
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Low grade liver angiosarcoma, rare primary liver malignancy, presented with right upper abdominal pain: A case report
Hassan Akhtar*; Sadaf Anjum
Department of Internal Medicine, Cavan General Hospital, Republic of Ireland.
*Corresponding Author : Hassan Akhtar
Department of Internal Medicine, Cavan General Hospital, Republic of Ireland.
Email: dr.hassanakhtar121@gmail.com
Received : Mar 25, 2024
Accepted : Apr 25, 2024
Published : May 02, 2024
Archived : www.jcimcr.org
Copyright : © Akhtar H (2024).
Abstract
Liver angiosarcoma is a rare primary liver malignancy which originates from sinusoidal endothelial cells, accounting for approximately 1.8% of primary hepatic malignancy, affecting mostly men in their sixth or seventh decade of life. In the present report, the case of 77 year old gentleman who presented with right upper abdominal pain initially investigated for urinary symptoms by GP found to have incidental liver lesion on CT KUB which was proven to be low grade angiosarcoma on biopsy results.
Citation: Akhtar H, Anjum S. Low grade liver angiosarcoma, rare primary liver malignancy, presented with right upper abdominal pain: A case report. J Clin Images Med Case Rep. 2024; 5(5): 3023.
Background
Primary hepatic malignancies are grossly divided into two groups: epithelial and non-epithelial. Non-epithelial tumors include hepatic angiosarcoma, rhabdomyosarcoma, lymphoma and hemangioendothelioma [1]. Liver angiosarcoma is a non-epithelial mesenchymal tumor which usually presents with nonspecific symptoms of anemia, abdominal pain, abdominal distention, fever of unknown origin and weight loss [2,3]. Due to aggressive nature of these tumors, they usually metastasize at the time of diagnosis [4]. It can progress and cause fulminant hepatic failure [5]. There is an association of angiosarcomas with environmental and occupational exposure to thorium dioxide, arsenic, radiation, vinyl chloride [6] and diseases like von Recklinghausen & hemochromatosis [7].
Case report
This is a case of 77 year old gentleman, presented to emergency department with history of right upper abdominal pain ongoing for last 6 months not associated with nausea, vomiting, jaundice and weight loss. His past medical history included COPD, diverticulosis and tuberculous colitis in his twenties. He worked as a bar man, lived with his family, quit smoking 30 years ago and drank alcohol quite often. Patient denied any history of hepatitis, diabetes mellitus or family history of malignancies. He was not taking any regular medications and has no known drug allergies. CT KUB was done 1 week before admission to hospital that was organized by General Practitioner as part of work up of Urinary Tract Infection, which showed 1.2 cm simple renal cyst in upper pole of right kidney and incidental solid liver mass with surrounding smaller lesions in right lobe of liver.
On physical examination, abdomen was soft, mild tenderness noted in right upper quadrant but no viscera palpable. Percussion elicited pain over the liver area. Cardiovascular and respiratory examination was normal. Laboratory results showed in Table 1.
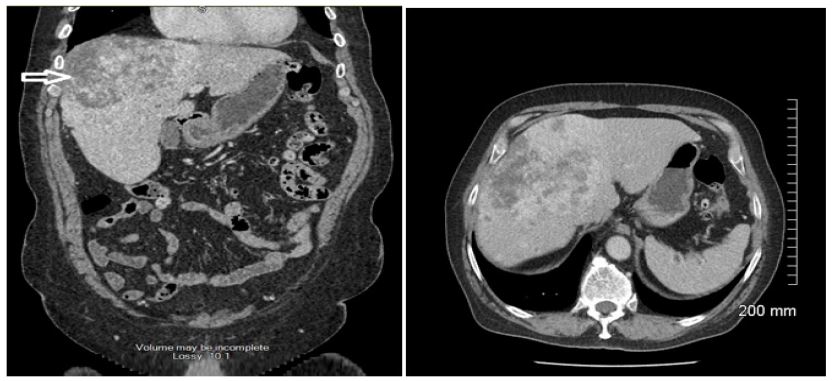
Subsequent workup including CT Abdomen/Pelvis with contrast was done which showed large heterogeneous liver mass involving right lobe of liver with irregular liver contour (Figures 1A-1B). Multiple hypodense smaller lesions of 5-10 mm noted in both lobes of liver. Primary liver malignancy was suspected based on radiological images. CT-Thorax and CT brain done as a part of metastatic workup were normal.
