
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 5
Prevalence and progression of interstitial lung abnormalities in the general population: A longitudinal study
Lei Sun1†; Guangshu Shen2†; Ruyi Zou3; Weihong Zhou4; Qi Zhao3; Jingzhi Tong3; Liyun Miao1,3*; Kefeng Zhou5*
1Yancheng Branch of Nanjing Drum Tower Hospital, Yancheng, No.135 Kaifang Avenue, 224003, China.
2Department of Radiology, Nanjing Drum Tower Hospital Clinical College of Nanjing Medical University, No.321 Zhongshan Road, Nanjing, 210008, China.
3Department of Respiratory and Critical Care Medicine, Nanjing Drum Tower Hospital, the Affiliated Hospital of Nanjing University Medical School, No.321 Zhongshan Road, Nanjing, 210008, China.
4Department of Health Management Centre, Nanjing Drum Tower Hospital Affiliated to Nanjing University Medical School, No.321 Zhongshan Road, Nanjing, 210008, China.
5Department of Radiology, Nanjing Drum Tower Hospital, the Affiliated Hospital of Nanjing University Medical School, No.321 Zhongshan Road.
†Equal Contribution.
*Corresponding Author : Liyun Miao
Nanjing Drum Tower Hospital, No.321 Zhongshan
Road, Nanjing, 210008, China.
Email: liyunmiao462@163.com
Received : Mar 13, 2024
Accepted : Apr 17, 2024
Published : Apr 24, 2024
Archived : www.jcimcr.org
Copyright : © Miao L (2024).
Abstract
Background: Interstitial lung abnormalities (ILAs) are increasingly recognized on chest Computed tomography (CT) scans. There has been no prior evaluation of ILA prevalence and progression in the general population in China. Therefore, we conduct a longitudinal study to investigate the prevalence and progression of ILA in the general population in China, and to provide a reference for the management of ILA and further researches.
Method: CT images of 10820 participants who underwent chest CT scans at the Health Management Centre of Nanjing Drum Tower Hospital in 2017 were evaluated. The temporal change of the ILA was evaluated at 2-5 years follow up. Logistic regression models were used to determine factors associated with development and progression of ILA.
Results: Interstitial lung abnormalities were noted in 715(6.6%) participants. Of whom, 83 participants were assessed as false or non-ILA changes, mainly due to gravity effect or inadequate inspiration. Age was associated with the prevalence of ILA. Of 497 participates with sequential chest CT scans during the five-year follow-up period, 165(33.2%) subjects had progressed ILA and 287(57.7%) patients had stable ILA, and 45(9.1%) patients had improved ILA. Compared to female, ILA in male are more likely to progress.
Conclusions: ILA is relatively common in the general population and the presence of ILA is associated with increasing age. ILA progression is common and more common in male. Early management may be the best option for these patients. Further studies are needed to validate management strategies and treatment benefits.
Keywords: Interstitial lung abnormalities (ILA); Prevalence; Progression; Management; Imaging pattern.
Citation: Sun L, Shen G, Zou R, Zhou W, Zhao Q, et al. Prevalence and progression of interstitial lung abnormalities in the general population: A longitudinal study. J Clin Images Med Case Rep. 2024; 5(4): 3007.
Introduction
ILA has been described since decades ago, initially discovered in clinically unaffected members of families with an idiopathic pulmonary fibrosis or smokers [1,3]. With the widespread use of high-resolution computed tomography (HRCT) in clinical setting, especially lung cancer screening, ILA has become more widely detected in asymptomatic and undiagnosed individuals. ILA has been shown to be associated with respiratory symptoms, functional impairment, risk of disease progression and increased all-cause mortality, possibly an early state of interstitial lung disease (ILD) [3,8]. In recent years, as studies on ILA have increased, the 2020 Fleischner Society position paper standardized the definition of ILA based on the available published literature and the Multidisciplinary consensus [9]: ILA is an incidental identification of non-dependent abnormalities involving at least 5% of a lung zone, including ground-glass or reticular abnormalities, lung distortion, traction bronchiectasis, honeycombing, and non-emphysematous cysts. Moreover, the position paper addressed the predisposing risk factors; clinical outcomes; initial evaluation, monitoring and management of ILA and future research needs, which may increase the awareness of ILA identification and help primary care providers and pulmonary specialists to evaluate and treat subjects with incidentally discovered ILA.
