
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Pierre marie bamberger or hypertrophic osteoarthropathy syndrome: Paranoplastic syndrome revealing lung tumor
Fjouji S1*; Bakkali H2; Houba A2; Kartit N2; Doghmi N2; Balkhi H2
1Hassan II University, Casablanca, Morocco.
2Mohamed V University, Rabat, Morocco.
*Corresponding Author : Fjouji Salaheddine
Hassan II university, Casablanca, Morocco.
Email: fjoujisalah@gmail.com
Received : Mar 24, 2024
Accepted : Apr 10, 2024
Published : Apr 17, 2024
Archived : www.jcimcr.org
Copyright : © Fjouji S (2024).
Abstract
Hypertrophic osteoarthropathy, known as Pierre Marie Bamberger syndrome, is characterized by clubbing of the fingers due to bone surface and soft tissue calcification, historically known as pulmonary carcinoma paraneoplastic syndrome. The clinical symptoms can easily misdiagnosed as autoimmune diseases. We describe the case of a 66-year-old man who presented with dyspnea with clubbing of the fingers. The exploration reveal an adenocarcinoma. The evolution was fatal. This report has highlighted the importance of clinical awareness of the association between HOA and carcinoma of the lung.
Keywords: Osteoarthropathy; Pierre marie bamberger; Paraneoplasic; Adenocarcinoma; Lung tumors.
Citation: Fjouji S, Bakkali H, Houba A, Kartit N, Doghmi N, et al. Pierre marie bamberger or hypertrophic osteoarthropathy syndrome: Paranoplastic syndrome revealing lung tumor. J Clin Images Med Case Rep. 2024; 5(4): 2992.
Introduction
Hypertrophic osteoarthropathy, known as Pierre Marie Bamberger syndrome, is characterized by clubbing of the fingers due to bone surface and soft tissue calcification. The age of onset is mainly middle-aged and old people [1]. Clinical signs may suggest etiologies other than neoplasy.
Case report
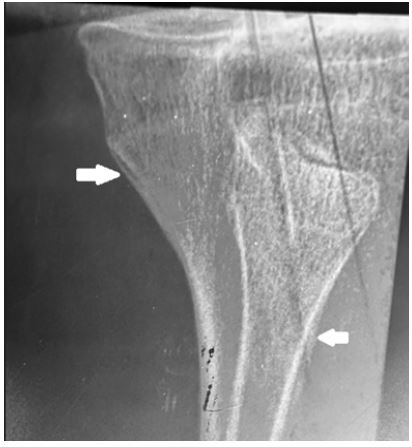
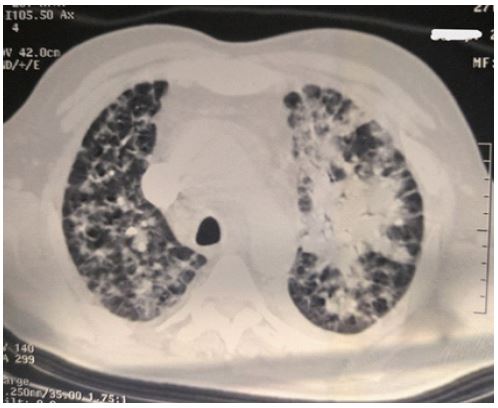
66-year-old man presented with joint swelling affecting the interphalangeal joints of the hands with finger clubbing (Figure 1) associated with exertional dyspnea with increasing asthenia over the past month. In the history, he is a 45 pack year smoker, stpped 5 years ago and is hypertensive on amlodipine 10 mg/day. On clinical examination, clubbing with hypertrophied hand joints. On the respiratory level, a respiratory frequency of 25 cycles per minute, desaturation of 88%, bilateral snoring rales more marked on the left. Biologically, there was a moderate inflammatory syndrome (white blood cells at 12.000 per mm3, C-reactive protein at 34 mg/l. The x-ray of the lower limb revealed lamellar periosteal apposition of the tibial diaphyses suggesting hypertrophic osteoarthropathy (Figure 2). Thoracic CT imaging revealed an appearance suggestive of a left lung tumor and bilateral interstitial and micronodular syndrome (Figure 3). After bronchoscopy and biopsy, a diagnosis of adenocarcinoma is made. The patient is admitted to the intensive care unit. Oxygen therapy with a high concentration mask, antibiotic therapy with ceftazidim and amikacin. The evolution was marked by clinical worsening. The patient after failure of non-invasive ventilation was intubated and placed on mechanical ventilation. A refractory acute respiratory distress syndrome is established. Death occurred after 5 days due to hypoxia and multiorgan failure.

