
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Recurrent midgut volvulus: A case report
Preeti Singh Prasad*; Timothy Jancelewicz; Preet K Sandhu
The University of Tennessee Health Science Center College of Medicine, India.
*Corresponding Author : Preeti Singh Prasad
The University of Tennessee Health Science Center College of Medicine, India.
Email: pprasad3@uthsc.edu
Received : Mar 18, 2024
Accepted : Apr 08, 2024
Published : Apr 15, 2024
Archived : www.jcimcr.org
Copyright : © Prasad PS (2024).
Abstract
We report the case of a 2-month-old who had recurrent midgut volvulus after undergoing the Ladd’s procedure on the first day of life for malrotation with midgut volvulus. Recurrent midgut volvulus after a Ladd’s procedure is a rare entity. The most common presentation is with bilious emesis. A high index of suspicion and awareness is necessary to allow for early recognition and intervention. If the diagnosis is delayed, a catastrophic outcome may occur.
Keywords: Midgut volvulus; Recurrence; Ladd’s procedure.
Citation: Prasad PS, Jancelewicz T, Sandhu PK. Recurrent midgut volvulus: A case report. J Clin Images Med Case Rep. 2024; 5(4): 2986.
Introduction
Midgut malrotation occurs in approximately 1 in 500 live births [1]. It can lead to a life-threatening emergency when complicated by midgut volvulus. The Ladd’s procedure is the operation of choice and is usually curative. On rare occasions, recurrent midgut volvulus can occur after surgical repair. The incidence of recurrent volvulus has been reported to range from 2% to between 5% and 7%. Its development is believed to be prevented by the formation of postsurgical adhesions that restrict the movement of bowel loops and thereby prevent a recurrence.
We report a case of a 2-month-old patient who was diagnosed with malrotation and midgut volvulus in the first week of life. The patient underwent a successful Ladd’s procedure. However, he returned after two months with recurrent midgut volvulus.
Case report
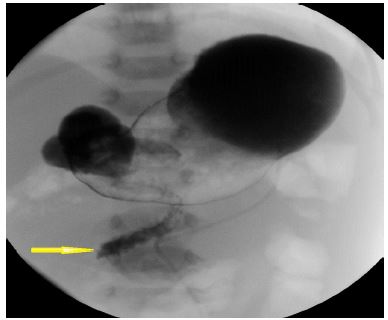
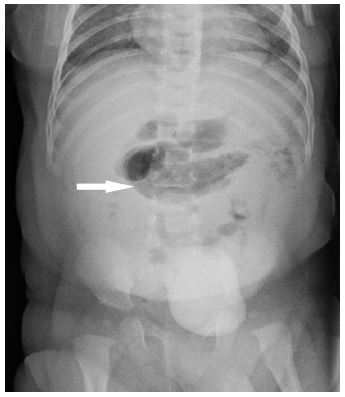
A 2-month-old male patient presented to the emergency room with new onset bilious emesis. The patient was born at full-term and had a history of intestinal malrotation and midgut volvulus that occurred at 27 hours of life and was treated with a standard open Ladd’s procedure. Abdominal radiograph at the time of first presentation (at 27 hours of age) showed a markedly gas-distended stomach (Figure 1). An upper Gastrointestinal (GI) imaging series performed at that time at an outside hospital revealed high-grade duodenal obstruction caused by malrotation and midgut volvulus with the classic ‘corkscrew appearance’ of midgut volvulus seen (Figure 2). The patient underwent an open Ladd’s procedure with appendectomy. He was started on enteral feeds on Postoperative Day (POD) 7 and was tolerating full feeds by POD 10. He was discharged on day 11 of life in good health.
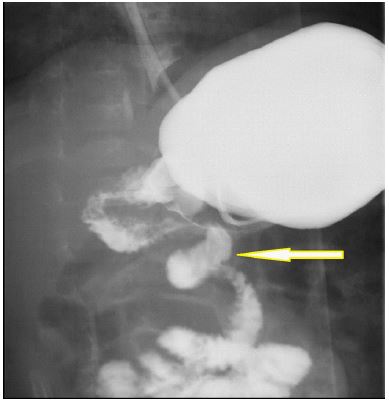
Two months after the surgery, the patient returned to the emergency room with new-onset bilious emesis. An abdominal radiograph was performed, which showed mildly distended tubular appearing bowel loops in the central upper abdomen concerning for proximal bowel obstruction (Figure 3). Concern for recurrent volvulus was raised, and an upper GI study was performed. The upper GI series revealed malrotation and recurrence of midgut volvulus with a “corkscrew” appearance of the proximal jejunum (Figure 4). The imaging appearance was similar to the initial study.
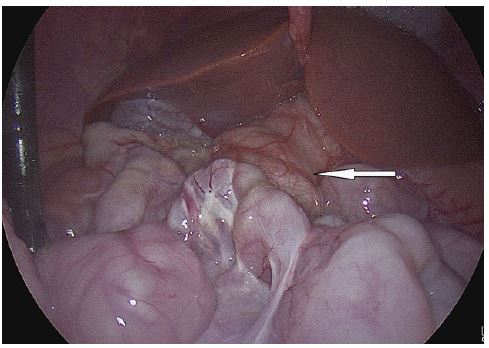
The patient underwent diagnostic laparoscopy through a 5 mm umbilical incision. A small amount of chylous ascites and very prominent lymphatics were noted in the right upper quadrant. A partial volvulus was noted (Figure 5), and the procedure was converted to a laparotomy. Partial recurrent volvulus was confirmed; the bowel had undergone a 270-degree twist. No bowel ischemia was seen. The patient had formed interloop adhesions that had set in such a way that seemed to allow recurrent malrotation, and the mesentery was insufficiently broad or else had scarred into a narrow pedicle with potential for volvulus. A repeat Ladd’s procedure was performed by lysing of all adhesions that were causing this narrow base of mesentery.

