
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Listeria pericarditis as a paraneoplastic presentation
Adi Hertz1*; Yehuda Shoenfeld3,4; Howard Amital1,2,3
1Department of Medicine ‘B’, Sheba Medical Center, Tel-Hashomer, Israel.
2Tel-Aviv Medical School, Tel Aviv University, Tel Aviv, Israel.
3Zabludowicz Center for Autoimmune Diseases, Sheba Medical Center, Israel.
4Reichman University, Herzliya, Israel.
*Corresponding Author : Adi Hertz
Department of Medicine ‘B’, Sheba Medical Center, Tel-Hashomer, Israel.
Email: adi.hertzy@gmail.com
Received : Mar 28, 2024
Accepted : Apr 18, 2024
Published : Apr 25, 2024
Archived : www.jcimcr.org
Copyright : © Hertz A (2024).
Abstract
Introduction: Pericarditis is a common cause of chest pain. It has many etiologies, which are classified into infectious and non-infectious causes. The majority of cases follow a benign course.
Case summary: A 66-year-old female presented with pleuritic chest pain following a febrile illness. She was diagnosed with acute idiopathic pericarditis, and standard treatment was initiated. In the following weeks she returned to the hospital multiple times due to unresolved symptoms. Pericardiocentesis was done and cultures from the fluid grew Listeria monocytogenes. CT scan uncovered metastatic pancreatic malignancy. Rapid symptom resolution was observed following the initiation of appropriate antibiotic treatment.
Discussion: While most cases of pericarditis follow a benign course, the presence of high-risk features warrants a thorough investigation. In cases resistant to standard treatment, less common causes of pericarditis should be sought.
Keywords: Refractory pericarditis; Incessant pericarditis; Listeria pericarditis; Paraneoplastic; Pancreatic adenocarcinoma.
Citation: Hertz A, Shoenfeld Y, Amital H. Listeria pericarditis as a paraneoplastic presentation. J Clin Images Med Case Rep. 2024; 5(4): 3011.
Introduction
Pericarditis accounts for 0.1% of all hospital admissions and 5% of emergency room admissions for chest pain. The majority of cases follow a benign course. Pericarditis has many etiologies, which are classified into infectious (two-thirds of cases) and non-infectious causes (one-third of cases). In developed countries, viral pericarditis is the most common etiology, while Tuberculosis (TB) predominates in developing countries. Other important etiologies include malignancy and autoimmune diseases [1]. We would like to present a case of refractory pericarditis, caused by Listeria monocytogenes, an uncommon infectious agent, which revealed an underlying malignancy, likely contributing to the unusual presentation through a paraneoplastic mechanism.
Case presentation
A 66-year-old female initially presented to another hospital with a five-day history of retrosternal pleuritic chest pain, which occurred two days after a febrile illness. Her medical history includes a small chronic pericardial effusion diagnosed eight years ago, which is monitored via sonographic follow-up without further evaluation. Upon examination, her vital signs were mostly within normal ranges, except for sinus tachycardia of 114 beats per minute. Laboratory tests showed elevated inflammatory markers with a CRP level of 15 mg/l (upper normal limit 5 mg/l), normal leukocyte count, and negative cardiac markers. Echocardiography revealed a small pericardial effusion, leading to a diagnosis of acute pericarditis. She was discharged with Ibuprofen and colchicine therapy.
Five days later, she returned to the same hospital due to ongoing chest pain, now accompanied by palpitations. Laboratory tests showed increased inflammatory markers with a CRP level of 90 mg/l, leukocytosis of 13 K/μL (normal range 4-10.8 K/μL), and slightly elevated Troponin levels at 33 ng/L (upper normal limit 12 ng/L). The results of the auto-immunity panel came back negative. An ECG revealed atrial fibrillation/flutter, with no hemodynamic compromise or pulmonary edema on chest X-ray. The pericardial effusion remained small on echocardiography. She was discharged with Prednisone 30 mg and colchicine therapy, with instructions for gradual tapering.