However, our understanding of ILAs is still minimal, currently epidemiological data are mainly derived from several large early cohort studies [6,7], with more longitudinal studies are lacking. It was also proposed in the Fleischner position paper that the preliminary radiological criteria for ILA presented in the paper required evaluation to determine their reproducibility and application to clinical practice. There has been no prior evaluation of ILA prevalence and progression in the general population in China. Therefore, we conducted a longitudinal study to explore the prevalence of ILA in the general population and the progression rate of ILA over a five-year follow-up period, and hope to provide more statistical evidence for development and progression of ILA in clinical practice and make recommendations for further research.
Methods
Study population
We retrospectively reviewed the CT images of 10820 participants who underwent low-dose CT at the Health Management Centre of Nanjing Drum Tower Hospital from January 2017 to December 2017. Subjects who were reported interstitial abnormalities and had serial chest CT scan from 2018 to 2022 (two to five years follow-up period) were selected, which were used for ILA progression evaluation. The Neusoft (v5.5.0 Diagnostic imaging systems) were used to view the image information. The study was approved by Medical Ethics Committee of Nanjing Drum Tower Hospital Affiliated to Nanjing University School of Medicine (NO.2022-046-01) and individual consent for this retrospective analysis was waived.
CT scan
In this study, participants underwent CT chest without contrast (Definition Sensation 64; Siemens Medical Solutions, Forchheim, Germany). Images were obtained after full inspiration and hold in the supine position.
ILA evaluation
To ensure the accuracy of the evaluation, the images of these participants were initially evaluated by radiologists (two radiologists, one reported and one reviewed) and the CT images were re-evaluated by experienced pulmonologists (physicians from respiratory department), who were blind to prior radiologic interpretations of other readers and all subjects-specific information. Inconsistencies between the evaluation were resolved by common discussions. ILA evaluation was objectively based on the radiological imaging and referenced to the fleischner paper criteria for ILA.
Statistical analysis
The demographic data between participants with and without ILA were compared by using an unpaired t test (for normal distribution data) or Mann-Whitney test (for non-normal distribution data). Chi-square test was performed to test for any differences in the distribution of categorical variables among two groups. Logistic regression models were used to assess the associations between ILA and demographic data (age, sex); the corresponding odds ratios with 95% confidence interval (CI) were computed. A two-sided p value less than 0.05 was considered to be statistically significant. All analyses were performed with statistical software (SPSS 25.0, Chicago) and GraphPad Prism9.0.0.
Results
Baseline characteristics and interstitial lung abnormalities
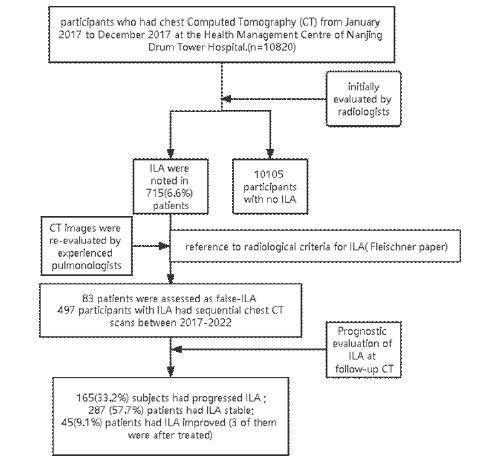
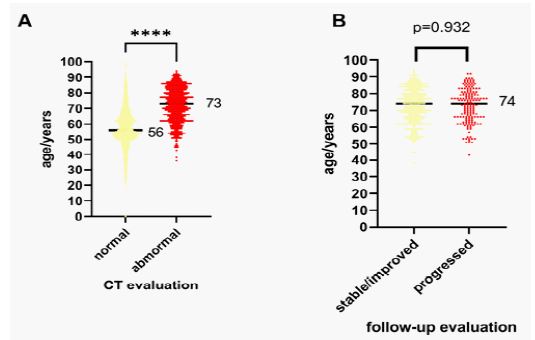
We reviewed images on a total of 10,820 subjects who had chest Computed Tomography (CT) from January 2017 to December 2017 at the Health Management Centre of Nanjing Drum Tower Hospital. The flowchart of participant inclusion and evaluation in this study is shown in figure 1. Table 1 shows the baseline characteristics of the participants. The participants consisted of 6833(63.2%) men and 3987(36.8%) women, with a mean age of 58.2±12.6 years (median: 57years, range: 19–100 years). ILA were noted in 715(6.6%) patients. As compared to participants had normal CT images, those reported to be ILA were more likely to be older (median age: 73 vs 56 years old, p< 0.0001) (Figure 2). Increasing age was associated with ILA prevalence (OR: 1.103, 95%CI: 1.095-1.111, P< 0.0001) (Table 2).
