
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Chediak-Higashi syndrome with hemophagocytic cells in CSF
Samin Alavi*; Roghayeh Rahimi Afzal; Fatemeh Dastmalchi
Pediatric Congenital Hematologic Disorders Research Center, Research Institute for Children’s Health, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
*Corresponding Author : Samin Alavi
Pediatric Congenital Hematologic Disorders Research Center, Research Institute for Children’s Health, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Email: saminalavi@hotmail.com
Received : Mar 11, 2024
Accepted : Apr 01, 2024
Published : Apr 08, 2024
Archived : www.jcimcr.org
Copyright : © Alavi S (2024).
Abstract
An infant with Chediak-Higashi syndrome is presented who developed hemophagocytic lymphohistiocytosis (HLH). During the initial evaluations, CSF was analyzed which showed abnormal leukocytes and monocytes with giant granules and hemophagocytosis.
Citation: Alavi S, Afzal RR, Dastmalchi F. Chediak-Higashi syndrome with hemophagocytic cells in CSF. J Clin Images Med Case Rep. 2024; 5(4): 2970.
Case presentation
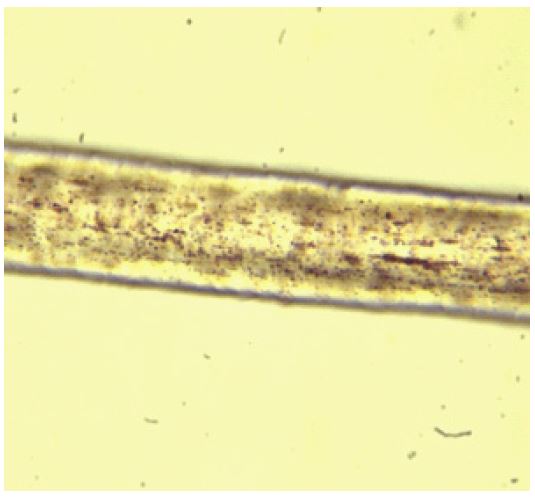
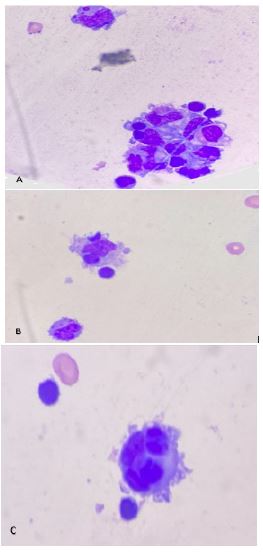
50-day-old male infant; born of a first-degree consanguineous parent, was referred for repair of umbilical hernia. Due to severe pancytopenia, he was consulted with pediatric hematology clinic. On physical examination, light-colored skin, blonde hair and eyelashes (Figure 1), and huge hepatosplenomegaly causing protruding umbilicus was observed. Hematologic findings were positive for severe pancytopenia (Hemoglobin 6.5 g/L, platelets 24×109 /L, leukocytes 1.9×109 /L). Peripheral blood smear showed abnormal large granules in leukocytes. According to pancytopenia, marked hepatosplenomegaly, light skin and hair color, and abnormal giant granules in neutrophils, Chediak-Higashi syndrome (CHS) was suggested for the patient. Clumps of the melanin pigment within the hair shaft were visualized under the light microscope which confirmed the diagnosis of CHS (Figure 2). The observation of hemophagocytic cells in bone marrow aspiration, low percentage of natural killer cells in flow cytometry, hyperferritinemia and hypofibrinogenemia fulfilled the criteria for diagnosis of accelerated phase of HLH. The patient was checked for viral infections by PCR, which was found to be negative for EBV and CMV. CSF examination of the patient showed typical neutrophils and monocytes with giant granules along with hemophagocytosis (Figure 3). HLH-2004 protocol including dexamethasone, IVIG and cyclosprin was started for the patient. He was also scheduled to receive CNS directed therapy, considering the observation of hemophagocytic cells in the CSF. Unfortunately, the patient expired due to severe bacterial infection and septicemia.

Discussion
Chediak Higashi syndrome (CHS) is a rare autosomal recessive syndrome that was first described by Cesar in 1943. Then, Chediak in 1952 and Higashi in 1954 reported two other cases [1]. The underlying defect in CHS is a mutation in the LYST or the CHS1 gene which is responsible for the regulation of lysosomal trafficking and assemble of cytoplasmic granules. The LYST gene is located on the long arm of chromosome 1. Chediak-Higashi syndrome (CHS) is characterized by partial oculocutaneous albinism, immunodeficiency, and a mild bleeding tendency. Approximately 85% of affected individuals develop the accelerated phase, or hemophagocytic lymphohistiocytosis [2].
This is the first report of an infant with CHS who showed abnormal neutrophils and hemophagocytosis in the CSF.
Declarations
Ethical Approval: The authors got informed consent from the parents regarding use of the patient’s photos.
Funding: This was an image of hematology and there was no funding required.
References
- Vaillant AAJ, CM. Stang, Lymphoproliferative Disorders, in StatPearls [Internet]. StatPearls Publishing. 2022.
- Toro C, et al. Chediak-Higashi Syndrome, in Gene Reviews® [Internet]. University of Washington, Seattle. 2023.