
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Commentary - Open Access, Volume 5
Prospective study on the efficacy of RoseK2 contact lenses in the treatment of keratoconus: 59 patients
Amine K*; Tebbay S; Hassina S; Robbana L; Akannour Y; Serghini L; Abdellah E
University Mohammed V Rabat, Morocco.
*Corresponding Author : Krichene Amine
University Mohammed V Rabat, Morocco.
Email: drkrichene.m.amine@gmail.com
Received : Jan 09, 2024
Accepted : Apr 03, 2024
Published : Apr 10, 2024
Archived : www.jcimcr.org
Copyright : © Amine K (2024).
Abstract
Keratoconus is a progressive corneal disease affecting vision. This 12-month prospective study in Rabat evaluated the efficacy of RoseK2 rigid Gas Permeable Contact Lenses (RPGCLs) in 59 patients (113 eyes) with keratoconus. Patients were monitored by refraction, keratometry and corneal topography. RPGCLs showed a significant improvement in Best Corrected Visual Acuity (BCVA) in 86% of eyes fitted, mainly in those with myopic astigmatism. Despite good overall tolerability, minor complications such as limbal hyperemia were noted in some patients. Keratoconus geometry was closely correlated with disease progression. This study confirms that RoseK2 RPGCLs are an effective therapeutic option for keratoconus patients, but underlines the need for ongoing monitoring to detect and treat complications early.
Keywords: Cornea; Lenses; Keratoconus.
Citation: Amine K, Tebbay S, Hassina S, Robbana L, Akannour Y, et al. Prospective study on the efficacy of RoseK2 contact lenses in the treatment of keratoconus: 59 patients. J Clin Images Med Case Rep. 2024; 5(4): 2976.
Introduction
Keratoconus is a degenerative, chronically progressive, non-inflammatory disease characterized by thinning and ectasia of the cornea, which affects patients’ quality of life and vision. Rigid gas Permeable Contact Lenses (RPGCLs), including the RoseK2 type, have been presented as a promising treatment option to correct the impaired vision caused by this disease. The aim of this prospective study on a cohort of keratoconus patients is to assess the efficacy, tolerability, and clinical implications of RoseK2 type RPGCLs in the visual correction and follow-up of this ocular pathology.
Materials and methods
We conducted a prospective study over a 12-month period in the ophthalmology department B of the Hospital of Specialties in Rabat, in which we included 59 patients (113 eyes) with uni or bilateral keratoconus, adapted to RPGCL (RoseK2), and followed on an outpatient basis. The follow-up of our patients was based on refraction, keratometry, and corneal topography (Pentacam).
Results
We adapted corneal RPGCL (RoseK2 type) on 113 eyes of 59 patients with keratoconus. The sex ratio was 1.03 and the mean age was 26.66.7% of patients were in full socio-professional activity, 42.1% of whom were young students (Figure 1).
Associated signs were allergic conjunctivitis in 20 patients (35.5%), eye rubbing in 18 patients (31.6%) and general atopy in 3 patients (5.3%).
A family history of keratoconus was found in 7% of cases, particularly among siblings.
65% of patients wore glasses, 26.3% had no correction and 8.7% wore contact lenses. Bilaterality in our series was noted in 94.7% of cases, and the majority of patients (53.5%) had stage 3 eyes (Table 1). In adapted eyes, refraction, if performed, showed myopic astigmatism in 61.4% versus 21.6% astigmatism alone (Table 2).
Topography was performed on all our patients, assessing maximum keratometry, pachymetry, elevation, refractive maps, and cone characteristics for each stage with a Kmax of 61.90 (Table 3).
Table 1: Percentage and number of eyes by keratoconus stage.
| Stage 1 | 4 eyes | 4,5% | 9 | 10,2% | 14,7% |
| Stage 2 | 15 eyes | 17% | 7 | 8% | 25% |
| Stage 3 | 26 eyes | 23,3% | 23 | 26,2% | 53,5% |
| Stage 4 | 0 eyes | 0% | 6 | 6,8% | 6,8% |
Table 2: Refraction data on adapted eyes.
| Refraction | Number of eyes | Percentage |
|---|---|---|
| Only astigmatism | 14 | 21,6% |
| Astigmatism + myopia | 73 | 61,4% |
| Does not take | 24 | 17% |
Table 3: Average keratometry of patients in our series.