Prognostic evaluation of ILA at follow-up CT
The detection rate of ILA in the baseline radiologic reports were 6.6%(715/10820). After re-evaluation by experienced respiratory physicians reference to the fleischner’s ILA criteria, 83 patients were assessed as non-ILA (“false-positive” or “not-real”) changes, mainly due to gravity effect or insufficient inspiration. 497 patients underwent at least two serial imaging evaluations during the five-year follow-up period were included in prognostic evaluation. Of the 497 participants with sequential chest CT scans, 165(33.2%) subjects had progressed ILA and 287 (57.7%) patients had ILA stable state, and 45(9.1%) patients had ILA improved (3 of them were after treated) (Table 3). Logistic regression showed that compared to male, female are a protective factors of ILA progression (OR:0.614, 95%CI:0.409-0.923, p=0,019) (Table 4).
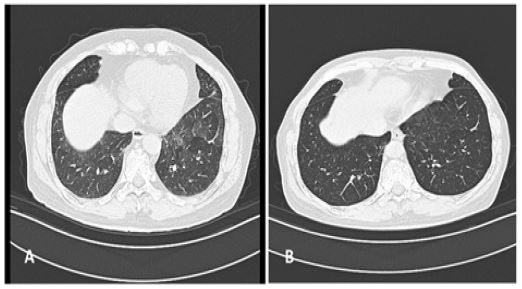
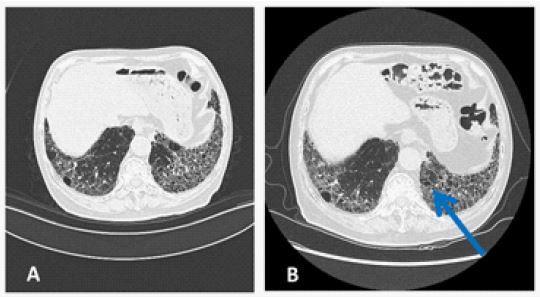
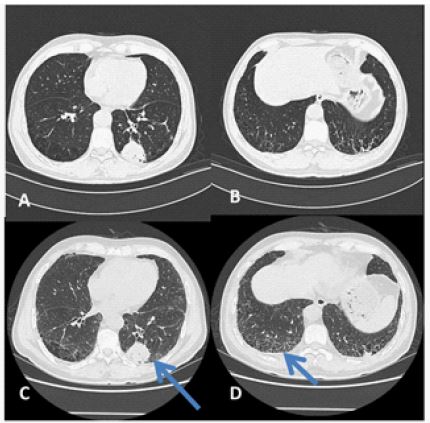
Representative CT images
Notably, we found that some patients have “false” ILAs, which were caused by transient factors such as incomplete inspiration during examination and gravity fall effect, infection, aspiration, and drugs. We need to carefully identify the radiological abnormalities (Figure 3). Some patients’ ILA progressed slowly during our 2-5year follow-up (Figure 4), and some patients’ ILA progressed rapidly during the treatment of lung cancer (Figure 5). We showed some CT images, hoping to provide some references to clinical physicians about the image patterns of ILA.
Table 1: Characteristics of 10820 participates with normal/abnormal interstitial lung images.
| Total n=10820 | Normal n=10105 | Abnormal n=715 | P | |
|---|---|---|---|---|
| Age* | 57(58.2±12.6) | 56(57.2±12.1) | 73(72.0±11.2) | <0.0001 |
| Age-layer | <0.0001 | |||
| <=40 | 808 | 806(8.0%) | 2(0.3%) | |
| 41-50 | 1617 | 1605(15.9%) | 12(1.7%) | |
| 51-60 | 4005 | 3902(38.6%) | 103(14.4%) | |
| 61-70 | 2678 | 2476(24.5%) | 202()28.3% | |
| 71-80 | 1108 | 902(8.9%) | 206(28.8%) | |
| >80 | 604 | 414(4.1%) | 190(26.6%) | |
| sex | 0.781 | |||
| male | 6833 | 6387(63.1%) | 455(63.6%) | |
| female | 3987 | 3727(36.9%) | 260(36.4%) |
*: age was shown as the median (mean±SD). Categorical variables (sex, age-layer) were analyzed by chi-square test.
