
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Cataract and Fahr syndrome: A case report
Amine K*; Hassina S; Tebbay N; Robbana L; Akannour Y; Serghini L; Abdellah E
University Mohammed V Rabat, Morocco.
*Corresponding Author : Krichene Amine
University Mohammed V Rabat, Morocco.
Email: drkrichene.m.amine@gmail.com
Received : Jan 09, 2024
Accepted : Apr 03, 2024
Published : Apr 10, 2024
Archived : www.jcimcr.org
Copyright : © Amine K (2024).
Abstract
Introduction: Fahr syndrome is a rare neurological disorder associated with abnormal calcium deposits in the brain. Cataract is a rare but potentially disabling complication of Fahr syndrome.
Case report: We report a case of bilateral posterior subcapsular cataract in a patient with Fahr syndrome secondary to primary hyperparathyroidism. The patient underwent phacoemulsification with implantation of an artificial lens, which improved his visual acuity and quality of life.
Discussion: Management of this association requires a multidisciplinary approach involving ophthalmologists, neurologists, endocrinologists and biologists. Further studies are needed to better understand the mechanisms, frequency, risk factors, screening, diagnosis and treatment of cataract in patients with Fahr syndrome.
Conclusion: Cataract is a rare complication of Fahr’s syndrome, requiring multidisciplinary management and further study. Phacoemulsification improves vision and quality of life in patients with this association.
Citation: Amine K, Hassina S, Tebbay N, Robbana L, Akannour Y, et al. Cataract and Fahr syndrome: A case report. J Clin Images Med Case Rep. 2024; 5(4): 2975.
Introduction
Fahr syndrome is a rare dominantly inherited neurological disorder characterized by abnormal bilateral intracerebral calcium deposits in regions that control movement, notably the basal ganglia and cerebral cortex.
We report a case of bilateral cataract in the context of Fahr’s syndrome, and highlight the importance of a phosphocalcic and metabolic work-up in the setting of cataract.
Case report
This was a 45-year-old patient with a 1-year history of neurological and memory disorders and an 18-month history of decreased visual acuity. A cataract was diagnosed and optically corrected without surgery.
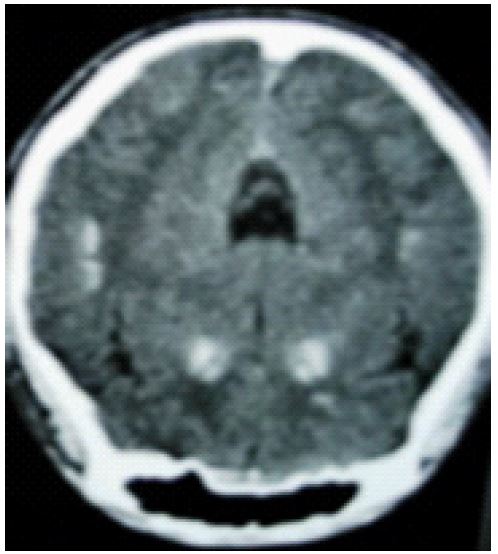
1 month prior to the ophthalmology consultation, the patient presented with worsening neurological disorders, with the onset of an extrapyramidal syndrome. The diagnosis of Fahr’s syndrome was evoked, and a cerebral Computed Tomography (CT) scan was performed, revealing calcifications in the caudate, lenticular, and subthalamic nuclei.
Biological tests revealed severe hypocalcemia with Ca++=65.3 mg/l and hyperphosphatemia at 59.4 mg/l. PTH was 4.2 pg/mL and 25 OH vitamin D=7 ug/l.
Given this clinical and paraclinical picture, the diagnosis of Fahr’s syndrome secondary to primary hyperparathyroidism was confirmed, and replacement therapy was initiated.
As the patient’s visual acuity worsened, he was referred to ophthalmology consultations for further management.
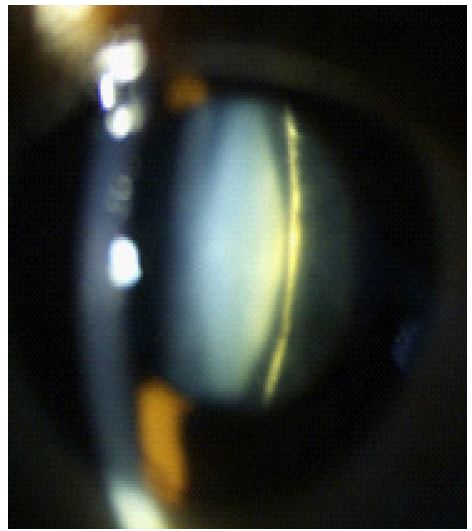
The ophthalmological examination revealed a decrease in bilateral visual acuity, quantified by finger count at 3 metres on the right and 1/10th on the left, and a dense bilateral posterior subcapsular cataract with a normal bilateral fundus. The rest of the examination was unremarkable.