| K1 | 48,91 | 41,9 | 57,8 |
| K2 | 53,3 | 44,8 | 61,9 |
| K m | 51,57 | 44 | 63 |
| K max | 61,90 | 48,6 | 80 |
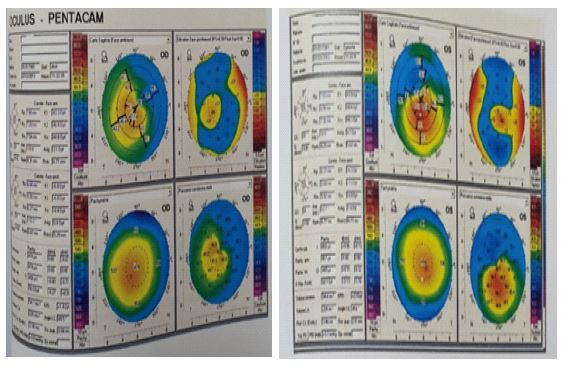
Table 4: Average pachymetry values measured.
| average | minimal | Maximal | |
|---|---|---|---|
| Central pachymetry (um) | 445,48 | 350 | 534 |
| Minimal pachymetry (um) | 415 | 298 | 435 |
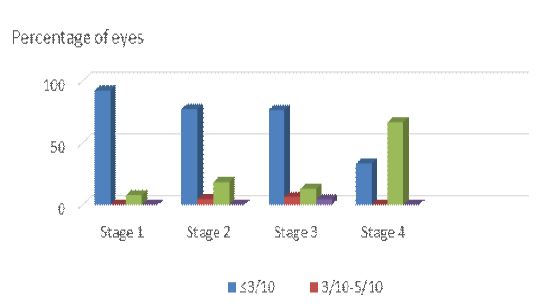
Table 5: Assessment of tolerability in adapted patients.
| Tolerance | Actual | Percentage |
|---|---|---|
| Bad | 5 | 8,8% |
| Good | 12 | 21,1% |
| Excellent | 40 | 70,1% |
| Total | 57 | 100% |
Table 6: Complications.
| Complications | Actual | Percentage |
|---|---|---|
| Limbic hyperaemia | 10 | 16,9% |
| 3h – 9h syndrom | 5 | 8,4% |
| giganto-papillary conjunctivitis | 1 | 1,69% |
| Lens loss or breakage | 1 | 1,69% |
Mean central pachymetry was 445.5 and 415 in the periphery (Table 4).
After adaptation of the RPGCLs, 86% of the eyes fitted were able to increase their best corrected visual acuity (BCVA) to a value greater than or equal to 7/10ths (Figure 3). As the disease progresses, BCVA decreases.
Average lens wearing time was 12 hours, with 91.2% of wearers enjoying satisfactory comfort (Table 5). The main complication was limbal hyperemia in 17.5% of cases (Table 6).
Discussion
RoseK2 corneal RPGCLs are effective and well tolerated for fitting patients with keratoconus, with significant improvement in BCVA and satisfactory comfort, as demonstrated in our study. These results are in line with those of other studies that have used similar multicurve lenses to treat keratoconus [1].
RPGCLs are considered the treatment of choice for moderate and severe forms of keratoconus, as long as the cornea remains transparent [2]. Thanks to the gas permeability of the materials used, they can correct irregular astigmatism and improve visual quality while respecting corneal physiology [3]. The shape and stage of the keratoconus, as well as the patient’s response, determine the lens geometry. Multicurved lenses, such as RoseK2 lenses, offer the advantage of adapting to the variability of keratoconus corneas by providing central support, smooth transition, and peripheral alignment [4].
We adapted 113 eyes from 59 patients in our series, whose mean age was 26 years, corresponding to the age group most affected by keratoconus. The sex ratio was close to 1, indicating that there was no sexual predominance in the occurrence of the disease, contrary to some studies that have shown the disease to be more common in men [5]. Bilaterality was 94.7% in our series, in line with the literature. In our setting, the majority of patients had stage 3 keratoconus, 53.5%, reflecting the delay in diagnosis and therapy of this disease. Refraction revealed myopic astigmatism in 61.4% of adapted eyes, compared with 21.6% with astigmatism alone, in accordance with Krumeich’s classification [6]. All our patients received topography by assessing maximum keratometry, pachymetry, elevation, refractive map, and cone characteristics for each stage. We found that as the keratoconus stage progressed, maximum keratometry increased from 48.5 D at stage 1 to 62.5 D at stage 4, which is comparable to the results of Gokhale [7]. Minimum pachymetry also decreased with the keratoconus stage. From 486 μm at stage 1 to stage 4, it decreased to 375 μm at stage 4, in line with the values reported by Hashemi [8]. The cone was most often central (52.2%) or inferocentral (36.3%), depending on the elevation map, which is in agreement with Belin’s observations [9]. The irregular astigmatism and myopia induced by keratoconus were confirmed by refractive mapping.
