
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Surgery for a thoracic gunshot wound reveals pleural infection with dirofilaria repens
Isabelle Moneke1*; Anastasiya Kornyeva1; Leonie Braun3; Frederik Kukla3; Fabian Kohn4; Bernward Passlick1; Laurin Titze1
1Department of Thoracic Surgery, Medical Centre, University of Freiburg, Faculty of Medicine, University of Freiburg, Germany.
2Department of Microbiology, Medical Centre, University of Freiburg, Faculty of Medicine, University of Frei-burg, Germany.
3Veterinary Laboratory Freiburg, Germany.
4Department of Anaesthesiology and Critical Care Medicine, Medical Centre, University of Freiburg, Faculty of Medicine, University of Freiburg, Germany.
*Corresponding Author : Isabelle Moneke
Department of Thoracic Surgery, Medical Centre, University of Freiburg, Faculty of Medicine, University of Freiburg, Germany.
Email: Isabelle.moneke@uniklinik-freiburg.de
ORCID: 0000-0002-1019-5214.
Received : Mar 01, 2024
Accepted : Mar 27, 2024
Published : Apr 03, 2024
Archived : www.jcimcr.org
Copyright : © Moneke I (2024).
Abstract
Dirofilaria repens (D. repens) is a vector-borne filaroid helminth of carnivores, with dogs representing the major reservoirs of infestation. Humans are accidental hosts in which D. repens usually do not reach sexual maturity but may induce local inflammation, mainly in subcutaneous or ocular tissues. Here, we present the rare case of an incidental pleural D. repens infection in a young patient with a gunshot wound to the right upper chest. During thoracoscopy to remove the bullet from the dorsal chest wall, a small solitary worm was discovered in the pleural cavity on the diaphragm and later identified as D. repens. Our patient was asymptomatic regarding the parasite. D. repens is considered an emergent zoonotic pathogen in northern and central Europe and may be increasingly relevant for animals and human health. Spreading of the parasite is facilitated by climate changes and globalization.
Keywords: Dirofilaria repens; Human; Thoracic manifestation; Gunshot wound.
Citation: Moneke I, Kornyeva A, Braun L, Kukla F, Kohn F, et al. Surgery for a thoracic gunshot wound reveals pleural infection with dirofilaria repens. J Clin Images Med Case Rep. 2024; 5(4): 2961.
Introduction
Human dirofilariasis is a zoonotic vector-borne helminth disease caused by two species of Dirofilaria: Dirofilaria repens (D. repens) and Dirofilaria immitis (D. immitis). Human dirofilariosis is mostly asymptomatic, however it can become clinically apparent by nodules that appear when pre- adult/adult worms are arrested in a pulmonary artery branch in the case of D. immitis (pulmonary dirofilariosis) or in subcutaneous or ocular tissue in the case of D. repens (subcutaneous or ocular dirofilariosis), causing coagulation necrosis and inflammatory cells infiltration [1]. Dirofilaria are mosquito-transmitted nematodes primarily using domestic and wild canids, and to a lesser extent felines as principal reservoirs [2]. D. immitis has a world-wide distribution [3] and may cause severe and potentially fatal disease (heart worm disease) in dogs and other carnivores but rarely in hu-mans [3,4]. Despite humans being accidental hosts for both Dirofilaria species, D. repens shows higher zoonotic potential [5]. Over the last 2 decades, the prevalence of the clinically less noticeable D. repens has increased in its endemic areas and its distribution range has expanded to previously unaffected regions in northern and central Europe [3,6]. Thus, D. repens infection has become increasingly relevant, not only for animals, but also for human health. Humans are accidental hosts, and while the parasite does not normally reach adult stage in humans, it may live for several years [7]. In most cases, only 1 parasite develops [6] and the infection usually remains asymptomatic. D. repens mostly presents as subcutaneous or ocular dirofilariasis [7,9]. Rarely, local infection may appear, accompanied by a mild systemic reaction, e.g., fever or mild eosinophilia [10]. Even more rare are severe systemic immunoreactions [7]. However, in cases of sexual maturity, it may cause larva migrans syndrome and migrate to other organs, such as the abdominal cavity or the lungs [7,9]. The definite treatment is surgical removal of the parasite. Pharmacological treatment is usually not necessary [8], unless systemic infection is present and/or the worm cannot be surgically removed.
