
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Long-standing hamstring and pelvic pain in a professional basketball player with pelvic malalignment syndrome; The role of detailed biomechanical assessment
Vahid Seifi1*; Farzin Halabchi2; Marzieh Mahmoudi Zarandi1
1Sports Medicine Research Center, Neuroscience Institute, Tehran University of Medical Sciences, Tehran, Iran.
2Sports and Exercise Medicine Department, Imam Khomeini Hospital, Tehran University of Medical Sciences, Tehran, Iran.
*Corresponding Author : Vahid Seifi
Sports Medicine Research Center, Neuroscience Institute, Tehran University of Medical Sciences, Tehran, Iran.
Tel: +98-9171894368,
Email: Vahidseifi@razi.tums.ac.ir
Received : Mar 04, 2024
Accepted : Apr 02, 2024
Published : Apr 09, 2024
Archived : www.jcimcr.org
Copyright : © Seifi V (2024).
Abstract
A 17-year-old former basketball player with refractory and long-standing hamstring and pelvic pain was referred to our clinic. Many interventions, such as ninety sessions of physical therapy and Platelet-rich plasma injections were performed for him, so he gave up basketball. We performed detailed biomechanical assessments and gait analysis. Based on the findings, we performed injections under the C-arm guide. A stabilizing pelvic belt was prescribed, and five sessions of muscle energy techniques and pelvic mobilization in the clinic and self-mobilization at home were performed. After four months, the patient recovered from the pain successfully.
Keywords: Pelvic Malalignment; Biomechanical Assessment; Gait Analysis.
Citation: Seifi V, Halabchi F, Zarandi MM. Long-standing hamstring and pelvic pain in a professional basketball player with pelvic malalignment syndrome; The role of detailed biomechanical assessment. J Clin Images Med Case Rep. 2024; 5(4): 2973.
Introduction
Malalignment syndrome refers to the biomechanical changes, signs, and symptoms consistently seen in any part of the pelvic bone of the normal kinetic chain. The syndrome may result in abnormal biomechanical stresses that can compromise the ability to deal with forces and cause chronic and longstanding lower extremity complaints [1,2]. Interventions directed to correct these abnormalities may positively affect the clinical outcomes.
Case presentation
A 17-year-old male, a former professional basketball player, was referred to our clinic due to hamstring and pelvic pain that started 3 years ago. Despite previous evaluations and treatments, the pain did not improve and his quality of life was disturbed dramatically, so he gave up sports 2 years ago.
The non-radicular pain started gradually, initially in the right buttock, and then progressed to severe bilateral pain (Numerical pain rating scale (NRPS) = 8/10). The pain was exacerbated with squat and lung exercises and during decelerations, but he had no problem with jogging. No paresthesia was reported in the lower limbs. The pain improved with periods of resting from sports. In the first three months, the cryotherapy and NSAIDs reduced pain (NPRS = 5/10). Low back pain and coccydynia developed after 1 year, that is why he gave up basketball. He went to a rheumatologist and tried a course of corticosteroids, and the specialist ruled out rheumatologic diseases. One year ago, he tried two PRP injections in the hamstring tendon insertion to the Ischial bone, but the pain did not change significantly (NPRS /10). Orthopedic consultations did not reveal any specific problem, and more than 100 sessions of physiotherapy (dry needling, electrotherapy, and manipulation) during this period did not improve the pain.
Past Drug History: Diclofenac sodium, Naproxen, Celecoxib, Gabapentin, Prednisone. Physical Examinations: Tenderness in the para-spinal region (L3 – L5), SI joints (especially on the right side), coccyx, and hamstring insertion to the ischial bone. Other specific clinical examinations are summarized in Table 1.
Table 1: The course of endoscopic treatments.