We were able to increase the BCVA in 86% of RPGCL-equipped eyes to a value greater than or equal to 7%, which is comparable to the success rates reported in other studies [10,11]. We also observed that the BCVA decreased as the disease progressed, which is logical given the progressive corneal deformation and thinning. Average lens wear time was 12 hours, with 91.2% satisfactory comfort, suggesting that our patients have a good tolerance to RPGCLs. In 17.5% of cases, limbal hyperemia was the main complication, which is lower than the rates reported by other authors [12,13]. Lens maladjustment, corneal hypoxia, allergic reactions, or poor lens hygiene may be the cause of this complication. By modifying lens geometry, using more permeable materials, prescribing lubricating or anti-allergic eye drops, or educating the patient on lens care rules, it can be prevented or treated.
Our study is interesting in that it is the first to evaluate the efficacy and tolerability of RoseK2 type RPGCLs in Keratoconus in Morocco. It demonstrates that these lenses are an effective treatment option for patients with moderate to severe keratoconus who cannot benefit from satisfactory correction with spectacles or soft lenses. It also highlights the importance of regular monitoring of RPGCL patients in order to detect and treat potential complications and of readjusting lenses in the event of keratoconus progression.
Conclusion
This prospective study, conducted over a 12-month period in the Ophthalmology B department of the Rabat Specialty HosHospital, demonstrated the significant efficacy of RoseK2 contact lenses in the treatment of keratoconus. Fitting these lenses resulted in a significant improvement in best corrected visual acuity in a majority of patients. The results also confirm satisfactory patient tolerance for RPGCLs, although some minor complications were observed, mainly limbal hyperemia.
This study reinforces the importance of RPGCLs, in particular RoseK2 lenses, as an effective treatment option for keratoconus patients, offering a significant improvement in quality of vision. It also highlights the importance of regular monitoring to detect complications early and adjust lenses if the disease progresses. These results highlight the beneficial impact of RPGCLs in the management of keratoconus and underline the need for an individualized approach for each patient, taking into account disease progression and clinical response to contact lenses.
References
- Baklouti A, Trigui A, Barkia I, Khabou A, Kharrat W, Fetoui F, Rebhi F, Kamoun B, Benzina Z, Feki J. L’adaptation des lentilles rigides perméables aux gaz dans le kératocône. Journal Français d’Ophtalmologie. 2009; 32(5): 507-508.
- Risser G, Muselier-Mathieu A. Avancées en adaptation lentilles pour les kératocônes. Réalités Ophtalmologiques. 2023; 287: 14-18.
- Alió JL, Shabayek MH, Artola A. Intracorneal ring segments for keratoconus correction: long-term follow-up. Journal of Cataract & Refractive Surgery. 2006; 32(6): 978-985.
- Efron N, Morgan PB, Hill EA, Raynor MK, Tullo AB. The Manchester Keratoconus Study: Contact Lens Fitting and Aftercare. Eye & Contact Lens. 2011; 37(1): 2-7.
- Gokhale NS. Epidemiology of keratoconus. Indian Journal of Ophthalmology. 2013; 61(8): 382-383.
- Krumeich JH, Daniel J, Knülle A. Live-epikeratophakia for keratoconus. Journal of Cataract & Refractive Surgery. 1998; 24(4): 456-463.
- Gokhale NS, Sawhney S, Vaidya S, Vaidya S. A retrospective study of the progression of keratoconus in Asian eyes using Scheimpflug imaging. Indian Journal of Ophthalmology. 2018; 66(6): 807-811.
- Hashemi H, Heydarian S, Hooshmand E, Saatchi M, Yekta A, Aghamirsalim M, Khabazkhoob M. The Distribution of Keratoconus and its Association with Pachymetry and Corneal Power Maps in a Population-Based Study. Cornea. 2019; 38(8): 1012-1017.
- Belin MW, Khachikian SS. An introduction to understanding elevation-based topography: how elevation data are displayed – a review. Clinical & Experimental Ophthalmology. 2009; 37(1): 14-29.
- Romero-Jiménez M, Santodomingo-Rubido J, Wolffsohn JS. Keratoconus: a review. Contact Lens and Anterior Eye. 2010; 33(4): 157-166.
- Ozkurt Y, Atakan M, Gencaga T, Akkaya S. Contact lens visual rehabilitation in keratoconus and corneal keratoplasty. Journal of Ophthalmology. 2012; 2012: 832070.
- Ozkurt YB, Sengor T, Kurna S, Aki S, Ozkan S. Evaluation of the corneal endothelial cell density and central corneal thickness in keratoconus. Clinical & Experimental Optometry. 2012.