
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Cracked tooth and endodontic-periodontal lesion: 2-years follow up of a conservative treatment
Carolina S Santinoni, DDS, PhD1*; Anderson Catelan, DDS, PhD2; Adrieli de Paula Couto Neves, DD, MSc3; Maurício Malheiros Badaró, DDS, PhD1; Danilo Louzada de Oliveira, DDS, PhD3; Rodrigo Vieira Caixeta, DDS, PhD3; Graziela Garrido Mori, DDS, PhD3; Christine Men Martins, DDS, PhD3; Victor Eduardo de Souza Batista, DDS, PhD2,3
1Dental School, Federal University of Santa Catarina, Florianópolis, SC, Brazil.
2Dental School, São Paulo State University - UNESP, Araçatuba, SP, Brazil.
3Dental School, University of Western Sao Paulo, Presidente Prudente, SP, Brazil.
*Corresponding Author : Carolina S Santinoni
Dental School, Federal University of Santa Catarina, Florianópolis, SC, Brazil.
Tel: +55 (48) 3721-3461;
Email: carolsantinoni@msn.com
Received : Mar 26, 2024
Accepted : Apr 11, 2024s
Published : Apr 18, 2024
Archived : www.jcimcr.org
Copyright : © Santinoni CS (2024).
Abstract
This study report diagnosis and management of an endodontic-periodontal lesion in a cracked mandibular tooth after a cyclist’s fall. A 34-year-old female patient with a chief complaint of pain and edema in the region of the mandibular right first molar was evaluated and treated. Patient presented excellent oral health. After clinical, radiographical and tomographic exams, it was diagnosed an acute periapical abscess in stage II combined with tooth cracks and a periodontal involvement (endodontic-periodontal lesion). After emergency dental care it was performed subgingival scaling and root planing, definitive endodontic treatment, indirect definitive restoration (overlay) combined with a reinforcement of the tooth structure with a high-resistance polyethylene tape. Patient was periodically followed up until 24 months and treatment was successful. It can be concluded that a correct diagnosis and a conservative and well-planned and -executed treatment of a compromised tooth by cracks can have good results even endodontic-periodontal lesion is present.
Keywords: Periodontium; Esthetics; Dental prosthesis; Smiling.
Citation: Santinoni CS, Catelan A, Neves ADPC, Badaró MM, Oliveira DLD, et al. Cracked tooth and endodontic-periodontal lesion: 2-years follow up of a conservative treatment. J Clin Images Med Case Rep. 2024; 5(4): 2996.
Introduction
Endodontic-Periodontal Lesions (EPL) may occur in acute or chronic forms, can compromise patients with or without periodontitis and occur clinically when there is simultaneous combination of pathological conditions through communication of periodontium and dental pulp in anatomical or pathological (cracks or root fractures) forms [1,2]. Among signs and symptoms are deep periodontal pocket or bone resorption in the apical or furcation region, spontaneous or stimulated pain, purulent exudate, tooth mobility, and negative or altered response to vitality test [3].
There is no consensus regarding therapeutic options, but challenge is preserving the tooth in oral cavity in healthy conditions and eradication of infection in periodontal tissues and root canals [3,4]. Tooth and periodontal commitment degree have direct impact on its prognosis and treatment, such as presence of fractures, cracks and perforations, presence or absence of periodontitis and the extent of periodontal destruction [3].
As well as EPL, cracked tooth present difficult prognosis due to lack of definitive method of establishment how far the microcracks has progressed [4,5]. Multiple factors such as excessive bite force and thermal cycling can cause cracked tooth extending from occlusal surface without separation of tooth fragments or damage the tooth structure [6,7]. Diagnosis is huge important and based on clinical symptoms including spontaneous, cold irritation and bite pain [8]. Rehabilitation of heavily damaged tooth poses a challenge to clinicians [9]. Intra coronal strengthening of teeth is a promising treatment option, particularly in posterior teeth where the stresses generated by forces of occlusion can lead to the fracture of unprotected cusps [10]. Efficient restorative materials also help to increase their survival and prevent tooth loss and additional costs [9].
The purpose of the present study is to report diagnosis and a conservative management option of a cracked tooth combined with endodontic-periodontal lesion.
Case report
This case report has been written according to Preferred Reporting Items for Case reports in Endodontics (PRICE) 2020 guidelines [11].
Patient consented to the publication of the case. A 34-year-old female patient presented to the Dental School of Presidente Prudente with a chief complaint of pain and edema in the mandibular right first molar region. She reported suffered a fall from a bicycle approximately five days before these symptoms and had taken anti-inflammatories (nimesulide) and analgesics (dipyron) prescribed by the doctor who provided emergency care to relieve the symptoms related to the fall.