Discussion
Intestinal malrotation can be complicated by bowel obstruction due to midgut volvulus or secondary to the presence of obstructing peritoneal bands. Ladd’s procedure is the surgery of choice. It was first described by William E. Ladd in 1936 and has been the preferred surgical procedure for intestinal malrotation repair and midgut volvulus. The procedure includes (a) reduction of midgut volvulus, (b) division of peritoneal bands obstructing the duodenum as well as mesenteric dissection to broaden the small bowel mesentery, (c) placement of the small and large bowel in a state of nonrotation, and (d) appendectomy [1].
There are studies in the literature comparing laparoscopic procedure with Ladd’s surgery [2,3]. Laparoscopic surgery has a longer operative time; however, it has a shorter duration of hospital stays and fewer chances of incision site infection. Open surgery is associated with shorter operating times. Open Ladd’s procedure continues to be the standard of care for patients who present with volvulus [4]. Some surgeons believe this may be because the open approach could facilitate adhesion development, which could keep the small bowel in the nonrotation configuration to decrease the risk for recurrent volvulus [5-7].
Recurrent midgut volvulus after Ladd’s procedure is uncommon. The incidence of recurrent volvulus has been reported to range from 2% [8] to between 5% [9] and 7% [10]. It is a life-threatening emergency requiring prompt diagnosis and surgical intervention. Recurrence of midgut volvulus might reflect decreased adhesion formation and can be prevented by the formation of postsurgical adhesions that restrict the movement of bowel loops [11,12]. Additionally, at surgery, complete dissection of the mesentery following lysis of Ladd’s bands is crucial to ensure a wide-based mesentery. Inadequate mesenteric dissection with a persistently narrowed midgut mesentery might allow the bowel to return to its original orientation, predisposing to recurrent volvulus [13].
Conclusion
Recurrent midgut volvulus after Ladd’s procedure is an uncommon clinical entity. It is a life-threatening emergency and requires awareness of this rare possibility, clinical vigilance, and prompt action. An urgent radiological evaluation should be sought to confirm the diagnosis. The study of choice is a contrast upper gastrointestinal series under fluoroscopic guidance. The patient should be operated upon immediately once the diagnosis is established.
Disclosure of interests
The authors have no competing interests to declare that are relevant to the content of this article.
References
- Strouse PJ. Disorders of intestinal rotation and fixation (“malrotation”). Pediatr Radiol. 2004; 34: 837-851.
- Zhiyi Zhang, Yajun Chen, Jiayu Yan et al. Laparoscopic Versus Open Ladd’s Procedure for Intestinal Malrotation in Infants and Children: A Systematic Review and Meta-Analysis. Journal of Laparoendoscopic & Advanced Surgical Techniques. 2021; 32(1). DOI: 10.1089/lap.2021.0436.
- Weike Xie, Zhongwen Li, Qi Wang et al. Laparoscopic vs open Ladd’s procedure for malrotation in neonates and infants: a propensity score matching analysis. BMC Surg. 2022; 25. https://doi.org/10.1186/s12893-022-01487-1.
- Mubina A Isani, Christopher Schlieve, Jeremy Jackson et al. Is less more? Laparoscopic versus open Ladd’s procedure in children with malrotation. J Surg Res. 2018; 229: 351-356.
- Fraser JD, Aguayo P, Sharp SW, Ostlie DJ, St Peter SD. The role of laparoscopy in the management of malrotation. J Surg Res. 2009;1 56: 80-82.
- Ooms N, Matthyssens LE, Draaisma JM, de Blaauw I, Wijnen MH. Laparoscopic treatment of intestinal malrotation in children. Eur J Pediatr Surg. 2016; 26: 376-381.
- Stanfill AB, Pearl RH, Kalvakuri K, Wallace LJ, VeguntaRK. Laparoscopic Ladd’s procedure: Treatment of choice for midgut malrotation in infants and children. J Laparo-endosc Adv Surg Tech A. 2010; 20: 369-372.
- Feitz R, Vos A. Malrotation: the postoperative period. J Pediatr Surg. 1997; 32: 1322-1324.
- Hiroshi K, Tadashi I. Recurrent midgut volvulus with intestinal malrotation. Jpn J Pediatr Surg. 2005; 37: 813-818
- Schultz LR, Lasher EP, Bill AH. Abnormalities of rotation of the bowel. Am J Surg. 1961; 101: 128-133.
- Bass KD, Rothenberg SS, Chang JH. Laparoscopic Ladd’s procedure in infants with malrotation. J Pediatr Surg. 1998; 33: 279-281.
- Stauffer UG, Herrmann. Comparison of late results in patients with corrected intestinal malrotation with and without fixation of the mesentery. J Pediatr Surg. 1980; 15:9–12.
- Mazeh H, Kaliner E, Udassin R. Three recurrent episodes of malrotation in an infant. J Pediatr Surg. 2007;42: E1–E3.