
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Long survivorship after advanced cervical carcinoma diagnosis
Magda Palka-Kotlowska1; Ximena Ribera-Escobar2; Sara Custodio-Cabello1; Vilma Emilia Pacheco-Barcia1; Eduardo Oliveros- Acebes3; Luis Cabezón-Gutierrez1*
1Medical Oncology, Hospital Universitario de Torrejón, Madrid, Spain.
2Student of Medicine, Universidad Francisco Marroquín, Guatemala, Spain.
3Internal Medicine, Hospital Universitario de Torrejón, Madrid, Spain.
*Corresponding Author : Luis Cabezón-Gutiérrez
Medical Oncology, Hospital Universitario de Torrejón, Madrid, Spain.
Email: lcabezon@torrejonsalud.com
Received : Mar 27, 2024
Accepted : Apr 22, 2024
Published : Apr 29, 2024
Archived : www.jcimcr.org
Copyright : © Cabezón-Gutierrez L (2024).
Abstract
Purpose: Patients with advanced cervical cancer have a very poor prognosis. The development of new drugs has led to an increase in the survival of these patients, although the situation can still be improved. In certain cases, despite the poor prognostic factors, the results can be very encouraging.
Case description: We present the case of a 53-year-old patient with multiple sclerosis diagnosed with stage IV cervical carcinoma in June 2020. She received combined radiotherapy and chemotherapy, including carboplatin, paclitaxel, and bevacizumab, followed by maintenance therapy with bevacizumab. She achieved a complete response and after 36 months of maintenance with bevacizumab, she discontinued the drug maintaining the complete response.
Conclusions: We highlight the relevance of therapeutic combination in patients with significant comorbidities such as multiple sclerosis and cervical carcinoma, as well as the importance of continuous follow-up to evaluate the response to treatment.
Keywords: Cervical cancer; Long survivor; Advanced stage; Complete response; Bevacizumab.
Citation: Cabezón-Gutierrez L, Palka-Kotlowska M, Ribera-Escobar X, Custodio-Cabello S, Pacheco-Barcia VE, et al. Long survivorship after advanced cervical carcinoma diagnosis. J Clin Images Med Case Rep. 2024; 5(4): 3015.
Introduction
Cervical cancer is one of the most common gynecological tumors. In advanced stages, the median survival until recently did not reach 18 months, being a sentence for those patients who suffered from it, despite the development and contribution to survival of drugs such as the antiangiogenic bevacizumab or the immune checkpoint inhibitors.
We present the case of a fragile patient, with a history of multiple sclerosis, who despite the diagnosis of advanced cervical cancer has exceptionally surpassed all statistics.
Case presentation
The patient, a 53-year-old Caucasian woman with a history of multiple sclerosis since the age of 19, was diagnosed on 6th June 2020 with stage IV cervical carcinoma, with Positron Emission Tomography (PET) positive balloon-release lung metastasis with lesions of up to 30 mm wide. Her first symptoms were pelvic pain and bleeding.
The cervical biopsy showed an undifferentiated cervical carcinoma, VPH negative, P16, P63, P40 PX 8 negative, estrogen and progesterone receptors, vimentine and CEA focal and weak positivity, and focal positivity for P53. There was not microsatellite instability.
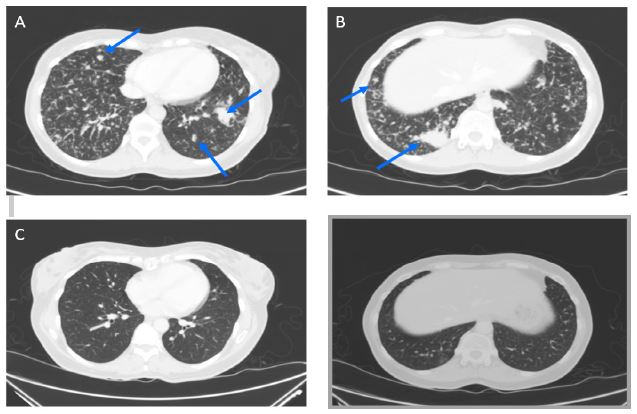
C and D: Thoracic CT scan once complete response was achieved in 22nd October 2020.