Regarding dental history, patient reported she has routine appointments annually to certify her oral health and had finished orthodontic treatment with clear aligners about 3 months before. She was using orthodontic containment (acrylic plate) in both arcades. She also reported that she was going through a phase of professional changes that was making her anxious and that she was experiencing nocturnal tooth clenching. She felt that there was stronger contact on the mandibular right first molar, but that since she is a dentist, she was following the symptoms before looking for the professional again.
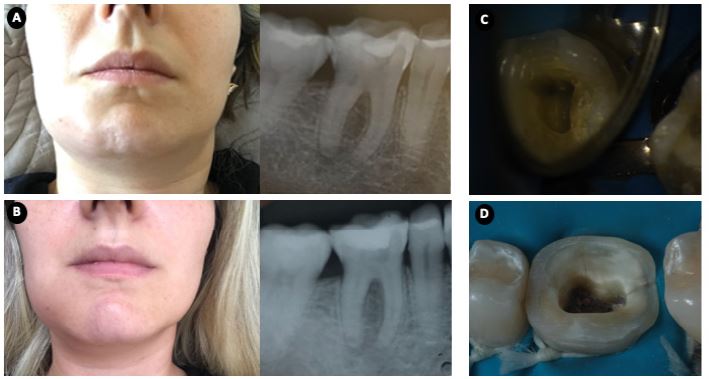
Upon clinical examination, it was observed extra oral edema in the right mandibular region (Figure 1A) and intraoral edema in the apical region of the mandibular right first molar. Tooth had a composite resin restoration with darkened margins but no evidence of active caries, did not respond to the cold thermal test and responded positively to the vertical and horizontal percussion tests. Radiographic analysis revealed a radiolucent area in the furcation region (Figure 1B). Endodontic diagnosis was acute periapical abscess in stage II.
After patient have signed the consent form for the treatment, emergency care was performed by an endodontist: abscess drainage after crown opening, formocresol-based intracanal medication and double provisional restoration (Coltosol and glass ionomer cement). Abscess drainage concurrently occurred by periodontal pathway. Patient was instructed to perform warm water homemade mouthwashes and was daily monitored for infection control certification. Orthodontic containment was suspense. It was prescribed antibiotic (azithromycin 500 mg for 5 days) and analgesic (paracetamol 750 mg) for 3 days.
After 3 days, it was observed an improvement in extraoral edema (Figures 1C and D), but there was recurrence of purulent secretion in gingival sulcus after 1 week. Specialist suspected periodontal involvement combined to endodontic lesion and referred the patient to a periodontist that observed presence of a deep periodontal pocket (6 mm) on the buccal surface of the lower right first molar. Subgingival Scaling and Root Planing (SRP) was performed (9-10 Gracey curette), followed by subgingival irrigation with tetracycline solution at 10 mg/ml. At that time, the formocresol-based intracanal medication was also renewed by the endodontist and with EPL diagnosis, amoxicillin 500 mg associated with metronidazole 250 mg was also prescribed for 7 days.
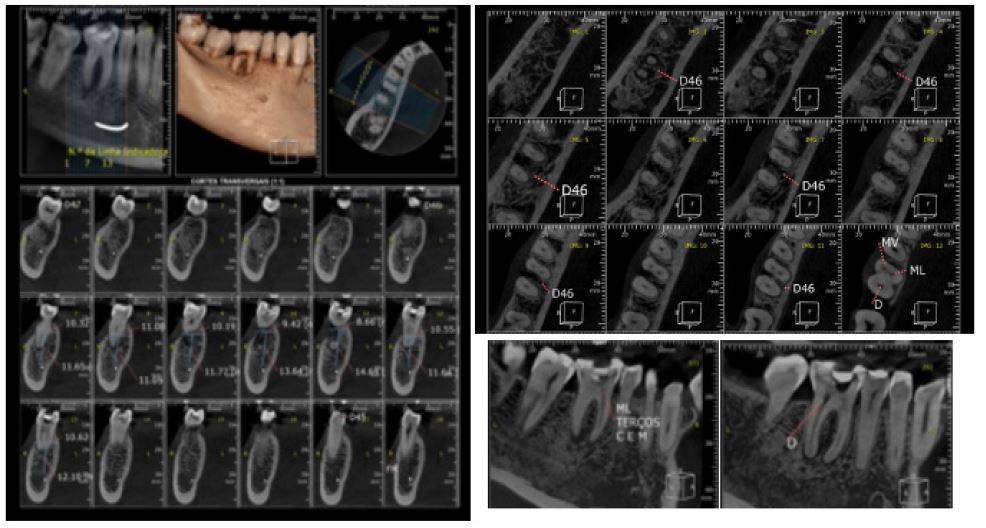
Due to excellent general oral health condition of the patient and history of nocturnal tooth clenching, the professionals suspected that there was some tooth crack involved in this acute pathology, allowing the communication between the endodontic and periodontal lesions. A tomography was requested (Figure 2) but it only confirmed endodontic and periodontal involvement and did not the presence of coronal or root cracks. Presence of the cracks was clinically confirmed in the distal region of the crown and on the floor of the pulp chamber (Figure 3) with clinical microscope aid in the next appointment when the endodontist performed the instrumentation of the root canals and completely removed the composite resin restoration.
