
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Excimer laser for tilted embedded inferior venal caval filter retrieval: A case report
Francesco Gallo, MD1; Paolo China, MD1; Gianpiero D Amico, MD, PhD1*; Andrea Panza, MD2;
Giovanni Vescovo, MD1;
Ada Cutolo, MD1; Marco Barbierato, MD1; Sakis Themistoclakis, MD1;
Federico Ronco, MD1
1Department of Cardio-Thoracic, Cardiology Unit, Vascular Medicine and Intensive Care, Ospedale Dell Angelo, Mestre, Venezia, Italy.
2Department of Cardiac, Thoracic, Vascular Sciences and Public Health, University of Padua, Italy.
*Corresponding Author : Gianpiero D Amico
Department of Cardio-Thoracic, Cardiology Unit, Vascular Medicine and Intensive Care, Ospedale Dell Angelo, Mestre, Venezia, Italy.
Tel: +393381264764
Email: gianpiero.damico@hotmail.it
Received : Mar 11, 2024
Accepted : Mar 29, 2024
Published : Apr 05, 2024
Archived : www.jcimcr.org
Copyright : © Amico GD (2024).
Abstract
The retrieval of Inferior Vena Cava Filters (IVCF) has become an increasingly significant concern, especially with the expanding use for filter implantations itself. Dwell time is a predictor of device-related complications and failure of standard retrieval techniques. Additionally, no specific devices for retrieval are available on the market whereby the use of alternative tools are growing up. We report a case of IVCF recapture using excimer laser after multiple unsuccessful attempts with common technique, which could represent a novel approach in complex cases.
Keywords: Caval filter; Pulmonary embolism; Inferior vena cava; Removal; Excimer laser.
Citation: Gallo F, China P, Amico GD, Panza A, Vescovo G, et al. Excimer laser for tilted embedded inferior venal caval filter retrieval: A case report. J Clin Images Med Case Rep. 2024; 5(4): 2966.
Introduction
Venous Thromboembolism (VTE), clinically presenting as Deep Vein Thrombosis (DVT) or Pulmonary Embolism (PE), is the third most frequent acute cardiovascular syndrome behind myocardial infarction and stroke [1]. VTE is considered to be a consequence of the interaction between permanent patient-related risk factors and temporary setting-related risk factors: surgery and prolonged bed rest are two of well-known risk factors that played an important role in our case. The anticoagulation was the fulcrum of the therapy in VTE but often challenging scenarios must be faced, in which the balance between thrombosis and bleeding risk is very difficult to determine. The 2019 ESC/ERS Guidelines on acute PE suggests that Inferior Vena Cava Filter (IVCF) should be considered in patients with acute PE and absolute contraindication to anticoagulation or in cases of PE recurrence despite anticoagulation therapy (both have a IIa indications with level of evidence C). The widespread recommendation to implant a venous filter in patients with a recent (within one month) proximal DVT and an absolute contraindication to anticoagulant therapy primarily stems from the perceived elevated risk of recurrent PE in this scenario, coupled with the absence of alternative treatment choices [2]. The aim of using caval filters is to mechanically stop the spread of venous clots to the pulmonary circulation. IVCF is only a temporary therapy helping to prevent PE recurrence until the risk factors were eliminated, thus multiple withdrawal techniques have developed, ranging from the use of snares, loops with guides, balloons and flossing or endobronchial forceps [3]. Among these techniques, the use of the excimer laser has been emerging in recent years. The excimer laser sheath was initially granted approval from FDA for removing long-term implanted pacemaker or defibrillator leads. This device employs 308-nm UV laser energy to ablate tissues around cardiac leads, making it easier to extract them from vascular and cardiac binding sites. Over the past decade, several physicians have documented successful off-label usage of the laser sheath for IVC filter retrieval in individual research studies. Similar to lead management procedures, the laser sheath enables the ablation of fibrous tissue surrounding the IVC filters, reducing the force needed to retrieve the filter. Histological analyses of extracted filters, available in the literature, reveal neointimal hyperplasia as the underlying mechanism for the formation of these adherent structures. This suggests that although there is a risk of significant vascular damage, it is limited [4,5].
