
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Chronic back pain in untreated gout
Syang Pyng Gan1*, Nurashikin Jamaluddin2
1Department of General Medicine, Rheumatology Unit, Hospital Sultan Idris Shah, Serdang, Ministry of Health, Malaysia.
2Radiology Department, Hospital Sultan Idris Shah, Serdang, Ministry of Health, Malaysia.
*Corresponding Author : Syang Pyng Gan
Department of General Medicine, Rheumatology Unit, Hospital Sultan Idris Shah, Serdang, Ministry of Health, Malaysia.
Email: gs_pyng@yahoo.com
Received : Mar 26, 2024
Accepted : Apr 10, 2024
Published : Apr 17, 2024
Archived : www.jcimcr.org
Copyright : © Pyng Gan S (2024).
Citation: Pyng Gan S, Jamaluddin N. Chronic back pain in untreated gout. J Clin Images Med Case Rep. 2024; 5(4): 2993.
Description
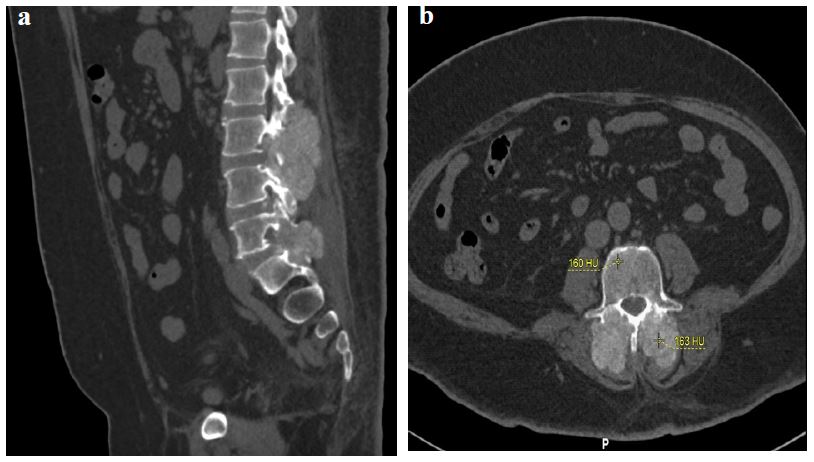
A 41-year-old man with a 10-year history of untreated chronic tophaceous gout presented with acute flare of gouty arthritis. He has chronic low back pain which has become more severe for the past 1 year. Clinically he has tenderness at lower lumbar spine although there was no neurological deficit. Laboratory test revealed raised inflammatory markers (ESR 70mm/hour) and C-reactive protein 287.1 mg/L, reactive thrombocytosis and leucocytosis, renal impairment and elevated serum uric acid (780 μmol/L). He had microscopic hematuria and ultrasound showed right mild hydronephrosis without any calculi identified. Computerized Tomography Urogram (CTU) confirmed the findings of an obstructive right hydronephrosis and hydroureter due to a right ureteric calculus. Incidentally, CTU revealed a lobulated, heterogenous hyperdense soft tissue ossified mass measuring (4.6x7.3x8.1 cm) at lumbar vertebral bodies (L2-L4) with overhanging edge erosions of adjacent vertebra mainly involving the facet joints, pedicles and lamina (Figure 1).
Based on the clinical and typical radiographic findings, spinal gout was diagnosed. Patient was however, not keen for a CT-guided biopsy for a confirmation of spinal tophi. Right nephrotomy was performed for the obstructive right hydronephrosis. Urate lowering therapy was started with the aim to target serum uric acid level less than 300 μmol/L, as recommended.
Spinal gout is often an underdiagnosed clinical manifestation of gout [1], with diagnostic challenges. Histopathological examination of the spinal mass is important for confirmation of gout [2]. However, tissue biopsy is invasive and is therefore, not always feasible. Dual-energy Computerized Tomography is a non-invasive imaging technique to look for monosodium urate deposition [3] but this modality is yet to be widely available. Hence pathognomonic radiological changes of gout in CT imaging play a crucial role in diagnosis. A diagnosis of spinal gout needs to be considered in patients with poorly controlled gout who present with back pain or neurological deficits.
References
- Ma SL, Zhao JH, Jiang R, An QM, Gu R. Diagnostic challenges of spinal gout. Medicine. 2019; 98: 16(e15265).
- Elgafy H, Liu XC, Herron J. Spinal gout: A review with case illustration. World J Orthop. 2016; 7(11): 766-775.
- Desai MA, Peterson JJ, Garner HW, Kransdorf MJ. Clinical utility of dual-energy CT for evaluation of tophaceous gout. Radiographics. 2011; 31(5): 1365-75.