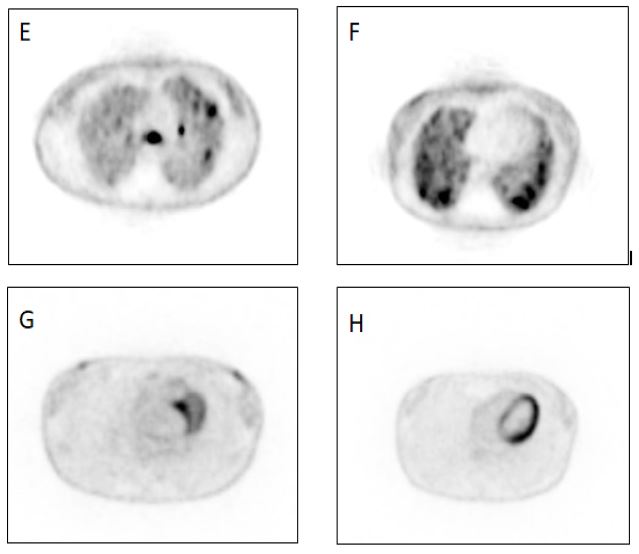
G and H: Thoracic PET with complete response in 27th December 2023.
The lung metastases were not present on previous CT scans (Figure 1), and were not biopsied due to limitations of the pandemic SARS-COV-2.
She was treated with hemostatic and analgesic radiotherapy up to 20 Gy on uterus, cervix, vagina, and adnexa in five sessions between 12th and 17th July 2020, and continued with Carboplatin AUC 5 and Paclitaxel 175 mg/m2 with bevacizumab 15 mg/kg i.v for 6 cycles since 21st July 2020 until 4th December 2020. She followed her treatment with bevacizumab maintenance every three weeks since 28th December 2020.
In the TAC scan performed on 22nd October 2020, a complete response was achieved (Figure 2), but she continued bevacizumab (until progression or relevant toxicity). On 16th November 2023 the treatment was stopped due to grade 2 proteinuria. A complete response was still demonstrated on the PET scan and CT scan performed in November of this year, and she initiated follow-up. In March 2024, she is still in complete response.
Discussion
Cervical cancer is one of the most common gynecological tumors. In developed countries, due to screening programs and vaccination, it is diagnosed at earlier stages and its incidence is decreasing [1]. The most common subtype is squamous cell carcinoma (70% of cases), followed by adenocarcinoma and adenosquamous carcinoma (25% and 5% of cases respectively) [2].
The initial symptom is usually local (vaginal bleeding, pain, or dyspareunia), and it is common to observe a lesion on the cervix during gynecological examination. In advanced cases, patients often do not present florid symptoms, although these may exist depending on the site of metastasis, for example, pain if there are metastatic bone lesions.
The main organs affected by disseminated disease are pelvic and para-aortic lymph nodes (75% and 62% respectively), lung (38%), liver (33%), peritoneum, adrenal glands, intestines, and even the skin [3]. The staging study, if possible, should be performed using PET/CT, as its sensitivity reaches 96% and its specificity 95% [4].
It is important, if possible, to obtain histological confirmation of metastatic disease due to the risk of second synchronous tumors or benign histology in 7% of cases [5]. Patients with oligometastatic advanced-stage disease may benefit from a radical approach [6], but generally, they will be candidates for chemotherapy treatment. In our case, the patient received palliative radiotherapy at the pelvic level and chemotherapy with carboplatin AUC 5, paclitaxel 175 mg/m2, and bevacizumab 15 mg/kg every 3 weeks for 6 cycles, and then maintenance with bevacizumab.
Unfavorable predictive factors include black race, ECOG Performance Status (PS) 1 or 2, pelvic disease, patients pretreated with cisplatin concomitant with radiotherapy, and those who experience disease recurrence within a year after diagnosis [7].