Case description
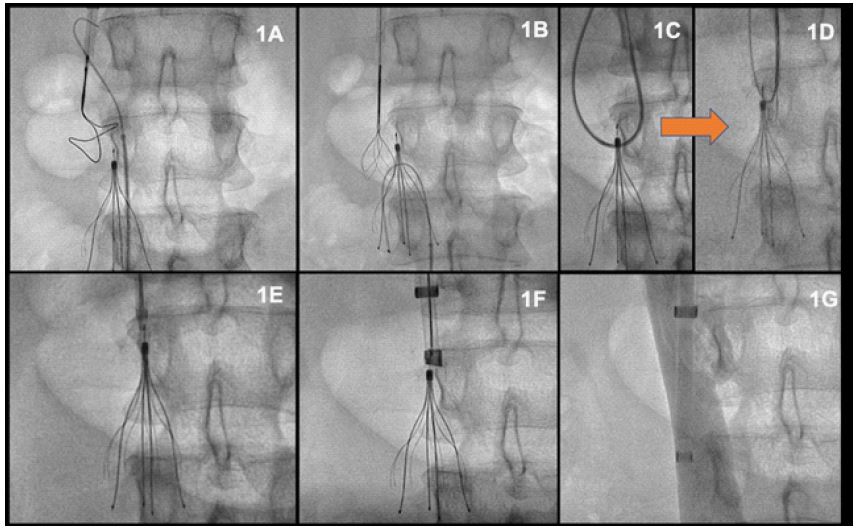
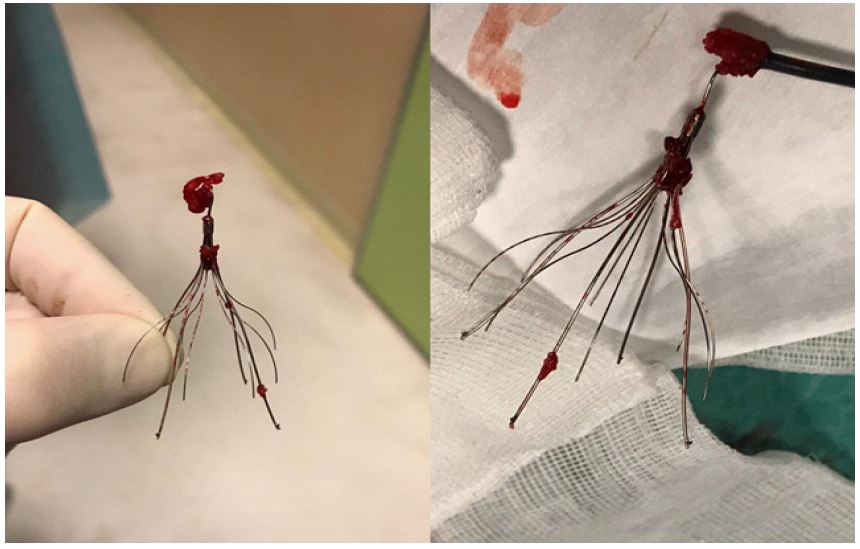
case presents a compelling scenario of a 28-years old male with no previous medical history who was admitted to our hospital in October 2020 for worsening headache and sleepiness. A cerebral computed tomography showed a vast cerebral cavernous malformation located at the left parietal side, complicated by intralesional bleeding. Because of quickly neurological deterioration, the patient underwent an urgent neurosurgical intervention leading to the lesion removal. During the in-hospital stay, after surgery, the patient experienced a hemodynamically stable PE, with an intermediate-high risk of mortality according to the guidelines (increased cardiac biomarkers, right ventricular dysfunction and sPESI >1). In the diagnostic work-up an echo-color Doppler of lower limb was performed and showed a DVT of right popliteal vein. For this reason, patient needed an anticoagulation therapy which was, however, contraindicated due to recent brain surgery associated with an intralesional bleeding. We managed to implant a removable vena cava filter (Cook, Bloomington, IN; USA). Procedure was performed through the right jugular vein and the IVCF was implanted without any complications. We planned a 3-months follow-up, in which patient recovered from symptoms, a new echo-color Doppler of lower limb veins showed a restored flow through the right popliteal vein without signs of DVT and an echocardiography revealed a normal right ventricle dimension and function. Given the full recovery, in February 2021, we decided to perform the first caval filter removal attempt. Unexpectedly, we found that the hook of the filter was tilted against the vein’s wall, and any attempt to recapture it, using the standard snaring techniques, failed because of strong adherence between the hook and the caval wall itself (Figures 1A-B). So, we decided to make another attempt using the “snare-over-guidewire technique” using a Judkins right 3.5 guiding catheter (Medtronic, Minneapolis, MN; USA) that was advanced on a “0.035 iodophilic wire (Terumo; Tokyo, Japan) and through the filter’s struts (Figure 1C) in order to create a guidewire loop, which was then snared and brought out of the internal jugular sheath. A snare loop has been advanced on this system to increase the possibility of capturing, but even this technique failed to recapture the filter because of heavy adherences. Then, we tried to advance a coaxial sheath system (Cook, Bloomington, IN; USA), that was manipulated simultaneously in a twisting way (Figure 1E) in order to dissect the adhesions between the filter and the caval wall in a so-called “double-sheath dissection technique”. Unfortunately, the adherences between the caval wall and, once again, the filter’s hook were impossible to dissect. Finally, we decided to dissolve the adherences using a 14 Fr GlideLight excimer laser (Philips; Amsterdam, Netherlands) inserted over the filter capture device through a right internal jugular vein access. Initially we decide to use a stepwise approach in which the first laser emission was with a low dose energy delivery (40 mJ of fluence, 25 mm/Hz repetition rate) and using saline infusion, in order to reduce any potential adverse events. After this first attempt, many adherences were already dissected but the filter seemed to be still trapped against the vein’s wall. Then, a new excimer laser delivery was carried out with higher energy (60 mJ of fluence and 40 mm/Hz repetition rate) and using a saline-free solution (blood) achieving a complete ablation of fibrotic tissue (Figure 1F) and obtaining a complete separation of the filter from the caval wall. Successively, the filter was easily snared and removed from the same access without any complication (Figures 1G and 2). The patient has been discharged at home after two days. We planned a 3-months and 1-year follow-up of the patient in which he was completely asymptomatic and no events was recorded, even without anticoagulation therapy.
Discussion
