
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Hydrocephalus as a rare presentation of neurosarcoidosis
Agnes T Stauning*; Carl C Larsen; Anders V Holst
Department of Neurosurgery, Copenhagen University Hospital, Inge Lehmanns Vej 6, 2100 Copenhagen, Denmark.
*Corresponding Author : Agnes T Stauning
Department of Neurosurgery, Copenhagen University Hospital, Inge Lehmanns Vej 6, 2100 Copenhagen, Denmark.
Email: tving.stauning@regionh.dk
Received : Mar 10, 2024
Accepted : Mar 28, 2024
Published : Apr 04, 2024
Archived : www.jcimcr.org
Copyright : © Stauning AT (2024).
Abstract
Background: Neurosarcoidosis represents a rare manifestation of sarcoidosis, with hydrocephalus occurring in only 5-9% of cases.
Observation: A 56-year-old female presented with severe hydrocephalus. Initial management involved a third ventriculostomy. Subsequent diagnostic evaluations confirmed neurosarcoidosis. However, before initiating medical treatment, recurrent hydrocephalus required reopening of the third ventriculostomy. The patient is currently undergoing a therapeutic regimen comprising methotrexate and infliximab, no new manifestations of hydrocephalus were observed following the reoperation.
Conclusion: In cases where obstructive hydrocephalus is associated with neurosarcoidosis, the prompt initiation of steroid treatment is imperative. Delays may contribute to the risk of relapse, underscoring the importance of timely medical management.
Keywords: Hydrocephalus; Neurosarcoidosis; Third ventriculostomy; Aqueductal stenosis; Ventriculoperitoneal shunt.
Citation: Stauning AT, Larsen CC, Holst AV. Hydrocephalus as a rare presentation of neurosarcoidosis. J Clin Images Med Case Rep. 2024; 5(4): 2965.
Introduction
Sarcoidosis is a multisystemic disease characterized by non-infectious granulomas. Sarcoidosis is most commonly observed in the lungs or cutaneous tissues [1]. In 5-10% of cases, the disease may spread to the nervous system, resulting in neurosarcoidosis [2,3]. Isolated neurosarcoidosis without systemic manifestations is extremely rare, occurring in less than 1% [4]. Untreated neurosarcoidosis can lead to severe neurological deficits ranging from mild paresis to death [5]. The most common presentation of neurosarcoidosis is cranial neuropathies whereas facial nerve palsy is the most frequent. Only 5-9% of patients develop hydrocephalus, the majority of these patients already had the diagnosis of sarcoidosis [2,3]. We here present a case of sarcoidosis manifesting with hydrocephalus which is extremely rare.
Case presentation
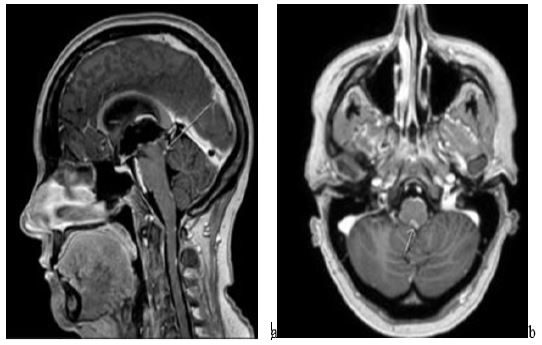
The case involves a 56-year-old woman with a past medical history of Ménière’s disease. She presented with fatigue, frontal headache, and vomiting in connection with food intake. Additionally, she had vertigo for one and a half years. In a clinical context, she presented with confusion, a broad-based gait, an unsteady tandem gait, and a positive Romberg test. Initially, she was diagnosed with exacerbation of Ménière’s disease, but a CT scan was performed for differential diagnostic purposes. The CT scan revealed severe supratentorial hydrocephalus. Subsequent MRI demonstrated aqueductal stenosis and multiple small contrast-enhancing lesions (Figure 1a-b). She was transferred to the neurosurgical department, where a third ventriculostomy was performed. During the procedure, small epidermal lesions were seen, and a biopsy was taken. The third ventriculostomy eased the patient’s symptoms. Subsequent investigation with an MR neuroaxis revealed multiple leptomeningeal changes (Figure 2). Carcinomatosis was suspected, leading to a CT scan of the thorax and abdomen, which showed enlarged mediastinal lymph nodes and a polyp in the intestine. Consequently, bronchoscopy with biopsy and colonoscopy were performed.
