
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
A case report of Kikuchi disease with aseptic meningitis and literature review
Mei-Tong Jin; Jian-Xin Jia; Xin-Xin Wang*
Baotou Medical College, Inner Mongolia, China.
*Corresponding Author : Xin-xin Wang
Baotou Medical College, Inner Mongolia, China.
Email: 57667478@qq.com
Received : Apr 02, 2024
Accepted : Apr 24, 2024
Published : May 01, 2024
Archived : www.jcimcr.org
Copyright : © Wang XX (2024).
Abstract
We report a case of kikuchi disease with aseptic meningitis in a 11-year-old male who suffered from a high fever without significant triggers 36 days ago and accompanied by enlarged right cervical lymph nodes with tenderness 19 days before admission. The symptoms were controlled after using low-dose dexamethasone, but temperature increased again after stopping dexamethasone, and dexamethasone continued to do well. Three days after discharge, fever and lymph node tenderness relapsed accompanied by unexplainied persistent headache and vomiting, in the frontal and overhead areas headache presented more severe. He was readmitted to hospital due to the aggravated symptoms. Cerebrospinal fluid examination indicated the patient may sufferred from aseptic meningoencephalitis, and necrotizing lymphadenitis was also considered according to the examination results of lymph node puncture biopsy. Therefore, the treatment plan including acyclovir, mannitol, methylprednisolone was employed. On the fourth day of admission, fever and headache were both relieved. This case highlights the rare clinical presentation of Kikuchi disease associated with aseptic meningitis. Lymph node biopsy should be considered early to confirm the diagnosis, and treatment plan need to be adjusted according to the accurate diagnosis. We happen to encounter such cases, reported in the form of summary.
Keywords: Kikuchi-Fujimoto disease; Histiocytic necrotizing lymphadenitis; Aseptic meningitis; Case report.
Citation: Jin M, Jia J, Wang X. A case report of Kikuchi disease with aseptic meningitis and literature review. J Clin Images Med Case Rep. 2024; 5(5): 3020.
Introduction
Kikuchi Disease (KD), also known as histiocytic necrotizing lymphadenitis, is characterized by subacute necrotizing regional lymphadenopathy, and 60 to 90% patients showed enlarged cervical lymph nodes with tenderness [1]. Symptoms of KD mainly include superficial lymph node enlargement, fever, leukopenia [2]. As well as extranodal manifestations. Lymph node biopsy plays an important role in the diagnosis of KD due to there was no typical clinical features and other specific diagnostic index. In clinical practice KD is more likely to be misdiagnosed when accompanied by other diseases, such as aseptic meningitis.
Case presentation