Table 2: logistics regression of factors associated with ILA detected at baseline CT.
| factor | Model 1 | groups | Model 2 | ||||
|---|---|---|---|---|---|---|---|
| OR | 95%CI | P | OR | 95%CI | P | ||
| Sex(f/m) | 0.925 | 0.782-1.094 | 0.360 | (f/m) | 0.903 | (0.764-1.067) | 0.230 |
| age | 1.103 | 1.095-1.111 | 0.000 | vs.<=40 years | |||
| 41-50 | 3.014 | (0.673-13.501) | 0.149 | ||||
| 51-60 | 10.494 | (2.584-42.621) | 0.001 | ||||
| 61-70 | 32.722 | (8.109-132.036) | 0.000 | ||||
| 71-80 | 91.712 | (22.709-370.376) | 0.000 | ||||
| >80 | 184.564 | (45.594-747.114) | 0.000 | ||||
f/m: female vs male; model 1 logistic regression included factors: sex and age(years), model 2: logistic regression when age were categorical variables.
Table 3: Characteristics of 497 participates with ILA at 2-5year Follow-up.
| Total n=497 | Stable/improved n=10105 | progressed n=715 | P | |
|---|---|---|---|---|
| Age* | 74(72.6±10.4) | 74(72.6±10.6) | 74(72.6±10.2) | 0.77 |
| Age-layer | 0.858 | |||
| <=40 | 1 | 1(0.3%) | 0(0.0%) | |
| 41-50 | 4 | 3(0.9%) | 1 (0.6%) | |
| 51-60 | 57 | 41(12.3%) | 16(9.7%) | |
| 61-70 | 145 | 94(28.3%) | 51(30.9%) | |
| 71-80 | 165 | 109(32.8%) | 56(33.9%) | |
| >80 | 125 | 84(25.3%) | 41 (24.8%) | |
| sex | 0.019 | |||
| male | 323 | 204(61.4%) | 119(72.1%) | |
| female | 174 | 174(38.6%) | 46(27.9%) |
*: age was shown as the median (mean±SD). Categorical variables (sex, age-layer) were analyzed by chi-square test.
Table 4: logistics regression of factors associated with the progression of ILA.
| factors | OR |
95%CI |
P |
|
|---|---|---|---|---|
| lower | upper | |||
| Sex(f/m) | 0.614 | 0.409 | 0.923 | 0.019 |
| age | 1.002 | 0.984 | 1.02 | 0.863 |
f/m: female vs male.
Discussion
This study was a longitudinal visual assessment of chest CT images for the purposes of characterizing ILA prevalence and progression. One of significance of this study was to conduct a robust evaluation about the preliminary radiological criteria for ILAs presented in Fleischner Position Paper, to determine their reproducibility and application to clinical practice. For the first time, this study provided some descriptive statistics on the prevalence and progression rate of ILA in the general population in China. ILA progression was relatively common, which may be the point that clinical physicians should pay more attention to.
The prevalence of ILA in the general population in our study (6.6%; 715 of 10820 participants) was similar with prior reports. In Framingham Heart Study (FHS), a longitudinal study originally designed to investigate risk factors for cardiovascular disease in the general population, ILA was prevalent on 3% of the initial scans and the progression rate of ILA was 43% over approximately 5 years of follow-up time [7]. In a National Lung Screening Trial population, the prevalence of ILA was 9.7% (86 of 884 participants) [4].
Participants with ILA were significantly older in our study, which is similar to previous reports. The main known risk factors for ILA are advanced age, smoking, and familial history of ILD [10,13]. In addition, researchers have suggested that increased copies of the MUC5B promoter, occupational exposure (including steam, dust and fumes), air pollution, nitrogen oxide exposure, and arsenic content in edible rice may all be related to the occurrence of ILA [14,18]. Notably, there were “false” and transient ILA in our research, which were caused by factors such as incomplete inspiration during examination and gravity fall effect, infection, aspiration, and drugs [3,13]. we need to carefully identify the radiological abnormalities, some of them may be “real” ILA, with a danger to progression, such patients need to be paid close attention and management; False, transient lung shadows due to position, infection, aspiration, etc., may usually resolve automatically when the cause is relieved.