Endodontic reciprocating instrumentation was performed followed by irrigation solution agitation easy clean protocol (Table 1). After 2% chlorhexidine 2% kept for 5 minutes, intracanal medication of calcium hydroxide, iodoform and propylene glycol for 14 days, it was double sealed again. After clinical silence, definitive obturation was performed with gutta percha cones and endodontic sealers (Sealapex).
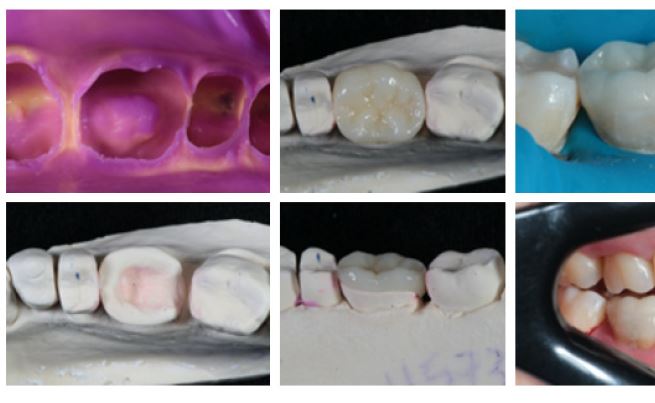
Definitive tooth restoration with ceramic-based overlay was planned. To reinforce the tooth structure due to the presence of cracks, a high-resistance polyethylene tape and dentin seal with flow resin was performed in the region of the floor of the pulp chamber (Figures 4 and 5). Occlusal adjustment was performed. At this time, the patient reported that she was no longer going through the anxiety phase and the nocturnal clenching of teeth had disappeared.
Patient was satisfied with the treatment performed and has attended follow-up consultations every 6 months (24 months for now after finishing rehabilitation phase) to monitor the tooth due to the presence of the cracks with a sensitive prognosis. Teeth did not move despite the using suspense of the orthodontic containment. Considering good results obtained with this conservative treatment, it was considered well-successes.
Table 1: Easyclean disinfection protocol.
| Solution | Frequency | Time |
|---|---|---|
| 2.5 % sodium hypochlorite | 3 times | 20 seconds |
| Trisodium ethylene diamine tetra acetic acid | 3 times | 20 seconds |
| Saline | 3 times | 20 seconds |

Discussion
In the reported case, patient used anti-inflammatory drugs after the bicycle fall. It can be inferred that these drugs reduced their immune defense capacity and that the pulp already affected by excessive occlusal forces due to nocturnal tooth clenching. Pulp commitment after occlusal disfunctions can occur aseptically due to damage of apical blood vessels which may follow to necrosis [12]. In this case, the infection can affect periapical tissues due to a host defense inability to stop the microorganism invasion [13-15]. In this context, previous studies demonstrated prolonged use of corticosteroids accelerates pulp necrosis and modifies bone loss in rat-induced apical periodontitis [16]. Osteopenia and immunosuppression caused by steroids use in the presence of a periodontal pathogens may also be an aggravating factor in periodontitis [17].
Acute apical abscess is an inflammatory reaction where lipopolysaccharides and lipoteichoic acid are endotoxins released during bacterial multiplication or death that lead to periapical bone resorption [18-27]. Although broad-spectrum antibiotic was used in the patient dental emergency care, the infection persisted after few days probably due to the presence of this endotoxins and biofilm protection in periapical and periodontal tissues. Lipoteichoic acid present could favored bacterial adhesion by acting to form bacterial biofilms and consequently increased the bacterial resistance to antibiotic used [18,24-26]. After subgingival SRP, new endodontic instrumentation, and second round prescription of systemic antibiotics, infection was solved. It has been demonstrated systemic administration of amoxicillin and metronidazole combined with SRP to treat severe periodontitis in young patients in a challenging condition promoted a beneficial change in the microbiome and remains the most effective therapy [28,29].