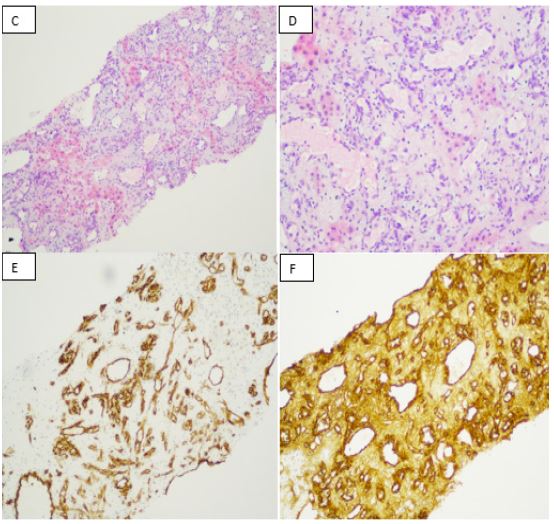
Subsequent liver biopsy results showed a core of liver with complete effacement of the normal architecture by atypical vascular lesions with proliferation of vascular spaces lined by atypical endothelial cells (Figures 1C-1D). Immunostaining for the vascular endothelial markers including CD34 and Factor VIII were positive (Figures 1E-1F) plus SMA stain within the stroma was positive. Tumor was negative for D2-40. These features were highly suggestive of mesenchymal vascular lesion. Differential diagnosis included: Epithelioid hemangioendothelioma, Kaposiform Angiosarcoma and Angiosarcoma.
Case was discussed in Hepatology multidisciplinary meeting in St Vincent Hospital, Dublin and was sent to histopathologist in Brigham & Women’s Hospital Boston, USA for another opinion and vascular lesions were confirmed as Angiosarcoma. It was morphologically low grade and well differentiated.
Outcome and follow-up
Due to aggressive nature of tumor surgical option was not viable and it was recommended by oncologist that chemotherapy will not give any benefit in long term survival. So all the options were discussed with patient and he opted for palliative treat ment. Patient was admitted again with confusion and shortness of breath and hemoptysis. Liver functions were markedly deranged and was found to have pulmonary embolism as cause of shortness of breath. Patient was treated by palliative team primarily and he passed away within few days of admission to hospital due to liver failure.
Table 1: Results.
| WCC | 10 × 109/L |
| Hemoglobin | 12.6 g/dL |
| Platelet Count | 227 × 109/L |
| Alanine Aminotransferase (ALT) | 20 U/L |
| Aspartate Transaminase (AST) | 29U/L |
| Alkaline Phosphatase (ALP) | 153 U/L |
| γ -glutamyl Transpeptidase (GGT) | 214 U/L |
| Albumin | 37 g/L |
| Total Bilirubin (TBIL) | 6 μmol/L |
| Prothrombin Time (PT | 11.0 sec |
| International Normalized Ratio (INR) | 1 |
| Alfa Fetoprotein | Normal |
| Carcinoembryonic Antigen (CEA), | Normal |
| Ca 19-9 | Normal |
| Prostate Specific Antigen (PSA) | Normal |
Discussion
Angiosarcoma is an aggressive malignancy of endothelial origin which commonly involves head & neck (60%) [8]. Liver angiosarcoma is more common in males with male to fem ale ratio 3:1, mostly presents with non-specific symptoms and liver function derangement especially alkaline phosphatase seen in advanced stages of disease and thrombocytopenia [9]. Due to vascular nature of the tumor they can easily rupture and presents with intrabdominal bleeding and peritoneal metastasis [10]. Liver angiosarcomas were traditionally linked with occupational exposure to vinyl chloride, arsenic, thorium dioxide and viral hepatitis but a study in Taiwan found no major role of these carcinogens found in drinking water with incidence of hepatic angiosarcomas [11]. The diagnosis of hepatic angiosarcoma requires imaging studies and liver biopsy as tumor markers are usually within normal range [12]. Hepatic angiosarcomas are positive for vascular antigens including CD31, CD34 and mesenchymal vimentin [13]. There are few treatment options available for angiosarcoma including tumor resection and liver transplantation. Recent study revealed that survival rates are very poor even after liver transplantation and it is contraindicated for diffuse hepatic angiosarcoma [14]. Rapid progression, early metastasis, high recurrence rates and resistance to available chemo-radiotherapy results in poor long term survival in primary hepatic Angiosarcoma. But palliative chemotherapy has shown improved survival in some cases [15]. Most patients die within 6 months of diagnosis [16].