The patient underwent phacoemulsification of the right eye and then the left eye two months apart.
Discussion
Cataracts are opacities of the crystalline lens that progressively reduce visual acuity. It is caused by a number of etiologies, such as age, trauma, systemic disease, medication, infection, or genetic factors. Disorders of calcium metabolism, such as primary hyperparathyroidism and Fahr’s syndrome, are among the systemic diseases associated with cataracts [1].
Fahr syndrome is a rare disease, with a probability of occurrence of around 0.5 per 100,000 people. A familial form is caused by mutations in the SLC20A2 gene, which codes for a phosphate transporter, and a sporadic form can be secondary to a variety of causes, such as primary hyperparathyroidism, hypoparathyroidism, pseudohyperparathyroidism, diabetes insipidus, Wilson’s disease, Huntington’s disease, multiple sclerosis, infections, trauma, or intoxication [1,2].
A rare ophthalmological complication of Fahr’s syndrome is cataract. Posterior subcapsular cataracts can be bilateral or unilateral. A review of the literature examined 230 cases of Fahr syndrome and found that 15% of patients had cataracts and that they were more common in patients with hypoparathyroidism than in those with hyperparathyroidism [6].
Although the precise mechanism of cataract formation is unknown, it may involve altered calcium and phosphate metabolism in the lens, leading to the accumulation of these minerals and lens opacification [1,2]. Chronic calcipenia is the likely mechanism behind cataracts, the severity of which is related to the age and degree of hypocalcemia and hyperphosphatemia [3].
A cerebral CT scan, revealing diffuse calcifications in the areas controlling movement, confirmed the diagnosis of Fahr’s syndrome. Phosphocalcemia and PTH, showing hypercalcemia and hypophosphatemia with elevated PTH, confirm the diagnosis of primary hyperparathyroidism.
Cataract treatment involves phacoemulsification and artificial lens implantation. The severity of brain damage and response to treatment determine the prognosis of Fahr’s syndrome. However, cataract surgery has a good prognosis, with improvements in vision and quality of life for patients [4]. A case of posterior subcapsular cataract in a patient with Fahr syndrome was reported in a study that showed that cataract surgery can improve visual acuity from 1/10th to 8/10th [5].
Cataract associated with Fahr’s syndrome is a rare but potentially disabling complication requiring multidisciplinary management. Many questions remain to be answered concerning this association, such as frequency, risk factors, molecular mechanisms, methods of screening, diagnosis, and treatment, as well as the long-term consequences of cataract surgery in patients with Fahr syndrome.
These questions are crucial to improving understanding, prevention and management of this complex disease. Epidemiological, biological, clinical and prospective studies are needed to find answers to these problems and open up new prospects for improving the quality of life and neurological prognosis of patients with Fahr’s syndrome.
Conclusion
Cataracts are a rare but potentially disabling complication of Fahr syndrome, an inherited neurological disorder caused by abnormal calcium deposits in the cerebral areas that control movement. We report a case of bilateral posterior subcapsular cataract in a patient with Fahr syndrome secondary to primary hyperparathyroidism. The management of this association requires a multidisciplinary approach involving ophthalmologists, neurologists, endocrinologists, and biologists. Further studies are needed to better understand the pathophysiology, frequency, screening, risk factors, diagnosis, and treatment of cataracts in patients with Fahr’s syndrome.
References
- Dr Y. Benabdelfedil, Dr S. Derrou, Pr F. El Guendouz, Pr H. Ouleghzal, Pr S. Safi Cataracte révélant un syndrome de Fahr: à propos d’un cas et revue de littérature. Doi : 10.1016/j.ando.2020.07.663.
- Feten Fekih-Romdhane, Abir Tounsi, Sinda Ben Fadhel, Rym Ridha Maladie de Fahr révélée par des troubles psychiatriques, L’information psychiatrique. 2020; 4(96): 279-283.
- Stein R, Godel V. Hypocalcemic cataract. J Pediatr Ophthalmol Strabismus. 1980; 17(3): 159-61.
- El Matri L, Chebbi A, Kort F, et al. Cataracte et syndrome de Fahr: à propos d’un cas. Journal Français d’Ophtalmologie. 2009; 32(2): 139-142. doi: 10.1016/S0181-5512(09)70035-0.
- Koc F, Kargi S, Biglan AW, et al. Cataract surgery in a patient with bilateral striopallidodentate calcinosis (Fahr syndrome). J Cataract Refract Surg. 2006; 32(9): 1471-1473. doi: 10.1016/j.jcrs.2006.04.021.
- Saleem S, Aslam HM, Anwar M, et al. Fahr’s syndrome: literature review of current evidence. Orphanet J Rare Dis. 2013; 8: 156. doi:10.1186/1750-1172-8-156 [8] Harding JJ. Cataract: Biochemistry, Epidemiology and Pharmacology. Chapman and Hall; 1991.