Innovative technology use to help diagnosis and facilitate the treatment of cracked tooth has been reported in other clinical reports [6,30]. In the present case, definitive restoration of the tooth with ceramic-based overlay combined with a tooth structure reinforcement with high-resistance polyethylene tape sealed with flow resin in the pulp chamber floor was proposed as conservative but effective treatment. It has demonstrated good results after 2 years. Similarly, Mahgoli et al. [6] suggested this technique for restoration and preservation of teeth with transverse cracks involving the pulp chamber floor with main advantage of postpone or avoid tooth extraction [6]. Also, it impedes crack propagation and splitting of the tooth for up 10 years [6].
It can be concluded correct diagnosis and a conservative but well-planned and -executed treatment of a compromised tooth by cracks can have good results even endodontic-periodontal lesion is present.
Acknowledgments: Not applicable.
Competing interests: The authors declare there is no conflict of interests.
References
- Razi MA, Mahajan A, Qamar S, Mehra S, Roy TR, Kumari P. A Comparative Study of Platelet-rich Fibrin (PRF) and Titanium-prepared Platelet-rich Fibrin (T-PRF) in Management of Endoperio Lesions. J Contemp Dent Pract. 2020; 21(9): 997-1001. Published 2020 Sep 1.
- Herrera D, Retamal-Valdes B, Alonso B, Feres M. Acute periodontal lesions (periodontal abscesses and necrotizing periodontal diseases) and endo-periodontal lesions. J Periodontol. 2018; 89: S85-S102. doi:10.1002/JPER.16-0642.
- Ardila CM, Vivares-Builes AM. Clinical Efficacy of Treatment of Endodontic-Periodontal Lesions: A Systematic Scoping Review of Experimental Studies. Int J Environ Res Public Health. 2022; 19(20): 13649. Published 2022 Oct 21. doi:10.3390/ijerph192013649.
- Lee TY, Yang SE, Kim HM, Kye MJ. Characteristics, Treatment, and Prognosis of Cracked Teeth: A Comparison with Data from 10 Years Ago. Eur J Dent. 2021; 15(4): 694-701. doi:10.1055/s-0041-1728842.
- Tan L, Chen NN, Poon CY, Wong HB. Survival of root filled cracked teeth in a tertiary institution. Int Endod J. 2006; 39(11): 886-889. doi:10.1111/j.1365-2591.2006.01165.x.
- Mahgoli HA, Arshad M, Rasouli K. Restoration of endodontically treated cracked maxillary teeth: A case series. Clin Case Rep. 2019; 7(10): 1951-1956. Published 2019 Sep 1. doi:10.1002/ccr3.2391.
- Qiao F, Chen M, Hu X, et al. Cracked Teeth and Poor Oral Masticatory Habits: A Matched Case-control Study in China. J Endod. 2017; 43(6): 885-889. doi: 10.1016/j.joen.2017.01.007.
- Signore A, Benedicenti S, Covani U, Ravera G. A 4- to 6-year retrospective clinical study of cracked teeth restored with bonded indirect resin composite onlays. Int J Prosthodont. 2007; 20(6): 609-616.
- Soares R, de Ataide Ide N, Fernandes M, Lambor R. Fibre reinforcement in a structurally compromised endodontically treated molar: a case report. Restor Dent Endod. 2016; 41(2): 143-147. doi:10.5395/rde.2016.41.2.143.
- Shivanna V, Gopeshetti PB. Fracture resistance of endodontically treated teeth restored with composite resin reinforced with polyethylene fibres. Endodontology. 2013; 24: 73-79.
- Nagendrababu V, Chong BS, McCabe P, Shah PK, Priya E, Jayaraman J, Pulikkotil SJ, Setzer FC, Sunde PT, Dummer PMH. PRICE 2020 guidelines for reporting case reports in Endodontics: a consensus-based development. Int Endod J. 2020; 53(5): 619-626. doi: 10.1111/iej.13285.
- Berlin-Broner Y, Febbraio M, Levin L. Association between apical periodontitis and cardiovascular diseases: a systematic review of the literature. Int Endod J. 2017; 50(9): 847-859. doi:10.1111/iej.12710.
- Gund MP, Wrbas KT, Hannig M, Rupf S. Apical periodontitis after intense bruxism. BMC Oral Health. 2022; 22(1): 91. Published 2022 Mar 24. doi:10.1186/s12903-022-02123-3.
- Nair PN. Pathogenesis of apical periodontitis and the causes of endodontic failures. Crit Rev Oral Biol Med. 2004; 15(6): 348-381. Published 2004 Nov 1. doi:10.1177/154411130401500604
- Xiong H, Wei L, Hu Y, Zhang C, Peng B. Effect of alendronate on alveolar bone resorption and angiogenesis in rats with experimental periapical lesions. Int Endod J. 2010; 43(6): 485-491. doi:10.1111/j.1365-2591.2010.01703.x.