An 11-year-old male child was admitted to the hospital with “intermittent fever for 36 days and lymph node enlargement for 19 days.” 36 days before admission (2023.07.01), the child suffered fever reach up to 39.5OC without obvious induction, temperature can be lowered by oral antipyretic drugs, and then rose again, the heat peak was 3 times/day, accompanied by headache. The patient presented intermittent fever after treatment with “azithromycin, pudilan anti-inflammatory oral liquid, and traditional Chinese medicine decoction” (the specific dosage is unknown). 19 days before admission (2023.07.18), the swelling right cervical lymph nodes were found and the diagnosis were determined as “1. Subacute necrotizing lymphadenitis 2. acute bronchitis”, and the treatment measures given included ceftazidime 1.0 g/time, twice a day, for 6 days. Adenosine monophosphate 0.2 g/time, once a day, for 7 days. Dexamethasone 5 mg daily for three days, then changed to 3 mg once a day untill discontinued. However, the temperature increased again when dexamethasone was stopped, so the original antibiotic was changed to azithromycin 0.5 g/time, once a day, for 7 days, added retoxinin 20 ml/time, once a day, for 8 days. Dexamethasone was continued to be given 5 mg daily for four days, then reduced to 3 mg daily for three days. The child was generally in good condition, and prednisone acetate tablet was given 10 mg/time, once a day after discharge. Meanwhile, they were instructed to take calcium tablets and vitamin D orally. However, he had fever again three days after discharge, and his temperature reached 38.2OC, which could drop by itself and then rise again. On August 20, he developed a persistent headache mainly in the forehead and the top of the head, with an unclear description of its nature and no obvious relief or aggravating factors as well as no apparent cause. The headache was accompanied by vomiting, which was non-ejection stomach contents, no blood and brown substance, about 2-3 times a day. The temperature fluctuated between 37.3-38.5OC, no chills, convulsions and rash appeared with ferver simultaneity. He has been admitted to a community hospital, Ceftriaxone, retoxin and mannitol were used for 2 days, but headache and fever were not significantly relieved and vomiting times increased. On August 22, blood routine examination showed that PCT, SAA, IL-6, neutrophil percentage and erythrocyte sedimentation rate increased rapidly. Lymphocyte percentage, eosinophilic granulocyte percentage, hemoglobin and hematocrit, 25-hydroxyvitamin D were decreased. On August 23, he transferred to our hospital for treatment because of “headache, vomiting and fever for 3 days, aggravated for 1 day”. In the course of the disease, he occasionally had acid reflux, heartburn, mental loss, poor appetite, increased sleep, normal stool but low urine volume. Physical examination showed a full moon face, congestion in the pharynx, swollen and congested tonsils on both sides, hairy body, several swollen lymph nodes on the right neck, the larger 0.5 cm x 0.5 cm, no tenderness, good motion. HE stained sectionexamination findings of right cervical lymph node puncture tissue were showed in Figure 1, in which tissue necrosis can been seen. Immunohistochemical examination results were showed in Figure 2, CD3 (few cells +), CD20 (partial cells +), CD43 (partial cells +), CD68 (histiocytes +), Ki-67 (70% +), Vimentin (+). So necrotizing lymphadenitis was considered according to pathologic examination findings.
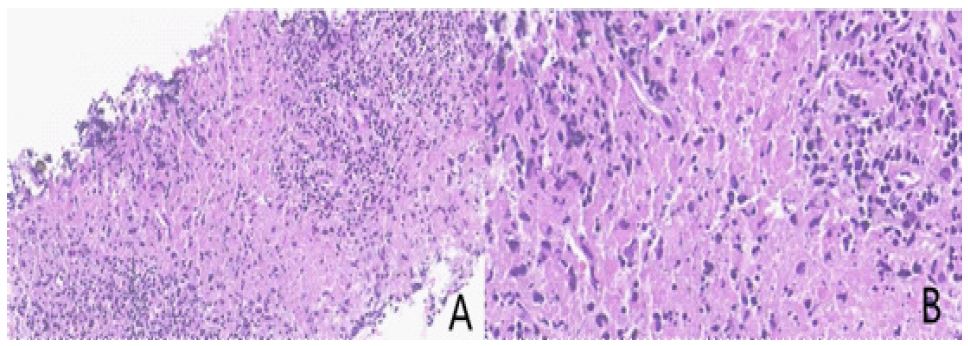
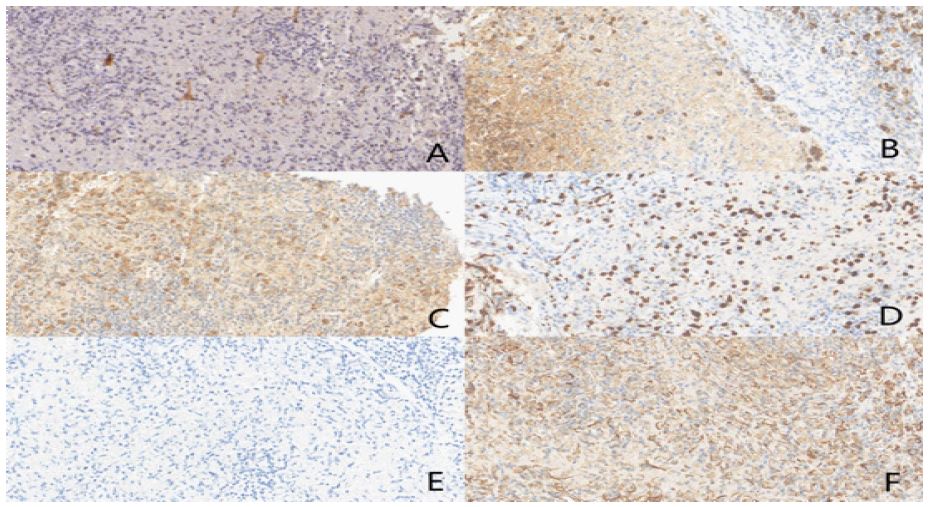
Table 1: CSF cytology of this patient.