In our study, participants with ILA had lung cancer rapidly progressing or worsening to death. Studies have shown an association between ILA and cancer treatment toxicity and mortality [19]. Studies suggest that ILA may increase lung injury risk caused by cancer therapies (e.g., surgery, radiation therapy, and drugs). This includes the development of associated ILD after immune checkpoint inhibitor (ICI) therapy (ICI-ILD) [20], acute respiratory distress syndrome (ARDS) after pulmonary surgery [21]. Extensive radiation pneumonitis (RP) is probably the most common and fatal complication in patients with pre-existing ILA treated with stereotactic body radiotherapy [22,27].
Despite the increasing attention to ILA in research Settings, it may be easier to ignore these interstitial lung changes in an actual clinical setting, mainly because they are often found incidentally and are usually asymptomatic. The clinical management strategy for ILA outlined in the fleischner position paper may help improve this situation and help clinicians manage these abnormalities. Our findings demonstrate that ILA is widespread in the general population and carries a risk of progression, calling for clinicians to pay more attention to this inconspicuous abnormality in clinical practice.
Our study has some limitations. First, as a single-center study, there may be some regional bias in the physical examination population. Second, the basic information we included was not comprehensive, and multivariable models were not adjusted for potential covariates (including body mass index, smoking status, pack-years of smoking, etc.). Third, all assessments were assessed by physicians based on CT images, with little understanding of the patient’s diagnosis and treatment process. At the same time, the presence or pattern of parenchymal abnormalities could not be demonstrated histologically, so the physiological correlation of imaging abnormalities could not be matched. Considering the deficiency of our study and current situation of ILA research, we put forward some ideas for further research.
Quantitative evaluation of ILA may be one of the further research directions, which may be applied to large-scale studies or mass screening. High-attenuation areas (HAA) is defined as the percentage of lung volume with CT attenuation value between -600 and -250 HU[28]. Nowadays, the clinical significance of HAA remains unclear, and assessment in individual patients is limited [9]. The feasibility of optimizing thresholds of HAA for large-scale ILA clinical identification and risk assessment need to be further explored.
Overall considering the current research status there are still some doubts about ILA: the appropriate follow-up cycle of ILA patients found by chance, the specific relationship between different imaging characteristics and the risk of progression, the biomarkers that predict disease progression effectively, and the effective criteria for progress risk assessment are still unclear. More longitudinal studies of ILA are needed to provide more statistical evidence and to investigate reasonable management and treatment strategies. Our study revealed that the prevalence and progression of ILA is common in Chinese populations, improving physicians’ attention in clinical practice and providing a reference for subsequent management.
Conclusion
Our study demonstrates that ILA is relatively common in the general population and is associated with advanced age. ILA progression is relatively common over a 5-year period. Early management and multidisciplinary discussions may be better managed for these people.
Declarations
The study was approved by Medical Ethics Committee of Nanjing Drum Tower Hospital Affiliated to Nanjing University School of Medicine (NO.2022-046-01).
Acknowledgements: We thank all the staffs of Health Management Centre who provide services to all the patients.
Conflict of Interest: The authors have no conflicts of interest to declare.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
- Bitterman PB, Rennard SI, Keogh BA, Wewers MD, Adelberg S, Crystal RG. Familial Idiopathic Pulmonary Fibrosis. Evidence of Lung Inflammation in Unaffected Family Members. The New England journal of medicine. 1986; 314(21): 1343-7. Epub 1986/05/22. doi: 10.1056/nejm198605223142103.
- Lederer DJ, Enright PL, Kawut SM, Hoffman EA, Hunninghake G, van Beek EJ, et al. Cigarette Smoking Is Associated with Subclinical Parenchymal Lung Disease: The Multi-Ethnic Study of Atherosclerosis (Mesa)-Lung Study. Am J Respir Crit Care Med. 2009; 180(5): 407-14. Epub 2009/06/23. doi: 10.1164/rccm.200812-1966OC.
- Washko GR, Hunninghake GM, Fernandez IE, Nishino M, Okajima Y, Yamashiro T, et al. Lung Volumes and Emphysema in Smokers with Interstitial Lung Abnormalities. The New England journal of medicine. 2011; 364(10): 897-906. Epub 2011/03/11. doi: 10.1056/NEJMoa1007285.
- Jin GY, Lynch D, Chawla A, Garg K, Tammemagi MC, Sahin H, et al. Interstitial Lung Abnormalities in a Ct Lung Cancer Screening Population: Prevalence and Progression Rate. Radiology. 2013; 268(2): 563-71. Epub 2013/03/21. doi: 10.1148/radiol.13120816.