Case report
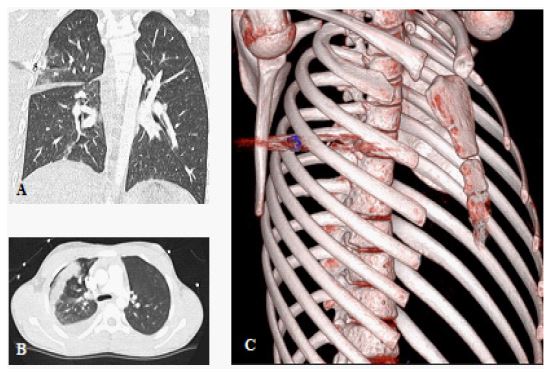
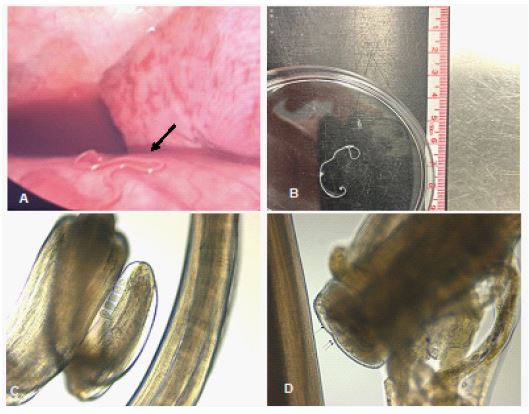
A 13-year-old male was admitted to our tertiary trauma center with a gunshot wound to the right upper chest caused by an air rifle accident. The CT-scan showed a penetrating gunshot wound with entry point of the projectile in the 4th ICR and consecutive traumatic injury to the right upper lobe with resulting hematopneumothorax (Figure 1). There was no evidence of active bleeding in the CT-scan, and the patient was hemodynamically stable. However, the bullet was stuck in the dorsal part of the chest wall. Therefore, we performed right-sided video-assisted thoracoscopy. First, we evacuated the hematoma and inspected the gunshot wound area in the dorsolateral chest wall. The projectile was divided into two parts which were stuck in the parietal pleura and could be recovered in total. The lung did not require suturing as the injury was superficial. After everything was cleaned up and the chest tube about to be placed, a winding formation suddenly appeared on the diaphragm, just below the right lower lobe. Upon closer inspection it was revealed to be a small translucent worm. The worm was removed alive and later identified as Dirofilaria repens by microscopic and molecular diagnosis at the veterinary reference institute (Figure 2). The patient was asymptomatic regarding the parasite. He was treated with mebendazole, a broad spectrum anthelmintic, for 3 days until the parasite was identified to be D. repens and the treatment was stopped. There was no evidence of a systemic reaction, e.g., no blood eosinophilia, or further clinical manifestation of D. repens. The patient made a full recovery and was discharged after 5 days. He had a history of traveling to Thailand and Italy for vacation a few months prior to the accident, however, the origin of the parasite remained unclear.
Discussion
To our knowledge, human D. repens manifestation in the pleural cavity is very rare. The current literature mostly consists of care reports and a few case series. Nematodes such as D. repens typically locate anywhere in the subcutaneous tissue or cause ocular dirofilariasis [3,9,11,12]. In the case of our patient, the pre-adult worm might simply have migrated as larva to end up in the pleural cavity, where it stayed. There was no indication for microfilaremia, although this cannot be ruled out, as we did not perform qPCR of a whole blood sample. Most human cases of dirofilariasis are asymptomatic and detected incidentally, just like in our patient. Over the last decade, an increasing number of cases was reported in previously unaffected areas in northern and central Europe [10,11,13]. Whether the number of cases has truly increased, or whether the detection of D. repens became significantly better, cannot be fully answered [2], however, there are several factors in favour of an actual spreading of the parasite. First and foremost, the climate change affecting mosquito vectors as well as globalization plays an important role in this expansion [7,9,14]. A higher annual mean temperature may contribute to accelerating the development of D. repens within the vector [7]. While our patient had travelled to Thailand and Italy for vacation within the last 2 years, he may very well have acquired the parasite in Germany. Many regions have already reached a periodically suitable climate for D. repens microfilariae to develop into infectious larvae, which might then be transmitted by mosquitoes [7].
Moreover, the import of dogs and the travel of dogs to endemic countries may contribute to the spread of the parasite, especially since many infected dogs remain undetected due to the subclinical nature of the disease [7,15]. Measures to control this infection should be focused on dogs and humans, as well as mosquitoes [8].
Conclusion
In conclusion, this case demonstrates an exceedingly rare case of pleural D. repens infection in a human. The available data are scarce and likely underestimate the number of cases, since dirofilariasis is usually not a notifiable disease [13]. Thus, further epidemiological studies are warranted to estimate the prevalence and incidence of D. repens infection in dogs, humans, or other hosts. Veterinarians as well as clinicians should become familiar with clinical manifestation of this emergent pathogen, because there will most likely be an increased number of cases in the future which may pose a relevant public health problem.
Declarations
Author contributions: IM and AK wrote the manuscript with input from LB, FK, FKu, BP and LT. FKu performed the morphological analysis of D. repens. All authors have read and approved the manuscript.