| Code Name | Project Name | BearFruit | Unit | Reference Ranges | Methodof Calibration |
|---|---|---|---|---|---|
| GLU | amylaceum | 3.15 | mmol/L | 2.5-4.5 | hexokinase method |
| CL | chlorine | 122.00 | mmol/L | 120-130 | Electrode method |
| NU-TP | Total CSF protein | 458 | mg/L | 200-400 | immunoturbidimetry |
| C-YS | pigment | achromatic colour | |||
| C-ZD | pellucidity | limpid | |||
| C-XBZS | TCS | 32 | 10*6/L | ||
| C-DH | Percentage of uninucleus cells | 94 | % | ||
| C-DGH | Percentage of multileaf nuclear cells | 6 | % | ||
| CJHXB | Old red blood cells | 0 |
After re-hospitalization, the patient was treated with ampicillin cissulbactam and retoxinin, and intravenous methylprednisolone. He still had fever and rashes on both legs, so we stopped ampicillin cissulbactam and switched to loratadine desensitization, after which the rashes on both legs disappeared. Mannitol was used due to obvious headache. His cerebrospinal fluid examination (Table 1) indicated aseptic meningoencephalitis, so we added acyclovir 0.25 g every 8 hours, up-regulated methylprednone to 40 mg every 12 hours, and mannitol to 200 ml every 6 hours. His headache alleviated but generalized flushing and bulboconjunctival congestion developed, sothe antibiotics was disused. By the fourth day, his temperature returned to normal, his headache was gone, and his skin flushing was gradually disappearing. Considering that he had fever several times in the past two months and swollen lymph nodes in his neck, the dosage of methylprednisolone was changed to oral prednisone acetate 20 mg twice a day, and mannitol was gradually reduced. The patient was discharged when all symptoms including fever, headache, nausea and vomiting disappeared. The physical examination showed good mental state, no obvious flushing of the skin all over the body, healing of lip ulcer, no abnormality of heart, lung, abdomen and nervous system.
Discussion
Kikuchi Disease (KD), is a benign and self-limiting rare disease of unknown etiology [3]. At present, there is very limited report on KD with aseptic meningitis, polymononneuritis and acute cerebellar ataxia [4]. The typical age of onset of the disease is less than 30 years, but it occurs in any age group. Recent studies reported that among Asian populations the ratio of KD between of the sexes was 1:1 [5]. The exact etiology of KD is unclear and is currently considered as related to viral infection or autoimmunity [6]. The initial symptoms of patients with KD were enlarged lymph nodes, especially cervical lymph nodes (56% to 98%), fever (77.3%), and sudden high fever or persistent low fever; about 30% of patients with non-specific skin lesions, the rash can be manifested as erythema, nodules, papules, etc., the histopathological characteristics of affected lymph nodes are sometimes very similar to Systemic Lupus Erythematosus (SLE), or even misdiagnosed as SLE rash [7]. In addition, KD may also show joint pain, pharyngeal discomfort, nausea, night sweats and weight loss, but only about 3% to 10% of the patients have spinal nerve system damage [8].
Differential diagnoses of KD include systemic lupus erythematosus lymphadenitis, lymphoid malignancies and various infectious causes including viruses (herpes family, rubella, HIV, parvovirus), bacteria (Hensebartonella, Yersinia enterocolitica and brucella) and parasites (toxoplasma gondii and Entamoeba endohistolytica) [9], Given the differences in these disorders, it is important to exclude them before establishing a diagnosis of KD.