Learning points
• Liver angiosarcoma can present with vague complaints of abdominal discomfort to nausea and malaise.
• It is a challenging diagnosis and demands a multidisciplinary approach.
• These tumors are aggressive in nature and prognosis is very poor as in this case survival was only few months.
Acknowledgments: We are very thankful to Dr. Hala Rizkalla (Consultant Histopathologist) Cavan General Hospital, Dr. Niamh Nolan (Consultantpathologist, St Vincent’s University Hospital, Dublin especially Dr. Christopher Fletcher, Brigham Women’s Hospital Harvard, USA.
References
- Casanova D, Figueras J, Pardo F. 7th ed. ARAN Ediciones. Cirugía Hepática, Guías Clínicas De La Asociación Española De Cirujanos. 2004; 141-161.
- Locker GY, Doroshow JH, Zwelling LA and Chabner BA. The clinical features of hepatic angiosarcoma: A report of four cases and a review of the English literature. Medicine (Baltimore). 1979; 58: 48-64. Google Scholar: PubMed/NCBI.
- Molina E, Hernandez A. Clinical Manifestatition of primary hepatic angiosarcoma. Dig Dis Sci. 2003; (4): 677-82.
- Kim HR, Rha SY, Cheon SH, Roh JK, Park YN, Yoo NC. Clinical features and treatment outcomes of advanced stage primary hepatic angiosarcoma. Ann Oncol. 2009; 20: 780-787.
- Marco Montell García, Raúl Romero Cabello, Raul Romero Feregrino, Mercado Atri Moises, Rafael Trejo Estrada, Padilla-Rodríguez Alvaro, et al. Angiosarcoma of the liver as a cause of fulminant liver failure. http://casereports.bmj.com/content/2012/bcr-2012-006417.full.pdf
- Kojiro M, Nakashima T, Ito Y, Ikezaki H, Mori T, Kido C. Thorium dioxide-related angiosarcoma of the liver. Pathomorphologic study of 29 autopsy cases, Arch Pathol Lab Med. 1985; 109(9): 853-7.
- Chandra S Bhati, 1 Anand N Bhatt, 1 Graham Starkey,1 Stefan G Hubscher, [PubMed].
- Angiosarcoma: clinical and imaging features from head to toe. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5594986/.
- Hepatic Angiosarcoma: A Challenging Diagnosis https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6235643/.
- Liver angiosarcoma, a rare liver malignancy, presented with intraabdominal bleeding due to rupture- a case report [PubMed].
- Arsenic, vinyl chloride, viral hepatitis, and hepatic angiosarcoma: A hospital-based study and review of literature in Taiwan (PDF Download Available). Available from: https://www.researchgate.net/publication/51894463_Arsenic_vinyl_chloride_viral_hepatitis_and_hepatic_angiosarcoma_A_hospital-based_study_and_review_of_literature_in_Taiwan
- Bioulac-Sage P, Laumonier H, Laurent C, Blanc JF, Balabaud C. Benign and malignant vascular tumors of the liver in adults. Semin Liver Dis. 2008; 28: 302-314.
- Leader M, Collins M, Patel J, Henry K. Vimentin: an evaluation of its role as a tumour marker. Histopathology. 1987; 11: 63-72.
- Yoshida Y et al. Liver transplantation for cryptogenic liver failure caused by diffuse hepatic angiosarcoma: Case report. Surg Case Rep. 2017; 3: 21.
- Kim HR, Rha SY, Cheon SH, Roh JK, Park YN, Yoo NC. Clinical features and treatment outcomes of advanced stage primary hepatic angiosarcoma. Annal Oncol. 2009; 20(4): 780-7.
- Timaran CH, Grandas OH, Bell JL. Hepatic angiosarcoma: long-term survival after complete surgical removal. Am Surg. 2000; 66(12): 1153-1157. PubMedGoogle Scholar.