IVCF are commonly implanted to provide protection from pulmonary embolism in patients who cannot receive anticoagulation [6,8]. Dwell time for IVCF is more likely to be associated with and increased risk of significant device-related complications such as device thrombosis and subsequent IVC occlusion, extravascular filter legs and migration [9,10]. Prolonged time for IVCF could favour adherence formation between caval wall and filter’s components and likely to fail retrieval with standard techniques, which could fail in up to 28% of the cases, according to literature [10,11]. In these cases, advanced devices or techniques, such as the “sling” technique or the use of rigid endobronchial forceps, are required to achieve successful retrieval [11]. However, the use of forceps is burdened by several complications, up to 5.3%, such as IVC pseudoaneurysm, traumatic arterio-venous fistula between the renal artery and IVC, and IVC rupture and the “sling” technique could be insufficient to retrieve an embedded or endothelized filter [12]. At the best of our knowledge, there are many data showing the efficacy of excimer laser in ICVF retraction. Kuo and colleagues [4] reported data on 251 consecutive patients who underwent IVCF implantation with a mean dwell time of 31 months were treated using laser-assisted filter retrieval after a first attempt with standard techniques; the technical success reported was high (99.2%), with a major complication rate of 1.6%. Moreover, in this study a force-gauge has been used during retrieval, demonstrating that use of the laser-sheath significantly decreased the force required compared with counter-traction techniques, hypothetically decreasing the risk of possible adverse events [13]. The register was further expanded to 500 patients enrolled until 2020, confirming again that laser-assisted procedure was associated with a success rate of 99.6%, a lower application of force for device recapture (laser-assisted group 3.6 lb vs. non-laser-assisted group 6.5 lb) and a 2% complication rate that was effectively treated with medical therapy alone [14]. In another registry, considering 441 patients, the excimer laser has been used to remove filters reaching high rates of technical success, despite an exceptionally long mean implantation time (56.6 months) [15]. The latest evidences in literature belong from the retrospective study from Desai et al.; this trial enrolled 265 patients from 7 American centres who underwent caval filter extraction by excimer laser sheath; the average dwell time was approximately 69 months. Even in this case, the results showed a high technical success rate (95.7%) with a major adverse event rate of 4.0%, (threshold were under 10%) although none of them were closely related to the device extracted [16]. Numerous reports of device-related adverse events associated with retrievable IVCF have been published: a systematic literature review [17] revealed penetration of the venous wall in 1699 (19%) of 9002 procedures; among these cases, 19% showed adjacent organ involvement, and ≥8% were symptomatic. Lethal complications were rare (only two cases), but 5% of the patients required major interventions such as surgical removal of the filter, endovascular stent placement or embolization, endovascular retrieval of the permanent filter, or percutaneous nephrostomy or ureteral stent placement. Further reported complications include filter fracture and/or embolization, and occasionally, DVT extending up to the vena cava [18,19]. It became very important to keep in mind that placement of this devices without timely retrieval has been linked to significant thrombotic complications, including filter-related acute venous thromboembolism, chronic caval occlusion, chronic DVT, and post-thrombotic syndrome - an incurable chronic condition. Consequently, patients with filters that cannot be removed are often managed with continuous anticoagulation to mitigate the risks associated with prolonged filter presence. However, this approach imposes additional costs, inconvenience, and bleeding risks associated with lifelong anticoagulation [20]. Despite its proven efficacy, the use of the excimer laser in such procedures requires careful patient selection. Factors such as significant tilt, a filter deeply embedded in the vessel wall, the presence of collateral vessels in the vicinity of the device, or a significant thrombotic burden within the filter must be carefully considered as they may lead to procedure failure or complications. A proper pre-procedural strategy for filter placement is also very important, taking into account the anatomy of the vena cava by performing venography before releasing the device. This will allow it to be aligned with the course of the vessel and avoid