Conclusion
KD with aseptic meningitis is a rare clinical case. For patients with symptoms of recurrent unexplained fever, lymph node biopsy should be adopted as early as possible in the course of the disease to confirm the diagnosis. Early accurate diagnosis can shorten disease course, avoid excessive and unnecessary examinations as well as potentially harmful treatment [10]. Short-term corticosteroids may do well to KD patients with aseptic meningitis presented severe headache, and the efficacy of long-term corticosteroids treatment remains uncertain, patients must undergo follow-up at the onset of subsequent symptoms.
Declarations
Acknowledgments: None to declare.
Conflict of interest: None to declare.
Financial disclosures: None to declare.
Availability of data and materials: All data underlying the findings are fully available.
Ethics approval and consent to participate: No ethical committee approval was required for this case report by the Department, because this article does not contain any studies with human participants or animals. Informed consent was obtained from the patient included in this study.
Funding: This study was supported by the Graduate Education Teaching Reform Project of Baotou Medical College (YJSJG 202204).
Consent for publication: patient gave his written consent to use his personal data for the publication of this case report and any accompanying images.
References
- Iwamoto N, Funahashi M, Shinohara K, et al.Two Cases of Kikuchi Disease Presenting with Aseptic Meningitis and Encephalitis.Intern Med. 2022; 61(17): 2687-2689. doi: 10.2169/internalmedicine.7724-21.
- Komagamine T, Nagashima T, Kojima M, et al.Recurrent aseptic meningitis in association with Kikuchi-Fujimoto disease: case report and literature review.BMC Neurol. 2012; 12: 112. Published 2012 Sep 29. doi: 10.1186/1471-2377-12-112.
- Khishfe BF, Krass LM, Nordquist EK.Kikuchi disease presenting with aseptic meningitis.Am J Emerg Med. 2014; 32(10): 1298. 1-1298.e12982. doi: 10.1016/j.ajem.2014.03.029.
- Pei, et al. “ histiocytic necrotizing lymphadenitis with aseptic meningitis and a review of the literature. Anhui Medicine. 2023; 27.09: 1783-1786.
- Patel J, Haltom M, Jackson C.The great masquerader: Kikuchi-Fujimoto disease presenting as fever of unknown origin.J Natl Med Assoc. 2022; 113(6): 680-682. doi: 10.1016/j.jnma.2021.07.006.
- Patel DR, Shah AB, Shah HR, Thorat KB.Kikuchi Disease: A Rare Cause of Aseptic Meningitis.Neurol India. 2019; 67(4): 1131-1133. doi: 10.4103/0028-3886.266242.
- Song Y, Liu S, Song L, et al.Case Report: Histiocytic Necrotizing Lymphadenitis (Kikuchi-Fujimoto Disease) Concurrent With Aseptic Meningitis.Front Neurol .2021;12:565387. Published 2021. doi: 10.3389/fneur.2021.565387
- Shen Jing, Zhang eshi, Zhang Gejuan, Chang Ming, Nan Guangxian. Thitiocytic necrotizing lymphadenitis starting with aseptic meningitis: a case report. The Journal of Stroke and Neurological Diseases. 2022; 0093(04): 362-363. doi: 10.19845/j.cnki.zfysjjbzz.
- Xu Li, Zhang Xiaoyi, Wang Anhai, Xue Zhanyou. Analysis of the clinical characteristics of necrotizing lymphadenitis with aseptic meningitis as the first symptom (with a case report). China Nursing Medicine. 2018; 10.047(10): 1116-1118. doi: 10.13517/j.cnki.ccm.
- Zhan Wencai, Huang Xujie, Shi Weicheng & Liu Yong. (2021). Diagnosis and treatment of 2 cases of Kikuchi disease and literature review. Shenzhen Journal of Integrated Traditional Chinese and Western Medicine. 2021; 21.077 (21): 195-197 + 203. doi: 10.16458/j.cnki.1007-0893.