Three days later, she presented to the Emergency Room at our medical facility, experiencing persistent chest pain and palpitations despite being on a 30 mg prednisone therapy and was admitted in the Cardiology department. Laboratory tests showed further elevation in inflammatory markers, with a CRP level of 83 mg/l, leukocytosis of 15 K/μL, and increased Troponin levels up to 360 ng/L. This time, ECG revealed Atrioventricular Nodal Reentrant Tachycardia (AVNRT) with a heart rate of 160 bpm, which resolved following an Adenosine challenge. The pericardial effusion remained unchanged in quantity. She was admitted to the cardiology department, where she underwent ablation of the slow pathway, and prednisone therapy was increased to 40 mg daily. She was discharged with 40 mg of Prednisone and colchicine, along with instructions for gradual tapering.
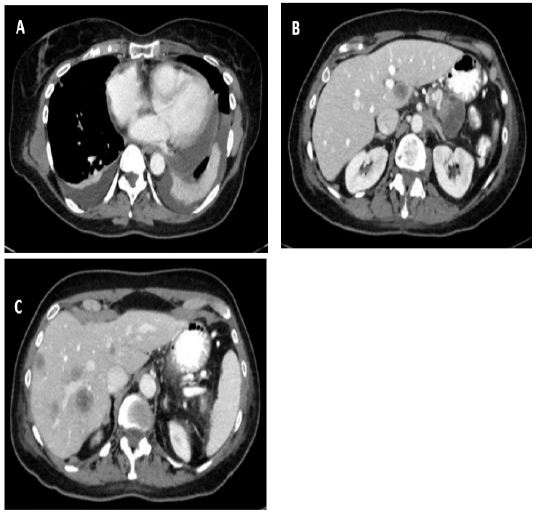
B: Solid-cystic pancreatic mass with septations located in the tail of the pancreas, measuring 4 cm in diameter.
C: Multiple hypodense hepatic lesions compatible with metastatic spread.
Table 1: High-risk features associated with poor prognosis of pericarditis.
| Major | Minor |
|---|---|
| 1. Fever > 38 2. Subacute course 3. Large pericardial effusion 4. Cardiac tamponade 5. Lack of response to aspirin or NSAIDs (after 1 week of therapy) |
1. Myopericarditis 2. Immunosupression 3. Trauma 4. Oral anticoagulant therapy |
Twelve days later, she was readmitted to the cardiology department with the same complaints and new symptoms of exertional dyspnea and bilateral lower extremity edema, while on 40 mg of prednisone. Laboratory tests revealed a significant increase in inflammatory markers, with a CRP level of 241 mg/l, leukocytosis of 20 K/μL, and elevated Troponin levels of 256 ng/L. Echocardiography showed an increase in the pericardial effusion, now classified as moderate. She was diagnosed with incessant pericarditis, defined as pericarditis lasting more than 4 weeks and up to 3 months without remission. She underwent pericardiocentesis, with 350 ml of fluid removed, and high-dose prednisone therapy of 60 mg was initiated as a bridge to Anakinra (Anti-IL1). She was transferred to the internal medicine department for further evaluation and treatment. Shortly after her arrival, the pericardial fluid culture returned positive for Listeria monocytogenes, with blood cultures also positive for Listeria. Antibiotic treatment with Parenteral Ampicillin and Gentamycin was initiated alongside corticosteroid tapering. Prompt clinical and laboratory improvements were observed, with CRP decreasing from 117 mg/l to 30 mg/l. As part of her evaluation, she underwent a chest, abdomen, and pelvis CT, which revealed pericardial thickening and a pericardial effusion, along with an unexpected finding of a solid-cystic mass in the pancreas tail, measuring 4 cm in diameter, and multiple hypodense lesions in the liver, suggestive of metastatic spread (Figure 1). A biopsy from the liver mass indicated a primary pancreaticobiliary origin, leading to the diagnosis of stage 4 pancreatic adenocarcinoma.
Three weeks later, she was readmitted to our ward due to recurring chest pain while tapering steroids from 30 mg to 25 mg, despite receiving appropriate antibiotic treatment. An increase in prednisone dosage immediately alleviated her symptoms, and she was discharged with instructions for a more gradual tapering regimen.
Discussion
This is a case of Listeria pericarditis in a patient with an underlying malignancy, likely leading to the immunosuppressed state facilitating Listeria infection. Furthermore, the malignancy likely contributed to the development of pericarditis through auto-inflammation driven by a paraneoplastic mechanism. This was evidenced during the last hospitalization when the patient.