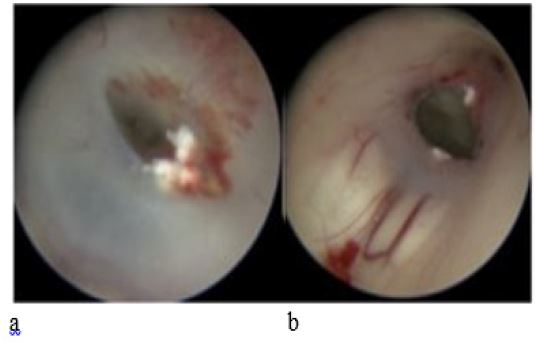
Both examinations revealed normal findings. The biopsy from the third ventriculostomy showed inflammation with some granulomatous features, and the biopsy from the bronchial mucosa demonstrated non-necrotizing granulomatous inflammation without signs of malignancy. Additionally, she underwent lumbar puncture and blood tests. The lumbar puncture showed mononuclear pleocytosis and elevated protein levels, but no cells suspicious for malignancy or signs of infection. Blood tests showed elevated interleukin-2 receptor but were otherwise normal. Six weeks after admission, she was referred to rheumatologists due to suspected neurosarcoidosis. Before treatment could be initiated, she began experiencing fatigue, confusion, and headaches again. Treatment with prednisolone was initiated, and a CT scan once again revealed hydrocephalus. She was readmitted to the neurosurgical department and underwent the placement of an External Ventricular Drain (EVD) for acute relief, which alleviated her pressure symptoms. Subsequent MRI revealed partial closure of the third ventriculostomy. This was addressed through a reoperation, during which the ventriculostomy was reopened (Figure 3a-b). The patient has subsequently commenced a therapeutic regimen comprising methotrexate and infliximab. No novel manifestations of hydrocephalus have been observed post-reoperation

Discussion
In 2018, diagnostic criteria for neurosarcoidosis were established, requiring verified neurosarcoidosis to involve a biopsy from nerve tissue containing granulomas [1]. Obtaining a biopsy from nerve tissue is often challenging. Therefore, the majority of patients with known systemic sarcoidosis who experience neurological symptoms are often treated for “possible or probable neurosarcoidosis”. A biopsy can be achieved through the performance of a third ventriculostomy. However, in our case, the biopsy initially did not show granuloma formation, preventing the establishment of a diagnosis. Consequently, it was necessary to rule out conditions such as malignancy before initiating treatment. In our case, the lack of timely treatment with steroids resulted in partial closure of the ventriculostomy. Normally closure of ventriculostomy is extremely rare. In our case, granuloma formation is presumed to be a contributing factor for closure. After the patient started treatment with steroids and later immunomodulatory therapy, she did not have a relapse of hydrocephalus (>3 months).
A study from 2023 investigated the use of ventriculoperitoneal shunts in the treatment of neurosarcoidosis-induced hydrocephalus [6]. Twenty-two patients had hydrocephalus and thirteen patients required a ventriculoperitoneal shunt in addition to medical treatment. Despite active medical treatment for neurosarcoidosis, 38.5% of patients required shunt revision, mostly due to shunt malfunction. Dam et al. described that 91% of patients treated medical for neurosarcoidosis-associated hydrocephalus needed surgical treatment in addition, 80% of the patients experienced a recurrence after the surgical procedure [7]. The majority (80%) were treated with a ventriculoperitoneal shunt. The increased protein content in Cerebrospinal Fluid (CSF) in neurosarcoidosis may be associated with an elevated risk of shunt dysfunction leading to recurrent hydrocephalus and subsequent shunt revisions; however, further studies are required to assess this. Several case reports have described favorable outcomes using third ventriculostomy as a treatment for hydrocephalus due to neurosarcoidosis [8,9]. If the ependymal lining of the ventricles is affected, third ventriculostomy also provides the opportunity to obtain a biopsy to confirm the diagnosis and initiate treatment at an earlier stage.
Conclusion
Hydrocephalus as the initial symptom of sarcoidosis is rare. Treatment with third ventriculostomy should be favored over Ventriculoperitoneal (VP) shunt placement, as it provides the opportunity to simultaneously perform a biopsy. Biopsy is essential for establishing the definitive diagnosis of neurosarcoidosis. Initiation of steroid treatment is crucial and should be started early on, as a delayed intervention may lead to a relapse of hydrocephalus due to the closure of the third ventriculostomy.
Declarations
Funding: No funding was received for this research.
Conflicts of interest/competing interests: All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest, or non-financial interest in the subject matter or materials discussed in this manuscript.
Availability of data and material: not applicable.
Code availability: not applicable.
Authors’ contributions: All authors contributed to the study conception and design. The first draft of the manuscript was written by Agnes T. Stauning, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Ethics approval: Informed consent was obtained from the participant included in the study.
Consent to participate/Consent for publication: The participant has been contacted, presented with this article, and has consented to the use of clinical information and images for publication.
References
- Stern BJ, Royal W, Gelfand JM, et al. Definition and Consensus Diagnostic Criteria for Neurosarcoidosis: From the Neurosarcoidosis Consortium Consensus Group. JAMA Neurol. 2018; 75(12): 1546-1553.
- Fritz D, van de Beek D, Brouwer MC. Clinical features, treatment and outcome in neurosarcoidosis: Systematic review and meta-analysis. BMC Neurol. 2016; 16(1): 1-8.
- Nowak DA, Widenka DC. Neurosarcoidosis: A review of its intracranial manifestation. J Neurol. 2001; 248(5): 363-372.
- Smith JK, Matheus MG, Castillo M. Imaging Manifestations of Neurosarcoidosis. American Journal of Roentgenology. 2004; 182(2): 289-295.
- Nozaki K, Judson MA. Neurosarcoidosis: Clinical manifestations, diagnosis and treatment. Presse Medicale. 2012; 41: 331-348.
- El Sammak S, Lec BM, Bou GA, Wagstaff W V., Lawson EC, Hutto SK. Hydrocephalus in Neurosarcoidosis: Clinical Course, Radiographic Accompaniments, and Experience with Shunting. Mult Scler Relat Disord. 2023; 79: 105040.
- ten Dam L, van de Beek D, Brouwer MC. Clinical characteristics and outcome of hydrocephalus in neurosarcoidosis: a retrospective cohort study and review of the literature. J Neurol. 2022; 269(5): 2727-2733.
- Togashi S, Maruya J, Abe H, et al. Endoscopic Management for Recurrent Hydrocephalus Associated with Neurosarcoidosis. World Neurosurg. 2020; 144: 121-124.
- Nakayasu H, Shirai T, Tanaka Y, Sato T, Muro H. Neurosarcoidosis Presenting with Obstructive Hydrocephalus Successfully Treated with Endoscopic Third Ventriculostomy. Intern Med. 2019; 58: 105-108.