| No. | Parameter | Test | Variable | Value* | Interpretation | |
|---|---|---|---|---|---|---|
| Left | Right | |||||
| Range of motions/ Muscle tightness & strength tests | ||||||
| 1 | Hip ROM (Flexion,Extension) |
Goniometricmeasurement | Degree | 115/18 | 117/20 | Normal |
| 2 | Knee ROM (Extension, Active Flexion, PassiveFlexion) | Goniometric measurement | Degree | 0/140/140 | 0/140/140 | Normal |
| 4 | Gastrocnemius tightness | Silfverskiöldtest | Qualitative | - | - | Normal |
| 6 | Hamstring tightness | Conventional Popliteal angle | Degree | -30° | -32° | Positive |
| 7 | Hip flexorstightness | Thomas test | Degree | + | + | Tight hipflexors |
| 8 | Tibial Torsion | Thigh-Foot Angle | Degree | 5° | 6° | Normal |
| 9 | Hip Version | Craig's Test | Qualitative | Retroversion | Retroversion | Both hipsretroverted |
| 10 | Rectus femoris tightness | Ely’s test | Qualitative | - | - | Normal |
| 11 | Hip Abductorstrength | Single leg Squat | Qualitative | + | + | Hip abductorweakness |
| Special Tests | ||||||
| 1 | Radicular lowback pain | Straight legraise (SLR) | Qualitative | - | - | Normal |
| 2 | Radicular low back pain / Sacroiliacjoint pain | Flexion abduction external rotation(FABER) | Qualitative | - | - | Normal |
| 3 | Radicular lowback pain / Sacroiliac joint pain | Flexionabduction external rotation (FADIR) | Qualitative | - | - | Normal |
| 4 | Sacroiliac joint pain | SI compression | Qualitative | + | + | Normal |
| 5 | Anterior pelvictilt | Sit to Supinelengthening | Qualitative | - | + | Right hemipelvisanterior tilt |
| 6 | Anterior pelvic tilt | Gillet’s test | Qualitative | - | + | Right hemipelvis anterior tilt |
| Balance test | ||||||
| 1 | Balance | Single leg balance Open-eye | Qualitative | - | - | Normal |
| 2 | Balance | Single legbalance Closed-eye | Qualitative | - | - | Normal |
| Static StandingAlignment Tests | ||||||
| Spinal Alignment | Landmark Distance Measurements | |||||
| 1 | Coronal Scoliosis / Adams test |
4.6° | Distance (centimeters) | Left | Right | |
| 2 | Sagital | No kyphosis or Lordosis | ASIS to Midline | 10.5 | 10.5 | |
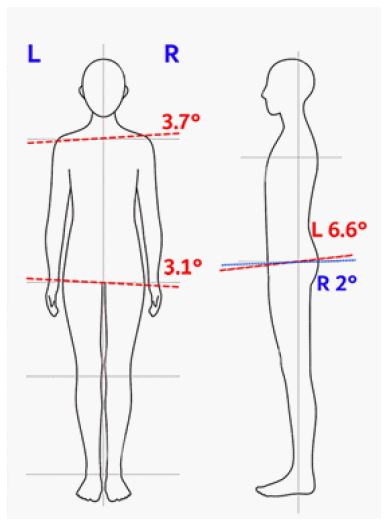
| Pelvic Alignment (Figure 2) | ASIS to Pubis | 14 | 14 | |||
| 1 | Sagittal Tilt | Rt Ant = 6.6° 1 Lt Ant = 2 ° 2 |
PSIS to Midline | 5 | 5.7 | |
| 2 | Coronal Tilt | 3.1° | Lower limbs Lengths | |||
| 3 | Axial Tilt | Neg | Left | Right | ||
| 4 | Hemipelvis Inflare /Outflare | Right HemipelvisInflare | Supine True lengths | 94 | 94 | |
| 5 | Hemipelvis Upslip | Left Hemipelvis Upslip | Sitted True lengths | 89 | 86.5 | |
| Knee Alignment | Standing True lengths | 93 | 93 | |||
| 1 | Coronal plane | No Knee varus or valgus | Apparent lengths | 105 | 105 | |
Laboratory tests: CBC, ESR, HLA-B27, Anti ds-DNA, 1,25(OH) vitamin D, 25(OH) vitamin D, and other tests were within the normal range.
Imaging: A pelvic AP X-ray is shown in figure 1. Left hemi-pelvis upslip is observed. In pelvic bone and sacroiliac MRI, no abnormality was noted in the sacrum, pelvis bones, sacroiliac joints, hip joints, femoral heads, necks, and sacrococcygeal joints. No abnormal signal intensities were visible in soft tissue and muscular structures. Pelvic malalignments measured with digital inclinometer and represented in figure 2.
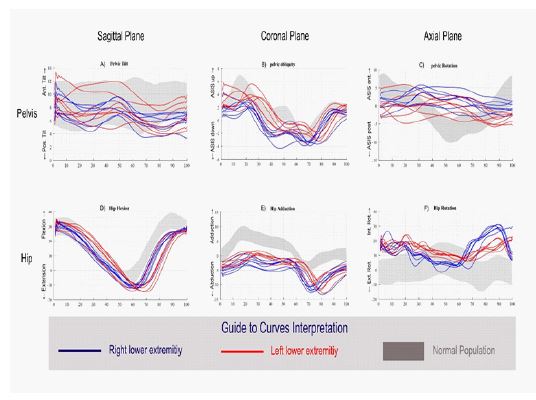
Clinical gait analysis: Due to prolonged tendinopathy with abnormal physical examination in pelvic alignment, gait analysis was ordered and performed with Vicon Capture System (Oxford Metrics Inc., Oxford, UK) and KISTLER force plates (KISTLER Instrumente AG, Winterthur, Switzerland). Three-plane kinematic changes of the pelvis and hip during gait cycles are reported in Figure 3. In this figure normal range for each parameter is shown in gray band, right lower extremity in blue, and left lower extremity in red for each detected gait cycle. There is a deviation in the pelvic and hip rotation kinematic charts that could be associated with long-standing hamstring tendinopathy.