tilting. The indication for caval filter implantation should therefore be based not only on the current characteristics of the patient, but also by planning the exact timing and modalities of the subsequent retrieval. As suggested in the literature, retrieval modalities should always be based on a stepwise approach, in which the possible use of more complex techniques and devices should be discussed in a multidisciplinary team, as they may increase the time and complexity of the procedure itself. Here we have described a case of a young man in which the excimer laser has been safely and effectively used in retrieval a tilted and embedded filter against the IVC wall, after that all the attempts with standard snaring technique failed. It is therefore rational to argue that the development of new techniques in this field, such as the use of the excimer laser, will improve the procedure safety, outcomes and survival, particularly after prolonged dwell time. Implementing excimer laser-assisted IVCF retrieval in clinical practice involves significant resource implications, including the initial investment in equipment, ongoing maintenance costs, and specialized staff training. Procedural challenges include adapting workflows, coordinating scheduling, and addressing potential increases in procedural time. Successful integration requires strategic planning and resource optimization to ensure effective implementation.
Conclusion
The use of IVCF is expanding and the interest in the retrieval filed is growing up. The excimer laser could represent an important tool in retrieval of embedded inferior vena cava filters and appears to be a safe a feasible approach in difficult cases. In selected scenarios, such as tilted or embedded filter element or prolonged dwelling time, this technique may avoid the necessity for multiple attempts and use of further tools that requiring a lot of traction force that may lead to serious complications like, in the worst case, the vena cava rupture. While the evidence supporting this technique is expanding, it remains in the developmental stage. The existing data are derived from a small number of cases and retrospective studies. To enhance the reliability of the findings, it is crucial to conduct prospective and randomized trials. In addition, the experience and expertise of the operator play a key role in determining the feasibility and safety of using the excimer laser for IVCF retrieval. A skilled operator who is familiar with the intricacies of laser technology and IVCF retrieval procedures can enhance the precision and effectiveness of the laser application. The ability to assess patient-specific factors, anatomical variations and potential complications is critical to making informed decisions during the retrieval process. The potential long-term benefits of incorporating excimer laser assisted IVCF retrieval extend to both improved patient outcomes and potential cost-effectiveness within healthcare systems. The precision of the excimer laser in retrieval procedures may lead to a reduction in the need for repeat procedures, minimising associated risks and helping to improve the incidence of long-term complications associated with indwelling filters, such as migration, fracture or thrombosis. From a healthcare cost perspective, the streamlined and efficient nature of excimer laser-assisted retrieval could result in shorter procedure times and fewer complications. While recognising the potential economic benefits, it is important to weigh these against the upfront costs of implementing and maintaining excimer laser technology.
References
- Raskob GE, Angchaisuksiri P, Blanco AN, et al. A Major Contributor to Global Disease Burden n.d.
- Konstantinides SV, Meyer G, Bueno H, et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS): The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC). Eur Heart J 2020; 41(4): 543-603. Doi: 10.1093/EURHEARTJ/EHZ405.
- Kuyumcu G, Walker TG. Inferior vena cava filter retrievals, standard and novel techniques. Cardiovasc Diagn Ther 2016; 6(6): 642-50. Doi: 10.21037/cdt.2016.09.07.
- Kuo WT, Odegaard JI, Rosenberg JK, Hofmann LV. Laser-Assisted Removal of Embedded Vena Cava Filters. Chest 2017; 151(2): 417-24. Doi: 10.1016/j.chest.2016.09.029.
- Kuo WT, Odegaard JI, Rosenberg JK, Hofmann LV. Laser-Assisted Removal of Embedded Vena Cava Filters. Chest 2017; 151(2): 417-24. Doi: 10.1016/j.chest.2016.09.029.