- do Nascimento IV, Rodrigues MIQ, Isaias PHC, et al. Chronic systemic corticosteroid therapy influences the development of pulp necrosis and experimental apical periodontitis, exacerbating the inflammatory process and bone resorption in rats. Int Endod J. 2022; 55(6): 646-659. doi:10.1111/iej.13724.
- von Wowern N, Klausen B, Olgaard K. Steroid-induced mandibular bone loss in relation to marginal periodontal changes. J Clin Periodontol. 1992; 19(3): 182-186. doi:10.1111/j.1600-051x.1992.tb00636.x.
- Gabrielli ES, Lima AR, Francisco PA, et al. Comparative analysis of bacterial content, levels of lipopolysaccharides and lipoteichoic acid in symptomatic and asymptomatic endodontic infections at different stages of endodontic treatment. Clin Oral Investig. 2022; 26(1): 287-302. doi:10.1007/s00784-021-03998-2.
- Aveiro E, Chiarelli-Neto VM, de-Jesus-Soares A, et al. Efficacy of reciprocating and ultrasonic activation of 6% sodium hypochlorite in the reduction of microbial content and virulence factors in teeth with primary endodontic infection. Int Endod J. 2020; 53(5): 604-618. doi:10.1111/iej.13261.
- Gomes BPFA, Herrera DR. Etiologic role of root canal infection in apical periodontitis and its relationship with clinical symptomatology. Braz Oral Res. 2018; 32(1): 69. Published 2018 Oct 18. doi:10.1590/1807-3107bor-2018.vol32.0069.
- Martinho FC, Chiesa WM, Leite FR, Cirelli JA, Gomes BP. Correlation between clinical/radiographic features and inflammatory cytokine networks produced by macrophages stimulated with endodontic content. J Endod. 2012; 38(6): 740-745. doi: 10.1016/j.joen.2012.02.021
- Martinho FC, Chiesa WM, Leite FR, Cirelli JA, Gomes BP. Antigenic activity of bacterial endodontic contents from primary root canal infection with periapical lesions against macrophage in the release of interleukin-1beta and tumor necrosis factor alpha. J Endod. 2010; 36(9): 1467-1474. doi: 10.1016/j.joen.2010.06.012.
- Gomes BP, Martinho FC, Vianna ME. Comparison of 2.5% sodium hypochlorite and 2% chlorhexidine gel on oral bacterial lipopolysaccharide reduction from primarily infected root canals. J Endod. 2009; 35(10): 1350-1353. doi: 10.1016/j.joen.2009.06.011
- Baik JE, Ryu YH, Han JY, et al. Lipoteichoic acid partially contributes to the inflammatory responses to Enterococcus faecalis. J Endod. 2008; 34(8): 975-982. doi: 10.1016/j.joen.2008.05.005.
- Fabretti F, Theilacker C, Baldassarri L, et al. Alanine esters of enterococcal lipoteichoic acid play a role in biofilm formation and resistance to antimicrobial peptides. Infect Immun. 2006; 74(7): 4164-4171. doi:10.1128/IAI.00111-06.
- Ginsburg I. Role of lipoteichoic acid in infection and inflammation. Lancet Infect Dis. 2002; 2(3): 171-179. doi:10.1016/s1473-3099(02)00226-8.
- Darveau RP, Hancock RE. Procedure for isolation of bacterial lipopolysaccharides from both smooth and rough Pseudomonas aeruginosa and Salmonella typhimurium strains. J Bacteriol. 1983; 155(2): 831-838. doi:10.1128/jb.155.2.831-838.1983.
- Feres M, Retamal-Valdes B, Fermiano D, et al. Microbiome changes in young periodontitis patients treated with adjunctive metronidazole and amoxicillin. J Periodontol. 2021; 92(4): 467-478. doi:10.1002/JPER.20-0128.
- Rabelo CC, Feres M, Gonçalves C, et al. Systemic antibiotics in the treatment of aggressive periodontitis. A systematic review and a Bayesian Network meta-analysis. J Clin Periodontol. 2015; 42(7): 647-657. doi:10.1111/jcpe.12427.
- Jun MK, Park SW, Lee ES, Kim BR, Kim BI. Diagnosis and management of cracked tooth by quantitative light-induced fluorescence technology. Photodiagnosis Photodyn Ther. 2019; 26: 324-326. doi: 10.1016/j.pdpdt.2019.04.025.