Treatment: Due to coccydynia and sacroiliac joint inflammation and dysfunction, corticosteroid injection was performed under the C-arm guidance. The stabilizing pelvic belt was prescribed for 2 weeks followed by 5 sessions of muscle energy techniques and pelvic mobilization in the clinic, and self-mobilization at home for pelvic malalignment [1].
Discussion
A significant portion of the general population has misaligned pelvises [3]. Most cases of malalignment may not be associated with clinical signs and symptoms. However, in long-standing or refractory cases of hip, knee, or ankle disorders, addressing these malalignments may affect the rehabilitation process, dramatically. In our case, three types of pelvic mal-alignments were found, i.e. right hemipelvis inflare and anterior tilt, and left hemipelvis upslip.
One of the important findings in clinical gait analysis in this patient was the absence of normal pelvic rotation, which is one of the six determinants of efficient gait that contributed to vertical displacement of the center of the mass [4]. Compensatory excessive hip internal rotation is seen in this patient. Furthermore, left hemipelvis upslip and asymmetry may lead to increased tension at the biceps origin and by inhibiting synergistic muscles, increase hamstring functional demands [5].
Proximal hamstring tendinopathy secondary to malalignment syndrome was reported in the literature. As the ischial tuberosity is the common origin for the long hamstrings, excessive anterior pelvic tilt places the hamstring muscle at longer lengths. This may increase the risk of hamstring injuries, as was reported in our case [6].
Pelvic outflare and inflare may cause sacroiliac joint compression and gapping, respectively, and impair the normal biomechanics of the sacroiliac joint. In addition, upslips are generally accompanied by counternutation of the sacrum (anterior rotation of the innominate) which results in the tension of the long dorsal sacroiliac ligament. Furthermore, anterior rotation of the innominate may also counter-nutate the sacroiliac joint resulting in sacral rotation/torsion to the opposite side and pelvic rotation to the ipsilateral side [7]. This can result in compression of the SIJ on the opposite side and hence localized pain there [8,9]. Altogether, these abnormalities may result in SI joint and coccygeal pain and dysfunction.
Recognition of malalignment and the resulting detrimental effects should be part of the routine examination carried out by those caring for athletes to avoid misdiagnosis, mistreatment, delayed recovery, and possibly failure of the athlete to realize his or her full potential. Interventions such as joint mobilization and muscle energy techniques may help to alleviate pain due to biomechanical adjustments.
Clinical Bottom Line: In patients, especially athletes, who have long-standing pain non-responsive to usual treatments, detailed biomechanical analysis and appropriate biomechanical interventions are recommended, as they may be effective in the treatment process.
References
- Schamberger W. Malalignment syndrome in runners. Phys Med Rehabil Clin N Am. 2016; 27(1): 237-317.
- Jeon CK, Han SY, Yoo KT. The effects of manual therapy on lower extremity alignment in pelvic malalignment. J Int Acad Phys Ther Res. 2018; 9(3): 1543-48.
- Schamberger W. The malalignment syndrome: Diagnosing and treating a common cause of acute and chronic pelvic, limb, and back pain. Edinburgh (United Kingdom): Churchill Livingstone. 2013.
- Inman VT, Eberhart HD. The major determinants in normal and pathological gait. JBJS 1953; 35(3): 543-58.
- Panayi S. The need for lumbar–pelvic assessment in the resolution of chronic hamstring strain. J Bodyw Mov Ther. 2010;14(3): 294-8.
- Fredericson M, Moore W, Guillet M, Beaulieu C. High hamstring tendinopathy in runners: meeting the challenges of diagnosis, treatment, and rehabilitation. Phys Sportsmed. 2005; 33(5): 32-43.
- Opar DA, Williams MD, Shield AJ. Hamstring strain injuries; Factors that lead to injury and re-injury. Sports Med 2012; 42(3): 209-26.
- Herzog W, Conway PJ. Gait analysis of sacroiliac joint patients. J Manipulative Physiol Ther. 1994; 17: 124-127.
- Falowski S, Sayed D, Pope J, Patterson D, Fishman M, Gupta M, et al. A review and algorithm in the diagnosis and treatment of sacroiliac joint pain. J Pain Res. 2020; 13: 3337-48.