Discussion
Hypertrophic Osteoarthropathy (HOA) is a syndrome manifesting bony deformities and multi-organ involvement [2]. Firstly described in 1889 by Bamberger and followed by further research by Pierre Marie in 1890, hence the name Pierre Marie–Bamberger (PMB) disease was coined [3]. PMB is arheumatologic disease with variable presentations. The common features include digital clubbing, increase in size of the limbs secondary to bone and periarticular tissue proliferation, arthralgia with edema, bilateral eyelid ptosis, leonine facies, and thickening of the skin. Histological examination of tissue biopsy shows hyperplasia of the adjacent subcutaneous tissue [4]. The physiopathology of digital clubbing still remains unknown and the same applies to the rest of the findings associated with HOA. Several underlying mechanisms associated with HOA development have been investigated, including abnormal vascularization, hypoxia, and chronic inflammation [5-7]. HOA incidence in cases of primary lung carcinoma in the USA published in the 1980s put the occurrence at 0.8% [8]. HOA is an uncommon paraneoplastic syndrome which is frequently associated with pulmonary tumor [9]. It occurs secondarily to conditions characterized by arteriovenous shunt like lung carcinoma, mesothelioma, pulmonary tuberculosis, congenital cyanotic heart disease, hepatic and colorectal carcinoma, inflammatory bowel disease, cirrhosis, pulmonary fibrosis and empyema [10]. The clinical symptoms can easily misdiagnosed as autoimmune diseases [11]. The prognosis and treatment of Secondary HOA is naturally linked to the primary aetiology [12]. The attenuation of signs and symptoms following treatment of the underlying pathology has been reported in the current literature [13]. With tumor, it is associated with an underlying multiorgan involvement and often has a fatal course.
Conclusion
Clinical and radiographic evidence allows the diagnosis of hypertrophic osteoarthropathy. Until proven otherwise, it is considered a paraneoplastic syndrome and physiciens should search for lung cancer or other neoplasy. The prognosis and treatment are naturally linked to the primary aetiology.
References
- Krugh M, Vaidya PN. Osteoarthropathy Hypertrophic. StatPearls. Treasure Island (FL). 2020.
- Nguyen, Sheila, and Mehrnaz Hojjati. “Review of current therapies for secondary hypertrophic pulmonary osteoarthropathy.” Clinical rheumatology. 2011; 30: 7-13.
- Carvalho, Tarcísio Nunes, et al. “Osteoartropatia hipertrófica primária (paquidermoperiostose): relato de casos em dois irmãos.” Radiologia Brasileira. 2004; 37: 147-149.
- Segal AM, Mackenzie AH. Hypertrophic osteoarthropathy: a 10-year retrospective analysis. Semin Arthritis Rheum. 1982; 12: 220-32.
- Chakraborty RK, Sharma S. Treasure Island (FL): StatPearls [Internet]; Secondary Hypertrophic Osteoarthropathy. 2022.
- Clubbing and hypertrophic osteoarthropathy: insights in diagnosis, pathophysiology, and clinical significance. Callemeyn J, Van Haecke P, Peetermans WE, Blockmans D. Acta Clin Belg. 2016; 71: 123-130.
- Vascular endothelial growth factor (VEGF)-A and platelet-derived growth factor (PDGF) play a central role in the pathogenesis of digital clubbing. Atkinson S, Fox SB. J Pathol. 2004; 203: 721-728.
- Martinez-Lavin, Manuel, et al. “Evidence of hypertrophic osteoarthropathy in human skeletal remains from pre-Hispanic Mesoamerica.” Annals of internal medicine. 1994; 120.3: 238-241.
- Armstrong, David J, Elisabeth MA McCausland, and Gary D. Wright. “Hypertrophic pulmonary osteoarthropathy (HPOA) (Pierre Marie–Bamberger syndrome): two cases presenting as acute inflammatory arthritis. Description and review of the literature.” Rheumatology international. 2007; 27: 399-402.
- Vandemergel X, and G. Decaux. “Review on hypertrophic osteoarthropathy and digital clubbing.” Revue Medicale de Bruxelles. 2003; 24.2: 88-94.
- Zhao, Maoyuan, et al. “Hypertrophic pulmonary osteoarthropathy with esophageal sarcomatoid carcinoma: a case report.” Annals of Palliative Medicine. 2021; 10.5: 5862869-5865869.
- Pourmorteza, Mehdi, et al. “Hypertrophic pulmonary osteoarthropathy: a rare but treatable condition in palliative medicine.” Journal of Pain and Symptom Management. 2015; 50.2: 263-267.
- Koliakos E, Chappalley D, Kalogiannis E, Sgardello S, Christodoulou M. Pierre-Marie Bamberger Syndrome Leading to the Diagnosis and Surgical Treatment of a Localized Lung Cancer. Cureus. 2023; 15(11): 48991. The prognosis and treatment of secoHAO are n.