- Cordier JF, Cottin V. Neglected Evidence in Idiopathic Pulmonary Fibrosis: From History to Earlier Diagnosis. Eur Respir J. 2013; 42(4): 916-23. Epub 2013/04/20. doi: 10.1183/09031936.00027913.
- Putman RK, Hatabu H, Araki T, Gudmundsson G, Gao W, Nishino M, et al. Association between Interstitial Lung Abnormalities and All-Cause Mortality. Jama. 2016; 315(7): 672-81. Epub 2016/02/18. doi: 10.1001/jama.2016.0518.
- Araki T, Putman RK, Hatabu H, Gao W, Dupuis J, Latourelle JC, et al. Development and Progression of Interstitial Lung Abnormalities in the Framingham Heart Study. Am J Respir Crit Care Med. 2016; 194(12): 1514-22. Epub 2016/06/18. doi: 10.1164/rccm.201512-2523OC.
- Doyle TJ, Hunninghake GM, Rosas IO. Subclinical Interstitial Lung Disease: Why You Should Care. Am J Respir Crit Care Med. 2012; 185(11): 1147-53. Epub 2012/03/01. doi: 10.1164/rccm.201108-1420PP.
- Hatabu H, Hunninghake GM, Richeldi L, Brown KK, Wells AU, Remy-Jardin M, et al. Interstitial Lung Abnormalities Detected Incidentally on Ct: A Position Paper from the Fleischner Society. The Lancet Respiratory medicine. 2020; 8(7): 726-37. Epub 2020/07/11. doi: 10.1016/s2213-2600(20)30168-5.
- King TE, Jr. Smoking and Subclinical Interstitial Lung Disease. The New England journal of medicine. 2011; 364(10): 968-70. Epub 2011/03/11. doi: 10.1056/NEJMe1013966.
- Salisbury ML, Hewlett JC, Ding G, Markin CR, Douglas K, Mason W, et al. Development and Progression of Radiologic Abnormalities in Individuals at Risk for Familial Interstitial Lung Disease. Am J Respir Crit Care Med. 2020; 201(10): 1230-9. Epub 2020/02/06. doi: 10.1164/rccm.201909-1834OC.
- Hunninghake GM, Quesada-Arias LD, Carmichael NE, Martinez Manzano JM, Poli De Frías S, Baumgartner MA, et al. Interstitial Lung Disease in Relatives of Patients with Pulmonary Fibrosis. Am J Respir Crit Care Med. 2020; 201(10): 1240-8. Epub 2020/02/06. doi: 10.1164/rccm.201908-1571OC.
- Washko GR, Lynch DA, Matsuoka S, Ross JC, Umeoka S, Diaz A, et al. Identification of Early Interstitial Lung Disease in Smokers from the Copdgene Study. Academic radiology. 2010; 17(1): 48-53. Epub 2009/09/29. doi: 10.1016/j.acra.2009.07.016.
- Sack CS, Doney BC, Podolanczuk AJ, Hooper LG, Seixas NS, Hoffman EA, et al. Occupational Exposures and Subclinical Interstitial Lung Disease. The Mesa (Multi-Ethnic Study of Atherosclerosis) Air and Lung Studies. Am J Respir Crit Care Med. 2017; 196(8): 1031-9. Epub 2017/07/29. doi: 10.1164/rccm.201612-2431OC.
- Sack C, Vedal S, Sheppard L, Raghu G, Barr RG, Podolanczuk A, et al. Air Pollution and Subclinical Interstitial Lung Disease: The Multi-Ethnic Study of Atherosclerosis (Mesa) Air-Lung Study. Eur Respir J. 2017; 50(6). Epub 2017/12/09. doi: 10.1183/13993003.00559-2017.
- Manichaikul A, Wang XQ, Sun L, Dupuis J, Borczuk AC, Nguyen JN, et al. Genome-Wide Association Study of Subclinical Interstitial Lung Disease in Mesa. Respir Res. 2017; 18(1): 97. Epub 2017/05/20. doi: 10.1186/s12931-017-0581-2.
- Sanchez TR, Oelsner EC, Lederer DJ, Lo Cascio CM, Jones MR, Grau-Perez M, et al. Rice Consumption and Subclinical Lung Disease in Us Adults: Observational Evidence from the Multi-Ethnic Study of Atherosclerosis. American journal of epidemiology. 2019; 188(9): 1655-65. Epub 2019/05/31. doi: 10.1093/aje/kwz137.
