
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 5
Neurological manifestations of ponto-medullary glioependymal cyst in a middle-aged female with hypothyroidism: A case report
Muhammad Maskoob Talib1; Areeba Tariq2*; Manzar Hussain3
1Resident, Neurosurgery, Liaquat National Hospital, Karachi, Pakistan.
2Registrar, Neurosurgery, Liaquat National Hospital, Karachi, Pakistan.
3Consultant, Neurosurgery, Liaquat National Hospital, Karachi, Pakistan.
*Corresponding Author : Areeba Tariq
Resident Neurosurgery, Liaquat National Hospital, Karachi, Pakistan.
Email: dr.areeba.tariq@gmail.com
Received : Mar 15, 2024
Accepted : Apr 04, 2024
Published : Apr 11, 2024
Archived : www.jcimcr.org
Copyright : © Tariq A (2024).
Citation: Talib MM, Tariq A, Hussain M. Neurological manifestations of ponto-medullary glioependymal cyst in a middle-aged female with hypothyroidism: A case report. J Clin Images Med Case Rep. 2024; 5(4): 2980.
Introduction
ChordomasArachnoid cysts, also referred to as leptomeningeal cysts, are congenital lesions originating during developmental stages through the division of the arachnoid membrane, making them technically intra-arachnoid cysts. These cysts typically contain fluid that closely resembles Cerebrospinal Fluid (CSF). While arachnoid cysts are commonly benign and asymptomatic, they are relatively prevalent. Although the majority are sporadic, an increased incidence is observed in mucopolysaccharidoses, akin to perivascular spaces. Most arachnoid cysts are small in size, and about 5% of individuals may experience symptoms, often attributed to gradual enlargement leading to mass effect. There is a notable male predominance, with a ratio of approximately 3:1. Diagnosis is typically accomplished through the gold standard imaging techniques of Computed Tomography (CT) and Magnetic Resonance Imaging (MRI).
Case details
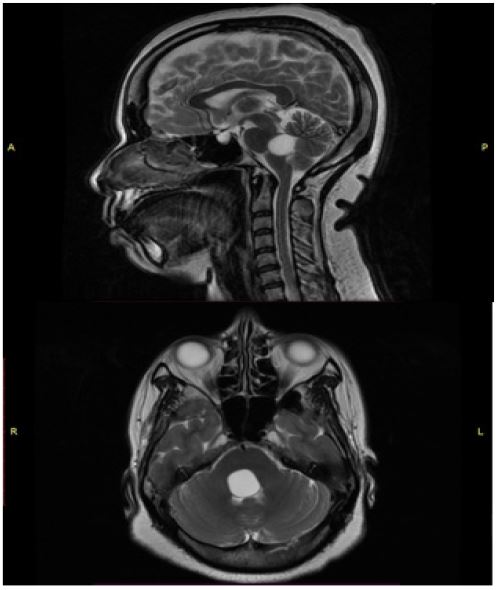
A 40-year-old female with a known history of hypothyroidism presented at the Outpatient Department, reporting gait imbalance, vertigo, facial asymmetry, and right-sided upper limb weakness persisting for one year. On examination, her Glasgow Coma Scale (GCS) was 15/15, but she exhibited an ataxic gait with positive cerebellar signs and had 4/5 power in the right upper limb. MRI brain revealed a well-defined rounded cystic lesion at the ponto-medullary junction on the right side, causing compression of the fourth ventricle. The lesion was indicative of a likely benign glioependymal cyst measuring 1.7 x 1.7 x 1.6 cm.
Discussion
The inception of the understanding of intracranial arachnoid cysts dates back to 1831 when the esteemed English surgeon Richard Bright first reported them at Guy’s Hospital, labeling them as “serious cysts in the arachnoid [1]. “In 1924, Gilbert Horrax introduced the term “generalized cisternal arachnoiditis” after a series of patients underwent excision of posterior fossa arachnoid cysts by Horrax and Harvey Cushing [2]. Subsequently, in 1932, Winchell M. Craig reported on the removal of posterior fossa arachnoid cysts referred to as “chronic cystic arachnoiditis,” believed to have developed post-meningoencephalitis [3].
Congenital arachnoid cysts are characterized by hyperplastic arachnoid cells in the cyst wall, the absence of traversing trabecular processes within the cyst (as seen in normal arachnoid), a split arachnoid membrane, and thick collagen in the cyst wall. While the exact cause remains unknown, a widely acknowledged theory suggests that the arachnoid membrane splits during embryonic neural tube folding, forming subarachnoid cisterns that may later accumulate Cerebrospinal Fluid (CSF) [4].
