
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Spontaneous hemothorax revealing aortic dissection and intramural hematoma
Badra Bahri1,2*; Fares Hamdi1,2; Belgacem Ines1,2; Touj Hajer1,2; Sedghiani Ines1,2; Chammakhi Chiraz1,3; Youssef Zied El Hechmi1,2; Nebiha Borsali-Falfoul1,2
1University of Tunis El Manar, Faculty of Medicine of Tunis, 1006, Tunis, Tunisia.
2Emergency Department, Habib Thameur University Hospital, 1089, Tunis, Tunisia.
3Radiology Department, Habib Thameur University Hospital, 1089, Tunis, Tunisia.
*Corresponding Author : Badra Bahri
University of Tunis El Manar, Faculty of Medicine of Tunis, 1006, Tunis, Tunisia.
Tel: +21 626137531.
Email: bahribadra@gmail.com
Received : Mar 18, 2024
Accepted : Apr 05, 2024
Published : Apr 12, 2024
Archived : www.jcimcr.org
Copyright : © Bahri B (2024).
Keywords: Aortic dissection; Intramural hematoma; Emergency; Hemothorax.
Abreviations: AAS: Acute Aortic Syndrome; AD: Aortic Dissection, IMH: Intramural Hematoma; CRP: C-Reactive Protein; CT: Chest Computed Tomographic.
Citation: Bahari B, Hamdi F, Ines B, Hajer T, Ines S, et al. Spontaneous hemothorax revealing aortic dissection and intramural hematoma. J Clin Images Med Case Rep. 2024; 5(4): 2982.
Introduction
Acute Aortic Syndrome (AAS) is a group of life-threatening aortic diseases that includes Aortic Dissection (AD), Intramural Hematoma (IMH) and penetrating aortic ulcer. Intramural Hematoma (IMH) of the thoracic aorta is a rare, little-known but potentially lethal entity. It has several features in common with Aortic Dissection (AD). We report a clinical observation of a spontaneous hemothorax revealing aortic dissection and Intramural hematoma.
Case presentation
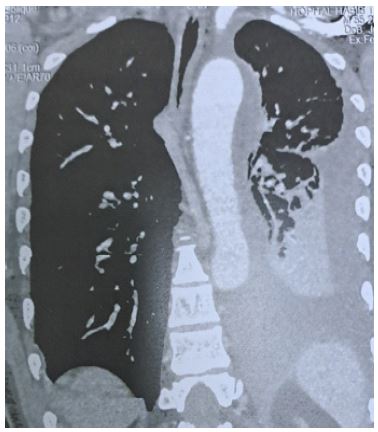
A 55 year smoking man with no medical history was admitted to our emergency department for chest pain and dyspnea evolving for one week. On examination, respiration rate was 22 breaths per minute, pulse rate was 104 beats per minute and blood pressure was 210/110 mmHg. Breath sound were decreased at the left lung, peripheral pulses were palpated. The electrocardiogram showed normal sinus rhythm. The chest radiography revealed an important left-sided pleural effusion (Figure 1). Laboratory test revealed normochrome anemia with an hemoglobin level of 9,5 gr/dl, arterial blood gases showed an hypoxemia of 52 mmHg. We found biological inflammatory syndrome with a C-Reactive Protein (CRP) level of 270 mg/l and hyperleukocytosis with a whiteblood cells count of 16590 el/mm3.
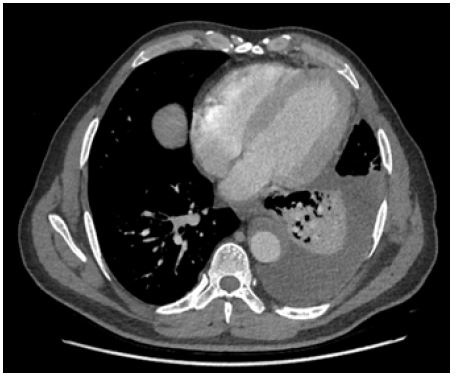
The chest Computed Tomographic (CT) scan confirmed the presence of a left-sided pleural effusion and showed a Stanford type B aortic dissection with intramural hematoma of the aorta associated with a penetrating atheromatous ulcer of the descending thoracic aorta complicated by a high abundance hemothorax (Figure 2) and a low abundance hemopericardium (Figure 3). Cardiac ultrasound at patient’s bedside showed left ventricle not dilated, left atrium was dilated at 20 cm², type I mitral profile, no significant mitro-aortic valve disease, straight non-dilated cavities and preserved right ventricular function with a thin strip of pericardial effusion. The patient received nicardipine by electric syringe pump in order to lower his blood pressure. Then he underwent chest drainage having removed two liters of hematic fluid. He was transferred to the cardiovascular surgery department on the second day, they opted for a conservative strategy and the patient was discharged under medical treatment.

