne State University School of Medicine, Pontiac, Michigan, USA.
Email: [email protected]
Received : Mar 08, 2024
Accepted : Mar 26, 2024
Published : Apr 02, 2024
Archived : www.jcimcr.org
Copyright : © Vojjala N (2024).
Abstract
Sepsis in patients with underlying malignancies can be due to multifactorial such as infections due to neutropenia, pneumonia, and gastrointestinal infections. Fistula formation leading to sepsis is very rare. We would like to highlight an unusual cause (Reno-duodenal fistula of polymicrobial sepsis in an elderly patient with lung cancer through this case report.
Keywords: Lung cancer; Reno-duodenal fistula.
Citation: Vojjala N, Prabhu RR, Azar I, Krishanmoorthy G. Emphysematous kidney due to reno-duodenal fistula: An unusual cause of polymicrobial sepsis in a lung cancer patient. J Clin Images Med Case Rep. 2024; 5(4): 2958.
Case description
A 60-year-old man with a past medical history of hypertension, hyperlipidemia, and non-small cell lung cancer presented to the Emergency Department (ED) with a history of fever and chills of one-day duration. Family members reported that the patient was dull appearing and had difficulty in word finding, for the past week.
Oncological history: Of note, the patient’s non-small cell lung cancer initially responded well to systemic therapy, then became resistant to multiple lines of therapy including progression while on a clinical trial. The patient was then placed on Gemcitabine-based chemotherapy and underwent radiation therapy for right renal metastasis three months before index presentation as a palliative intent.
On presentation to the ED, he was febrile (103.6 F), hypotensive (blood pressure 70/50 mmHg), tachycardic (121/min), and hypoxic saturating 87% on room air. Physical examination revealed an ill-appearing man with tachypnoea. A neurological examination showed that he was disoriented with a Glasgow Coma Scale (GCS) of 13. Per abdominal examination showed right costovertebral angle tenderness with a resonant percussion note in the lower posterior thorax. He was resuscitated with intravenous fluids, and oxygen supplementation, and started on antibiotics as per sepsis protocol. Given his loin pain, a Computerized Tomography (CT) scan of the abdomen was done which showed a right upper pole renal mass. Air was seen within the right renal parenchyma, with a fistula between the C-loop of the duodenum and the anterior surface of the kidney (Figure 1A and 1B). Subsequently, Blood cultures grew multiple atypical organisms both bacteria and fungi. The bacteria isolated were Lactobacillus acidophilus, Streptococcus, and Leuconostoc mesenteroides, and the fungi were Saccharomyces Cerevisiae and Candida Albicans. The patient’s vital signs improved with fluid resuscitation and antibiotics initially. Esophagogastroduodenoscopy was done which showed a large fistulous opening in the duodenum extending into the kidney. Endoscopic closure of the fistulous opening was attempted but was not done due to adherence of the duodenum to the anterior wall of the kidney. Trans-esophageal echocardiogram did not show any vegetation. A CT scan brain and chest did show evidence of metastatic disease. Because of multiple medical comorbidities, poor performance status, and progressive disease, patient care was transitioned to hospice care.
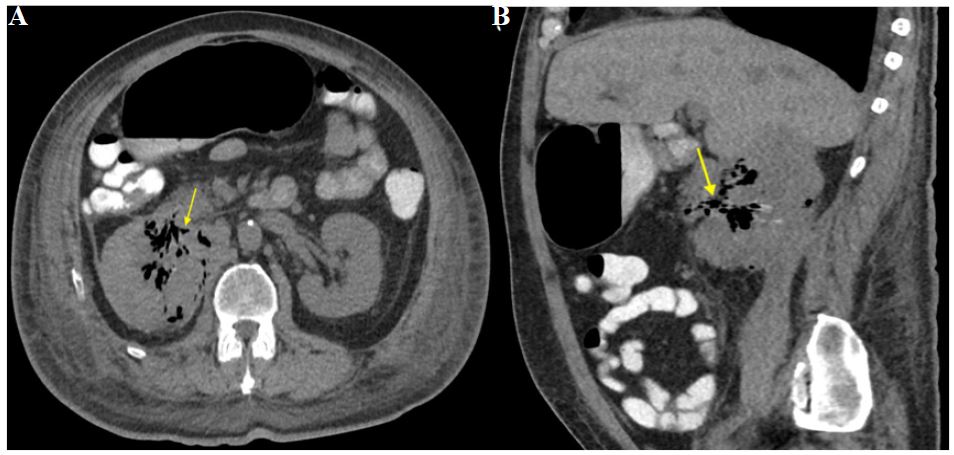
(B) Showing sagittal view showing fistulisation with duodenum (Yellow arrow).
Conclusion
Through this case report we would like to highlight a few points. Reno-duodenal fistula is a very rare and unusual cause of sepsis in patients with malignancy. Polymicrobial blood cultures and loin pain prompted us to think about gut translocation. Early identification may make surgical intervention possible. Though in this patient, we were not able to control the source of sepsis, endoscopic closure should be attempted, if possible, especially in poor surgical candidates. Poor performance status, diffuse metastatic disease, and recurrent hemodynamic instability excluded the surgical treatment options for this patient.