The GOG 240 trial [8] randomized 452 patients with advanced cervical cancer to the arms of cisplatin plus paclitaxel versus paclitaxel plus topotecan with or without bevacizumab in each arm. The cisplatin and paclitaxel arm was superior to the paclitaxel and topotecan arm, and the combination of cisplatin, paclitaxel, and bevacizumab improved on cisplatin and paclitaxel, resulting in progression-free survival of 8.2 versus 6 months (HR 0.68, 95% CI 0.54-0.82) and overall survival of 16.8 versus 13.3 months (HR 0.77, 98% CI 0.62-0.95). The use of carboplatin instead of cisplatin due to its better tolerance and toxicity profile is based on the JCOG 505 study in the Asian population [9]. This study compared the treatment arms of cisplatin 50 mg/m2 + Paclitaxel 135 mg/m2 versus carboplatin AUC 5 and paclitaxel 175 mg/m2 every 3 weeks for 6 cycles in advanced cervical cancer. The response rate was similar in both treatment arms (60 versus 63%), and overall survival was similar (HR for mortality 0.99, 90% CI 0.79-1.25) with a better safety profile for the carboplatin combination (grade 4 neutropenia, renal insufficiency, nausea, and vomiting). A systematic review published in 2014 also supported the carboplatin alternative to cisplatin [10].
To our knowledge, this case is the only one published in the literature with a significantly superior overall survival and recurrence-free survival, remaining disease-free for 4 years after diagnosis.
Currently, checkpoint inhibitors are a key strategy in the management of metastatic disease. Atezolizumab and pembrolizumab have demonstrated benefits in overall survival.
Atezolizumab, a PD-L1 inhibitor, was evaluated in a phase III trial [11], and showed advantages in progression-free survival and overall survival regardless of PD-L1 status (PFS 13.7 versus 10.4 months; HR 0.62, 95% CI 0.49-0.78 and OS 32 versus 23 months; HR 0.68, 95% CI 0.52-0.88, after a median follow-up of 33 months). It is still pending regulatory approval in several countries.
Pembrolizumab, a PD-1 inhibitor indicated in PD-L1 positive disease (CPS>1), has demonstrated efficacy in a phase III trial with 617 patients [12]. It compared chemotherapy with bevacizumab and pembrolizumab versus placebo, improving progression-free survival (10.4 versus 8.2 months; HR for disease progression or death 0.65, 95% CI 0.53-0.79) and overall survival (26 versus 17 months among the overall population, those with CPS ≥1 29 versus 17 months, and those with CPS ≥10 30 versus 17 months) [13]. Among patients with CPS < 1 (69 patients), the benefit did not reach statistical significance possibly due to insufficient sample size, so the real benefit in this population is not clear (HR for OS 0.87, 95% CI 0.50-1.52).
Conclusion
This case illustrates a detailed description of the management of advanced cervical carcinoma in a high-risk patient. In this case, the individualized management and probably some intrinsic molecular characteristics of the tumor led to the long survivor of the patient. There is still a need to develop new tools for the treatment of tumors with poor prognosis and better selection of patients candidates for treatment. Many of those patients present with adverse prognostic and predictive factors but still benefit from available drugs.
Declarations
Author contributions: Dr. Magda Palka-Kotlowska contributed to the conception, design, and drafting of the work, acquisition and treatment of the patient.
Miss Ximena Ribera-Escobar was responsible of drafting the work.
Dr Luis Cabezón and Magda Palka-Kotlwoska ensured that questions related to the accuracy or integrity of any part of the work were appropriately investigated and resolved.
Dr Sara Custodio-Cabello, Eduardo Oliveros-Acebes and Vilma Pacheco-Barcia helped to the conception and design of the work, drafting oand reviewing it critically for important intellectual content.
Funding: None.
Conflict of interest: Luis Cabezón Gutiérrez declares the following conflicts of interest: Advisory role; Astra Zeneca, Roche, Eisai and Brystol Myers Squibb. Speakers’ bureau; Roche, Astra Zeneca, Brystol Myers Squibb, Merck Serono, Ipsen Pharma, Grunenthal, Kyowa Kirin, Pfizer, Roche and Eisai.
Magda Palka Kotlowska: declares advisory role for Glaxo Smith Kline and Esteve. Speakers’ bureau; Pfizer, Gilead, Daiichi Sankyo, Glaxo Smith Kline, Astra Zeneca and Novartis, Sara Custodio Cabello: declares speakers’ bureau; Fresenius, Abbot, Astelas.
