
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 5
Insights into EJV varix: A comprehensive case report
Diwash Sunar*; Rahul Mahato; Shiva Bhusan Pandit; Aahana Pokharel
Birat Medical College Teaching Hospital, Biratnagar, Nepal
*Corresponding Author : Diwash Sunar
Lecturer, Department of ENT, Birat Medical College Teaching Hospital, Biratnagar, Nepal.
Email: drdiwash1@gmail.com
Received : Mar 24, 2024
Accepted : Apr 10, 2024
Published : Apr 17, 2024
Archived : www.jcimcr.org
Copyright : © Sunar D (2024).
Citation: Sunar D, Mahato R, Bhusan Pandit S, Pokharel A. Insights into EJV varix: A comprehensive case report. J Clin Images Med Case Rep. 2024; 5(4): 2991.
Introduction
Venous aneurysms originating from the External Jugular Vein (EJV) are uncommon, with those arising from the internal jugular vein being more prevalent. Spontaneous EJV aneurysms are exceedingly rare, leading to ongoing debates regarding their management [1]. Varix of the EJV often manifests as an abnormal sacculofusiform dilation, typically discovered incidentally, and its etiology remains unclear. The preferred diagnostic method involves ultrasonography with Doppler before, during, and after the Valsalva manoeuvre. A high index of suspicion is essential for diagnosing this condition [2]. These aneurysms are typically viewed as benign abnormalities requiring treatment primarily for cosmetic reasons, with open surgical intervention being the preferred therapeutic approach [3].
Case report
A 34-year-old female presented with a swelling on the right side of her neck persisting for 6 years. The swelling had developed gradually, remained stable in size, and occurred intermittently without causing pain. It would become more noticeable during activities such as coughing, straining, and performing the Valsalva maneuver (Figures 1 and 2). The patient denied experiencing any voice changes, difficulty swallowing, or breathing difficulties. There was no history of neck trauma or surgery, nor did the patient report any significant medical illnesses.
Upon physical examination, no abnormalities were noted at rest. However, during the Valsalva maneuver, a swelling was observed on the right side of the neck, lateral to the sternocleidomastoid muscle at the level of the middle third, measuring 4x3 cm. The swelling was found to be compressible, soft, and non-tender, with pinchable and normal skin overlying it. No pulsations were observed. Videolaryngoscopy revealed a normal larynx and hypopharynx. Examination of other systems yielded normal results. A mediastinal mass was ruled out through a chest X-ray, which showed no widening, and a laryngocele was excluded as no air was observed in the region of the mass.
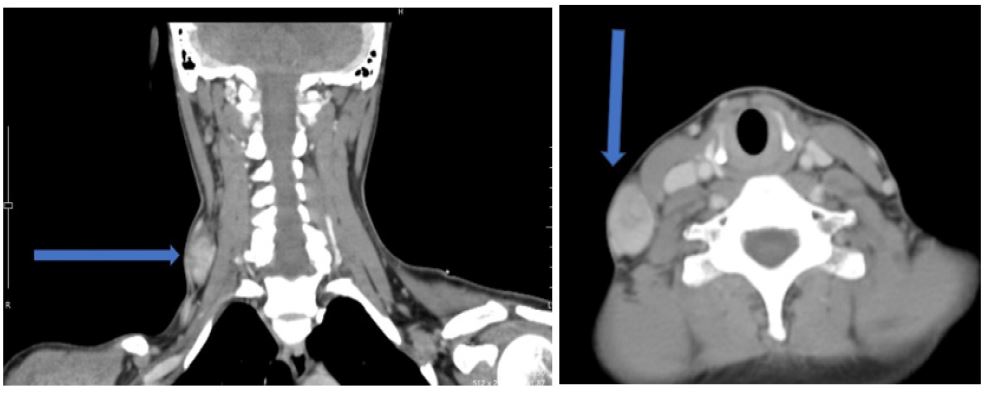
The diagnosis was favoured by Ultrasonography with Doppler, revealing a hypoechoic lesion in the lateral neck that was continuous with the superficial vein (EJV). Turbulent flow was observed within the lesion, and its size increased during the Valsalva maneuver. Computed tomography of neck revealed segmental aneurysmal dilatation of right EJV in neck at the level of C6-C7 vertebrae. The dilated segment measured 37.5x26.3 mm (Figures 3 and 4)


Discussion
A venous aneurysm refers to the dilation of a specific segment of a vein, where the diameter expands to at least 1.5 times that of the non-dilated portion of the vein. This dilation encompasses all three layers of the vein wall. It is characterised by a single channel communicating with the main vein and is not associated with varicosities or arteriovenous communications [4]. Jugular venous aneurysms are uncommon occurrences, largely due to the superior vena cava being a low-pressure system with distensible walls and gravity-assisted drainage. Among the jugular veins, the internal jugular vein is most frequently affected [5]. The occurrence of spontaneous External Jugular Vein (EJV) aneurysms in patients is highly uncommon.