- Ortiz-Quintero B, Buendía-Roldán I, Ramírez-Salazar EG, Balderas-Martínez YI, Ramírez-Rodríguez SL, Martínez-Espinosa K, et al. Circulating Microrna Signature Associated to Interstitial Lung Abnormalities in Respiratory Asymptomatic Subjects. 2020; 9(6). Epub 2020/07/02. doi: 10.3390/cells9061556.
- Axelsson GT, Putman RK, Aspelund T, Gudmundsson EF, Hida T, Araki T, et al. The Associations of Interstitial Lung Abnormalities with Cancer Diagnoses and Mortality. Eur Respir J. 2020; 56(6). Epub 2020/07/11. doi: 10.1183/13993003.02154-2019.
- Nakanishi Y, Masuda T, Yamaguchi K, Sakamoto S, Horimasu Y, Nakashima T, et al. Pre-Existing Interstitial Lung Abnormalities Are Risk Factors for Immune Checkpoint Inhibitor-Induced Interstitial Lung Disease in Non-Small Cell Lung Cancer. Respir Investig. 2019; 57(5): 451-9. Epub 2019/06/30. doi: 10.1016/j.resinv.2019.05.002.
- Saito H, Minamiya Y, Nanjo H, Ito M, Ono T, Motoyama S, et al. Pathological Finding of Subclinical Interstitial Pneumonia as a Predictor of Postoperative Acute Respiratory Distress Syndrome after Pulmonary Resection. European journal of cardio-thoracic surgery: official journal of the European Association for Cardio-thoracic Surgery. 2011; 39(2): 190-4. Epub 2010/07/06. doi: 10.1016/j.ejcts.2010.05.017.
- Yamaguchi S, Ohguri T, Matsuki Y, Yahara K, Oki H, Imada H, et al. Radiotherapy for Thoracic Tumors: Association between Subclinical Interstitial Lung Disease and Fatal Radiation Pneumonitis. International journal of clinical oncology. 2015; 20(1): 45-52. Epub 2014/03/13. doi: 10.1007/s10147-014-0679-1.
- Yamaguchi S, Ohguri T, Ide S, Aoki T, Imada H, Yahara K, et al. Stereotactic Body Radiotherapy for Lung Tumors in Patients with Subclinical Interstitial Lung Disease: The Potential Risk of Extensive Radiation Pneumonitis. Lung cancer (Amsterdam, Netherlands). 2013; 82(2): 260-5. Epub 2013/09/24. doi: 10.1016/j.lungcan.2013.08.024.
- Takeda A, Sanuki N, Enomoto T, Kunieda E. Subclinical Interstitial Lung Disease: Is It a Risk Factor for Fatal Radiation Pneumonitis Following Stereotactic Body Radiotherapy? Lung cancer (Amsterdam, Netherlands). 2014; 83(1): 112. Epub 2013/11/10. doi: 10.1016/j.lungcan.2013.10.009.
- Niska JR, Schild SE, Rule WG, Daniels TB, Jett JR. Fatal Radiation Pneumonitis in Patients with Subclinical Interstitial Lung Disease. Clinical lung cancer. 2018; 19(4): 417-e20. Epub 2018/03/13. doi: 10.1016/j.cllc.2018.02.003.
- Li F, Liu H, Wu H, Liang S, Xu Y. Risk Factors for Radiation Pneumonitis in Lung Cancer Patients with Subclinical Interstitial Lung Disease after Thoracic Radiation Therapy. Radiation oncology (London, England). 2021; 16(1): 70. Epub 2021/04/15. doi: 10.1186/s13014-021-01798-2.
- Liu Y, Zhu Y, Wu R, Hu M, Zhang L, Lin Q, et al. Stereotactic Body Radiotherapy for early stage Non-Small Cell Lung Cancer in Patients with Subclinical Interstitial Lung Disease. Translational lung cancer research. 2020; 9(6): 2328-36. Epub 2021/01/26. doi: 10.21037/tlcr-20-1050.
- Podolanczuk AJ, Oelsner EC, Barr RG, Hoffman EA, Armstrong HF, Austin JH, et al. High Attenuation Areas on Chest Computed Tomography in Community-Dwelling Adults: The Mesa Study. Eur Respir J. 2016; 48(5): 1442-52. Epub 2016/11/02. doi: 10.1183/13993003.00129-2016.