Experienced recurrent symptoms despite antibiotic treatment, and resolution occurred promptly following an increase in prednisone dosage. A Danish cohort study found that pericarditis may be a marker of occult malignancy. Cancer-related pericarditis may occur through various mechanisms, such as direct infiltration by malignant cancer cells from adjacent structures, pericardial hemorrhage, hematogenous dissemination and also as a paraneoplastic syndrome [2].
Listeria monocytogenes is an exceptionally rare causative agent of pericarditis. A search on Medline revealed 13 previous cases of Listeria pericarditis, with a high mortality rate (7 out of 13 patients, with 2 patients dying from causes unrelated to Listeria pericarditis).
Most patients exhibited an underlying immunocompromised state, although one patient, who had a favorable outcome, did not. The most prevalent underlying comorbidities were cirrhosis and malignancy. Other risk factors included renal failure necessitating hemodialysis, rheumatoid arthritis treated with low-dose prednisone, HIV infection with a low CD4 count, multiple myeloma, giant cell arteritis on prednisone therapy, and recent delivery in the postpartum period [3-5].
The aforementioned case illustrates key considerations in the evaluation and management of pericarditis and the importance of ruling out bacterial pericarditis, neoplastic pericarditis, and pericarditis associated with systemic diseases (e.g., autoimmune diseases) to allow a directed therapy. The European Society of Cardiology (ESC) Guidelines propose an algorithm by which admission and a comprehensive etiological investigation are recommended in the presence of high-risk features (Table 1) or when a specific etiology is suspected. High-risk features are associated with increased risk of complication, including tamponade, recurrences and constriction [1]. Throughout her hospitalizations, the patient exhibited several high-risk features, including a subacute course, lack of response to NSAIDs, myocardial involvement (manifested by arrhythmias and elevated troponin levels), and immunosuppression.
Another crucial aspect, is when should pericardiocentesis be carried out. Pericardiocentesis is not essential for the diagnosis of the underlying cause of pericardial effusion. Indications for this diagnostic and sometimes therapeutic procedure include cardiac tamponade or for symptomatic moderate to large pericardial effusions not responsive to medical therapy, and for suspicion of unknown bacterial or neoplastic etiology. Purulent bacterial pericarditis is a rare (< 1% of cases) rapidly progressive life-threatening disease with a mortality rate of 40% among treated patients. The cornerstones of treatment include the immediate initiation of empirical intravenous antimicrobial therapy and urgent pericardiocentesis and drainage as part of a source control strategy [6].
Conclusion
In conclusion, while most cases of pericarditis follow a benign course, the presence of high-risk features warrants a thorough investigation. In cases resistant to standard treatment, less common causes of pericarditis should be sought. Bacterial pericarditis, although rare, carries a high risk of mortality. Therefore, it should be ruled out, especially before initiating immunosuppressive therapy.
References
- Adler Yehuda, et al. ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC) Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS). European heart journal. 2015; 36(42): 2921-2964. doi:10.1093/eurheartj/ehv318.
- Søgaard, Kirstine Kobberøe, et al. Pericarditis as a Marker of Occult Cancer and a Prognostic Factor for Cancer Mortality. Circulation. 2017; 136(11) (2017): 996-1006. doi:10.1161/CIRCULATIONAHA.116.024041.
- Findlater, Aidan Reid, et al. Listeria pericarditis in a lymphoma patient: Case report and literature review. Journal of the Association of Medical Microbiology and Infectious Disease Canada = Journal officiel de l’Association pour la microbiologie medicale et l’infectiologie Canada. 2020; 5(3): 182-186. doi:10.3138/jammi-2020-0008.
- Brown Andrew, et al. Listeria myopericarditis associated with right atrial mural thrombus: A case report. European heart journal. Case reports. 2020; 4(4): 1-5. doi:10.1093/ehjcr/ytaa145.
- Ghersin Itai, et al. Listeria Monocytogenes Pericarditis in the Immune Compromised: A Case Report in a Newly Diagnosed Alpha Light Chain Cardiac Amyloidosis Patient. The Israel Medical Association journal: IMAJ. 2019; 21(10): 696-697.
- Pankuweit Sabine, et al. Bacterial pericarditis: diagnosis and management. American journal of cardiovascular drugs: Drugs, devices, and other interventions. 2005; 5(2): 103-12. doi:10.2165/00129784-200505020-00004.