External Jugular Vein (EJV) aneurysms can arise from either congenital or acquired causes. Fusiform aneurysms typically have a congenital origin, whereas saccular aneurysms may develop spontaneously or as a result of various factors such as inflammation, malignancy, trauma (e.g., cannulation), or arteriovenous fistulas [6]. The majority of EJV aneurysms are asymptomatic. However, some patients may experience mild discomfort or painful swelling, primarily attributed to thrombus formation within the aneurysm, phlebitis, or pressure effects on surrounding structures. Typically, they manifest as a unilateral, soft, reducible, non-pulsatile swelling superficial to the sternosternocleidomastoid muscle along the course of the external jugular vein. This swelling tends to enlarge during activities such as straining, crying, bending, breath-holding, sneezing, or coughing [5].
The majority of authors do not advocate surgery for this benign and self-limiting condition, instead recommending conservative follow-up [4-6]. However, surgery may be recommended for cosmetic reasons or if complications such as hoarseness, stridor, or dysphagia arise. The standard surgical procedure typically involves resection of the dilated segment after ligating the feeding vessels [7].
In our case, since the patient was asymptomatic and the size of the swelling remained stable. The patient was counselled regarding the nature of the swelling and was informed about the worrisome symptoms that may arise out of swelling such as hoarseness, dysphagia, pain and sudden rise in size of the swelling. She was asked for regular follow-up at our centre.
References
- Thakur UK, Savlania A, Naik AL, Singh C, Chatterjee D, Gorsi U. Clinical profile and management of external jugular vein aneurysms. Phlebology. 2021; 36(5): 401-406. doi:10.1177/0268355520975583.
- Vinod Kumar G, Ranganatha Reddy B, Bhat SM, Vuppala R. An Intriguing Case of Ectasia of External Jugular Vein Presenting as Intermittent Neck Mass. Indian J Otolaryngol Head Neck Surg. 2016; 68(3): 367-9. doi: 10.1007/s12070-015-0911-y. Epub 2015 Sep 29. PMID: 27508141; PMCID: PMC4961637.
- Nakajima Y, Murata M, Shudo K, Yoshikawa K. External Jugular Venous Aneurysm: A Case Report. Plast Reconstr Surg Glob Open. 2022; 10(10): 4617. doi: 10.1097/GOX.0000000000004617. PMID: 36299812; PMCID: PMC9592330.
- Nana P, Korais C, Mpouronikou A, Lachanas V, Spanos K, Kouvelos G. Management of an external jugular vein aneurysm in a young patient. J Vasc Surg Venous Lymphat Disord. 2020; 8(5): 861-863. doi: 10.1016/j.jvsv.2020.03.002. Epub 2020 Apr 19. PMID: 32321691.
- Mohanty D, Jain BK, Garg PK, et al. External jugular venous aneurysm: a clinical curiosity. J Nat Sci Biol Med 2013; 4: 223-225.
- Schatz IJ and Fine G. Venous aneurysms. N Engl J Med. 1962; 266: 1310-1312.
- Bowdler DA, Singh SD Internal jugular phlebectasia. Int J Pediatr Otorhinolaryngol. 1986; 12: 165-171.