- Kaufman JA, Kinney TB, Streiff MB, et al. Guidelines for the use of retrievable and convertible vena cava filters: Report from the society of interventional radiology multidisciplinary consensus conference. World Journal of Surgery. 2007; 31: 251-64.
- Decousus H. Eight-year follow-up of patients with permanent vena cava filters in the prevention of pulmonary embolism: The PREPIC (Prévention du Risque d’Embolie Pulmonaire par Interruption Cave) randomized study. Circulation. 2005: 416-22. Doi: 10.1161/CIRCULATIONAHA.104.512834.
- Sarosiek S, Crowther M, Sloan JM. Indications, complications, and management of inferior vena cava filters: The Experience in 952 Patients at an academic hospital with a level I trauma center. JAMA Intern Med. 2013; 173(7): 513-7. Doi: 10.1001/jamainternmed.2013.343.
- Marquess JS, Burke CT, Beecham AH, et al. Factors Associated with Failed Retrieval of the Günther Tulip Inferior Vena Cava Filter. Journal of Vascular and Interventional Radiology. 2008; 19(9): 1321-7. Doi: 10.1016/j.jvir.2008.06.004.
- Andreoli JM, Lewandowski RJ, Vogelzang RL, Ryu RK. Comparison of complication rates associated with permanent and retrievable inferior vena cava filters: A review of the MAUDE database. Journal of Vascular and Interventional Radiology. 2014; 25(8): 1181-5. Doi: 10.1016/j.jvir.2014.04.016.
- von Stempel C, Hague J, Brookes J. Excimer laser assisted complex inferior vena cava filter retrieval: a single institution’s experience over 6 years. Clin Radiol 2019; 74(1): 79.15-79.20. Doi: 10.1016/j.crad.2018.09.012.
- Laws JL., Lewandowski RJ., Ryu RK., Desai KR. Retrieval of Inferior Vena Cava Filters: Technical Considerations. Semin Intervent Radiol. 2016; 33: 144-8. Doi: 10.1055/s-0036-1582119.
- Kuo WT, Odegaard JI, Rosenberg JK, Hofmann L v. Laser-Assisted Removal of Embedded Vena Cava Filters: A 5-Year First-in-Human Study2017; 151: 417-24.
- Kuo WT, Doshi AA, Ponting JM, Rosenberg JK, Liang T, Hofmann L V. Laser‐Assisted Removal of Embedded Vena Cava Filters: A First‐In‐Human Escalation Trial in 500 Patients Refractory to High‐Force Retrieval. J Am Heart Assoc. 2020; 9(24). Doi: 10.1161/JAHA.119.017916.
- Desai KR, Xiao N, Salem R, Karp JK, Ryu RK, Lewandowski RJ. Excimer laser sheath–assisted retrieval of “closed-cell” design inferior vena cava filters. J Am Heart Assoc. 2020; 9(17). Doi: 10.1161/JAHA.120.017240.
- Desai KR, Kaufman J, Truong P, et al. Safety and Success Rates of Excimer Laser Sheath–Assisted Retrieval of Embedded Inferior Vena Cava Filters. JAMA Netw Open 2022; 5(12): 2248159. Doi: 10.1001/jamanetworkopen.2022.48159.
- Jia Z, Wu A, Tam M, Spain J, McKinney JM, Wang W. Caval Penetration by Inferior Vena Cava Filters: A Systematic Literature Review of Clinical Significance and Management. Circulation 2015; 132(10): 944-52. Doi: 10.1161/CIRCULATIONAHA.115.016468.
- Durack JC, Westphalen AC, Kekulawela S, et al. Perforation of the IVC: rule rather than exception after longer indwelling times for the Günther Tulip and Celect retrievable filters. Cardiovasc Intervent Radiol. 2012; 35(2): 299-308. Doi: 10.1007/s00270-011-0151-9.
- Angel LF, Tapson V, Galgon RE, Restrepo MI, Kaufman J. Systematic review of the use of retrievable inferior vena cava filters. J Vasc Interv Radiol. 2011; 22(11): 1522-1530.e3. Doi: 10.1016/j.jvir.2011.08.024.
- Hajduk B, Tomkowski WZ, Małek G, Davidson BL. Vena Cava Filter Occlusion and Venous Thromboembolism Risk in Persistently Anticoagulated Patients. 2010; 137(4): 877-82. Doi: 10.1378/chest.09-1533.