Discussion
Intramural hematoma is a localized haemorrhage within the wall of the aorta in the absence of a defined intimal flap [1]. The hemothorax secondary to a rupture of a great chest vessel is uncommon. It is essentially aneurysm of the aorta, an aortic dissection or pulmonary arteriovenous malformations [2].
IMH is most commonly diagnosed in elder men aged between 60 and 80 years [3,4]. It occurs in an area where the aorta is weakened. This can occur as a consequence of a hypertension, an atherosclerosis, a Marfan syndrome, a Takayasu’s arteritis, a prior aortic surgery, an aortic aneurysm, a coarctation of the aorta, a bicuspid aortic valve, the pregnancy and a prior cardiac surgery [5]. Our patient was a 55 year smoking man with no history of hypertension and no other medical history.
Radiological investigations are the key for the diagnosis. Chest X rays may show mediastinal enlargement, left pleural effusion, as we observed in our patient and an indistinct aortic contour [6,7]. The chest CT scan with contrasts is the best tool for the diagnosis and the management of patients with suspected aortic acute syndrome [8].
IMH can be classified as Stanford type A involving the ascending aorta and Stanford type B involving the aortic arch or descending aorta [9]. IMH may progress into AD over time in 47% of cases but they may also regress spontaneously or remain static [10,11] such as the case of our case. In well-established tertiary care setups, emergency surgical measures may provide a better outcome than medical treatment for patients with an acute type A aortic IMH [12-14] while the aggressive management of hypertension showed good short-term outcomes in patients with Stanford type B IMH [12].
Conclusion
IMH is less frequent than AD and uncommon. The emergency physicians must be aware of the spontaneous hemothorax and the atypical presentations of this life threatening aortic disease to perform Imaging as soon as possible.
References
- Omar A, Ali MD, Nsidinanya Okike MD, Robert G, Hogan MD, and Richard C. Becker MD. Intramural Hematoma of theThoracic Aorta in a Woman With Neurofibromatosis. Ann Thorac Surg. 2002; 73: 95860.
- T Langin, PE Kelkel, D Villemot, “Left Hemotho- rax, a Complication of a Dissecting Aneurysm of the De- scending Thoracic Aorta, Revue Des Maladies Respiratoires 1994 :11: 74-76.
- IB, Alomari Hamirani YS, Madera G, Tabe C, Akhtar N, Raizada V. Aortic intramural hematoma and its complications. Circulation. 2014; 129(6): 711-6.
- Cappellini interventions. Early and follow-up CT imaging findings. Radiol Cardiothorac Imaging. 2021; 3(6): 210241..
- Kanaan T, Abdelrahman AS, Jaber J, Fahmi AM, Almasalmeh A, Alnakawa S, Kanaan T. Type A aortic dissection with intramural hematoma: A challenging diagnosis. Cureus. 2023; 15(1): 33300.
- S Bousnina, I Zendah, K Marniche, H Racil, S Kach- boura, ML Megdiche and A. Chabbou, “Left Hemotho- rax Caused by Aortic Dissection Rev Pneumol Clin. 2007; 63(2): 119-22.
- F Miller, HR Shah, RS Pritchard, EC Buck- ner, “CT Diagnosis of Right Hemothorax Secondary to Ruptured Thoracoabdominal Aneurysm: Case Report : Cardiovasc Intervent Radiol. 1989; 12(6): 326-8.
- F. Özkan, E. Akpına, T. Serter, A. Özyüksel and T. Hazı- rolan, Ruptured Type B Aortic Dissection Presenting with Right Hemothorax. Diagn Interv Radiol. 2008; 14(1): 6-8.
- Bossone E, LaBounty TM, Eagle KA. Acute aortic syndromes: Diagnosis and management, an update . Eur Heart J. 2018; 39: 739-749.
- Tsushima T, Al-Kindi S, Patel T, Kalra A. Atypical complications of aortic intramural hematoma: Paraplegia resulting from spinal cord infarction. Int J Cardiol Heart Vasc. 2019; 22: 154-5.
- Vilacosta I, Aragoncillo P, Cañadas V, San Román JA, Ferreirós J, Rodríguez E. Acute aortic syndrome. A new look at an old conundrum. Postgrad Med J. 2010; 86: 52-61.
- Hoey ET, Wai D, Ganeshan A, Watkin RW. Aortic intramural haematoma: pathogenesis, clinical features and imaging evaluation. Postgrad Med J. 2012 ; 88: 661-7.
- Vilacosta I, Castillo JA, Peral V, Batlle E, Rollán MJ, Sánchez-Harguindey L. Intramural aortic haematoma following intra-aortic balloon counterpulsation. Documentation by transoesophageal echocardiography. Eur Heart J. 1995; 16(12): 2015-6.
- Mohr-Kahaly S, Erbel R, Kearney P, Puth M, Meyer J. Aortic intramural hemorrhage visualized by transesophageal echocardiography: Findings and prognostic implications. J Am Coll Cardiol. 1994 ; 23: 658-64.