Despite common locations such as the quadrigeminal plate, retrocerebellar area, cerebellopontine angle, fourth ventricle, and clivus, only 5 to 10% of these cysts occur in the posterior cerebral fossa [5]. Arachnoid cysts in the fourth ventricle are exceptionally rare [6], with only 16 reported cases in the literature. When symptomatic, posterior fossa arachnoid cysts can exert a mass effect on ventral CSF flow, leading to headaches, ataxia, urine incontinence, and disturbed gait. Symptoms resembling Chiari malformation may also manifest, including positional headache, neck pain, and occipital headache [7]. Unlike suprasellar cysts, which may directly compress the optic system, vision-related complaints result from papilledema and hydrocephalusn [8].
Posterior fossa arachnoid cysts are categorized into four subtypes: 1a (midline and in communication with the fourth ventricle), 1b (retrocerebellar midline and not in communication with the fourth ventricle), 2a (off midline within the cerebellopontine angle, overlapping with quadrigeminal cistern cysts), and 2b (off-midline retrocerebellar or intracerebellar) [9].
A study in India demonstrated the feasibility of completely removing the cyst wall, including the portion adhering to the cerebellar surface, in midline PFAC 1b and retrocerebellar PFAC 2b by carefully peeling the cyst wall [10]. As a safe alternative to open microsurgical excision, the same study recommended cysto-peritoneal shunt for treating PFAC 1a cysts situated deep intra-fourth ventricle or retroclival cysts. In the case of retroclival or intra-fourth ventricular PFAC, where microsurgical treatment is pursued, either elevating the vermis or making a midline vermis-splitting incision is required, both of which pose a postoperative risk of persistent vermian dysfunction. For PFAC 1a cysts, cysto-peritoneal shunt is the preferred method. In treating retroclival or intra-fourth ventricular PFAC with cysto-peritoneal shunting, incorrect positioning of the proximal catheter inside the brainstem or cerebellum may lead to acute shunt dysfunction or neurological impairments [11]. Therefore, the recommended treatment for intra-fourth ventricular arachnoid cysts is cysto-peritoneal shunt or endoscopic cyst fenestration.
References
- Bright R. Reports of medical cases: Selected with a view of illustrating the symptoms and cure of diseases by a reference to morbid anatomy. Vol 2: Richard Taylor, Red Lion Court, Fleet Street. 1831.
- Horrax G. Generalized cisternal arachnoiditis simulating cerebellar tumor: its surgical treatment and end-results. Archives of Surgery. 1924; 9: 95-112.
- Craig WM. Chronic cystic arachnoiditis. The American Journal of Surgery. 1932; 17: 384-8.
- Starkman S, Brown T, Linell E. Cerebral arachnoid cysts. Journal of Neuropathology & Experimental Neurology. 1958; 17: 484-500.
- Samii M, Carvalho GA, Schuhmann MU, Matthies C. Arachnoid cysts of the posterior fossa. Surgical neurology. 1999; 51: 376-82.
- Hiroshima S, Saga T, Saito M, et al. Treatment of Fourth Ventricle Arachnoid Cyst via Anterior Hone of Lateral Ventricle Using Flexible Endoscope. World Neurosurgery. 2019; 124: 224-7.
- Bahuleyan B, Rao A, Chacko AG, Daniel RT. Supracerebellar arachnoid cyst–A rare cause of acquired Chiari I malformation. Journal of Clinical Neuroscience. 2007; 14: 895-8.
- Ahmed AK, Cohen AR. Intracranial arachnoid cysts. Child’s Nervous System. 2023: 1-8.
- Barkovich AJ, Kjos BO, Norman D, Edwards MS. Revised classification of posterior fossa cysts and cystlike malformations based on the results of multiplanar MR imaging. American journal of neuroradiology. 1989; 10: 977-88.
- Gazioglu N, Kafadar AM, Tanriover N, Abuzayed B, Biceroglu H, Ciplak N. Endoscopic management of posterior fossa arachnoid cyst in an adult: case report and technical note. Turkish Neurosurgery. 2010; 20.
- Srinivasan U, Lawrence R. Posterior fossa arachnoid cysts in adults: Surgical strategy: Case series. Asian journal of neurosurgery. 2015; 10: 47.