Vilma Pacheco Barcia declares Advisory role: Advanced accelerator applications, a Novartis company. Speakers’ bureau: Merck, Eli Lilly, Eisai, Pierre Fabre. Congress attendance: Merck, Amgen, Merck Sharp and Dhome, Nutri-cia. Grant support: FSEOM and Merck. Other: Amgen. Martín AJM: Consultant or advisory role: GSK, Sanofi, Pfizer-BMS, Celgene, Leo Pharma, Incyte, Astra Zeneca, MSD, Lilly, Servier, Bayer, Roche. Research funding: Leo Pharma, Sanofi, Celgene. Speakers’ bureau: Rovi, Bayer, Menarini, Stada, Daichii Sankyo. Patents, Royalties. Other intellectual property: Risk assessment model in venous thromboembolism in Ximena Ribera Escobar and Eduardo Oliveros Acebes declare no conflicts of interest.
Acknowledgements: To the patient and her family.
References
- National Cancer Institute. Cancer stat facts: Cervical cancer (https://seer.cancer.gov/statfacts/html/cervix.html).
- Surveillance, Epidemiology, and End Results. SEER registry data. 2000 to 2004. http://seer.cancer.gov/
- Fulcher AS, O’Sullivan SG, Segreti EM, Kavanagh BD. Recurrent cervical carcinoma: Typical and atypical manifestations. Radiographics. 1999; 19: S103-S265. doi:10.1148/radiographics.19.suppl_1.g99oc19s103
- Patel CN, Nazir SA, Khan Z, Gleeson FV, Bradley KM. 18F-FDG PET/CT of cervical carci-noma. AJR Am J Roentgenol. 2011; 196(5): 1225-1233. doi:10.2214/AJR.10.5084.
- Lim MC, Lee HS, Seo SS, et al. Pathologic diagnosis and resection of suspicious thoracic me-tastases in pa-tients with cervical cancer through thoracotomy or video-assisted thoracic sur-gery. Gynecol Oncol. 2010; 116(3): 478-482. doi:10.1016/j.ygyno.2009.10.039.
- Lim MC, Lee HS, Seo SS, Kim MS, Kim JY, et al. Pathologic diagnosis and resec-tion of suspicious thoracic metastases in patients with cervical cancer through thoracotomy or video-assisted thoracic surgery. Gyne-col Oncol. 2010; 116(3): 478-82. doi: 10.1016/j.ygyno.2009.10.039.
- Moore DH, Tian C, Monk BJ, Long HJ, Omura GA, et al. Prognostic factors for response to cisplatin-based chemotherapy in advanced cervical carcinoma: A Gynecologic Oncology Group Study. Gynecol Oncol. 2010; 116(1): 44-9. doi: 10.1016/j.ygyno.2009.09.006.
- Tewari KS, Sill MW, Long HJ, Penson RT, Huang H, et al. Improved survival with bevacizumab in advanced cervical cancer. N Engl J Med. 2014; 370(8): 734-43. doi:10.1056/NEJMoa1309748.
- Kitagawa R, Katsumata N, Shibata T, et al. Paclitaxel Plus carboplatin versus paclitaxel plus cisplatin in metastatis or recurrent cervical cancer: The open-Label randomized phase III Trial JCOG0505. J Clin Oncol. 2015; 33(19): 2129-2135. doi:10.1200/JCO.2014.58.4391.
- Lorusso D, Petrelli F, Coinu A, Raspagliesi F, Barni S. A systematic review comparing cispla-tin and car-boplatin plus paclitaxel-based chemotherapy for recurrent or metastatic cervical can-cer. Gynecol Oncol. 2014; 133(1): 117-123. doi:10.1016/j.ygyno.2014.01.042.
- Oaknin A, Gladieff L, Martínez-García J, et al. Atezolizumab plus bevacizumab and chemot-herapy for metastatic, persistent, or recurrent cervical cancer (BEATcc): A randomised, open-label, phase 3 trial. Lancet. 2024; 403(10421): 31-43. doi:10.1016/S0140-6736(23)02405-4.
- Colombo N, Dubot C, Lorusso D, et al. Pembrolizumab for Persistent, Recurrent, or Metasta-tic Cervical Cancer. N Engl J Med. 2021; 385(20): 1856-1867. doi:10.1056/NEJMoa2112435.
- Monk BJ, Colombo N, Tewari KS, et al. First-Line Pembrolizumab + Chemotherapy versus Placebo + Chemotherapy for Persistent, Recurrent, or Metastatic Cervical Cancer: Final Overall Survival Results of KEYNOTE-826. J Clin Oncol. 2023; 41(36): 5505-5511. doi:10.1200/JCO.23.00914.