Patient consent statement: The patient’s and the patient’s parents’ informed consent for publication of the case report was obtained. Both parents both signed the written consent form provided by the university clinic, which is in accordance with the guidelines of the local ethics committee. A separate voting is not needed.
Data availability statement: On reasonable request to the corresponding author the data used in this article will be shared.
Potential conflicts of interest: The authors have no financial conflict of interest or relevant disclosures related to this case report.
References
- Gonzalez-Miguel J, Rosario L, Rota-Nodari E, Morchon R, Simon F. Identification of immunoreactive pro-teins of Dirofilaria immitis and D. repens recognized by sera from patients with pulmonary and subcutaneous dirofilariosis. Parasitol Int. 2010; 59: 248-56.
- Kondrashin AV, Morozova LF, Stepanova EV, Turbabina NA, Maksimova MS, Morozov AE, Anikina AS, Morozov EN. Global Climate Change and Human Dirofilariasis in Russia. Int J Environ Res Public Health. 2022; 19.
- Genchi C, Kramer L. Subcutaneous dirofilariosis (Dirofilaria repens): an infection spreading throughout the old world. Parasit Vectors. 2017; 10: 517.
- Brindicci G, Santoro CR, Signorile F, Leone A, Di Ciaula G, Monno L, Angarano G. Subcutaneous Human Dirofilariosis By D. Repens In South Italy: A Case Report. New Microbiol. 2019; 42: 234-6.
- Gabrielli S, Mangano V, Furzi F, Oliva A, Vita S, Poscia R, Fazii P, Di Paolo J, Marocco R, Mastroianni CM, Bruschi F, Mattiucci S. Molecular Identification of New Cases of Human Dirofilariosis (Dirofilaria repens) in Italy. Pathogens. 2021; 10.
- Biasizzo H, Soba B, Ilovski F, Harlander M, Lukin M, Blatnik O, Turel M, Srpcic M, Kern I, Beovic B. Severe and Rare Case of Human Dirofilaria repens Infection with Pleural and Subcutaneous Manifestations, Slovenia. Emerg Infect Dis. 2022; 28: 2504-7.
- Capelli G, Genchi C, Baneth G, Bourdeau P, Brianti E, Cardoso L, Danesi P, Fuehrer HP, Giannelli A, Ionica AM, Maia C, Modry D, Montarsi F, Krucken J, Papadopoulos E, Petric D, Pfeffer M, Savic S, Otranto D, Poppert S, Silaghi C. Recent advances on Dirofilaria repens in dogs and humans in Europe. Parasit Vectors. 2018; 11: 663.
- Redon-Soriano M, Blasco A, Gomila B, Gonzalez-Sanchez M, Simon F, Esteban JG. Subconjunctival human dirofilariasis by Dirofilaria repens in the Mediterranean Basin. Am J Ophthalmol Case Rep. 2022; 26: 101570.
- Miterpakova M, Antolova D, Ondriska F, Gal V. Human Dirofilaria repens infections diagnosed in Slovakia in the last 10 years (2007-2017). Wien Klin Wochenschr. 2017; 129: 634-41.
- Mateju J, Chanova M, Modry D, Mitkova B, Hrazdilova K, Zampachova V, Kolarova L. Dirofilaria repens: emergence of autochthonous human infections in the Czech Republic (case reports). BMC Infect Dis. 2016; 16: 171.
- Salamatin RV, Pavlikovska TM, Sagach OS, Nikolayenko SM, Kornyushin VV, Kharchenko VO, Masny A, Cielecka D, Konieczna-Salamatin J, Conn DB, Golab E. Human dirofilariasis due to Dirofilaria repens in Ukraine, an emergent zoonosis: epidemiological report of 1465 cases. Acta Parasitol. 2013; 58: 592-8.
- Balendran T, Yatawara L, Wickramasinghe S. Human Dirofilariasis Caused by Dirofilaria repens in Sri Lanka from 1962 to 2020. Acta Parasitol. 2022; 67: 628-39.
- Deksne G, Jokelainen P, Oborina V, Lassen B, Akota I, Kutanovaite O, Zaleckas L, Cirule D, Tupits A, Pim-anovs V, Talijunas A, Krumina A. The Zoonotic Parasite Dirofilaria repens Emerged in the Baltic Countries Estonia, Latvia, and Lithuania in 2008-2012 and Became Established and Endemic in a Decade. Vector Borne Zoonotic Dis. 2021; 21: 1-5.
- Geissler N, Ruff J, Walochnik J, Ludwig W, Auer H, Wiedermann U, Geissler W. Autochthonous Human Dirofilaria repens Infection in Austria. Acta Parasitol. 2022; 67: 1039-43.
- Genchi C, Kramer LH. The prevalence of Dirofilaria immitis and D. repens in the Old World. Vet Parasitol. 2020; 280: 108995.