
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Inferior mesenteric artery embolization for postpartum hemorrhage due to vaginal lacerations: A case report
Emika Murasawa1; Tomoki Tozawa1; Kento Hatakeyama1; Manabu Hashimoto2*
1Department of Radiology, Akita University School of Medicine, Japan.
2Department of Radiology, Akita City Hospital, Japan.
*Corresponding Author : Manabu Hashimoto
Department of Radiology, Akita City Hospital 4-30 Kawamoto Akita City, Akita 010-0933, Japan.
Tel: +81-18-823-4171, Fax: +81-18-866-7026;
Email: ac789213@akita-city-hospital.jp
Received : Apr 05, 2024
Accepted : Apr 25, 2024
Published : May 02, 2024
Archived : www.jcimcr.org
Copyright : © Hashimoto M (2024).
Abstract
Postpartum Hemorrhage (PPH) is a major cause of maternal mortality. We report a case of a patient with PPH due to vaginal lacerations, where the Inferior Mesenteric Artery (IMA) was the source of bleeding. The 31-year-old woman was transferred to our hospital because of vaginal bleeding 4 hours after a normal vaginal delivery. Contrast-enhanced computed tomography showed contrast extravasation from the right posterior vaginal wall. Angiography revealed an abnormal stain, suspected to be due to leakage of contrast from the right internal pudendal artery. Embolotherapy was not performed owing to occlusion caused by an iatrogenic dissection during the catheter maneuver. Vaginal bleeding persisted after the angiography. The pelvic angiogram from the second session did not show any abnormal findings. Aortography clearly showed extravasation from the superior rectal branch of the IMA. We occluded this vessel with N-butyl-2-cyanoacrylate. Hemostasis was obtained after embolotherapy.
Keywords: Postpartum hemorrhage; Embolotherapy; Inferior mesenteric artery.
Citation: Murasawa E, Tozawa T, Hatakeyama K, Hashimoto M. Inferior mesenteric artery embolization for postpartum hemorrhage due to vaginal lacerations: A case report. J Clin Images Med Case Rep. 2024; 5(5): 3024.
Introduction
Postpartum Hemorrhage (PPH) remains a major cause of maternal mortality [1]. Uterine atony is the most frequent cause of PPH, accounting for 70% of such cases of bleeding [2]. Genital tract injury is also a frequent cause of PPH associated with pelvic hematoma [3]. Currently, Transcatheter Arterial Embolization (TAE) is widely used for managing intractable PPH [4-7]. In most cases, branches of the anterior trunk of the internal iliac artery, such as the uterine and internal pudendal arteries, are the target for embolization [4-7]. The Inferior Mesenteric Artery (IMA) is a rare source of PPH [8,9]. Herein, we present a case of a patient with PPH due to vaginal lacerations, who we successfully treated through TAE of the IMA using an N-Butyl-2-Cyanoacrylate (NBCA) mixture.
Case report
A 31-year-old woman with an uneventful medical history vaginally delivered a full-term baby. One hour after delivery, vaginal bleeding occurred and was controlled by repair of the episiotomy site. Four hours after delivery, the patient developed a vaginal wall hematoma and vaginal bleeding from a difficult suture site. Subsequently, she was transported to our hospital for embolotherapy.
Physical and laboratory examinations conducted upon her admission to our hospital yielded the following results: blood pressure, 125/86 mmHg; pulse rate, 111/bpm; hemoglobin, 10.4 g/dL; platelet count, 238.000/μL; activated partial thromboplastin time, 22.3s; Prothrombin Time (PT), 12.7s; PT-international normalized ratio, 0.95; D-dimer, 10.67 μg/mL; and fibrinogen, 341.0 mg/dL. The estimated bleeding volume was approximately 1450 mL, and she did not have a history of disseminated intravascular coagulopathy.
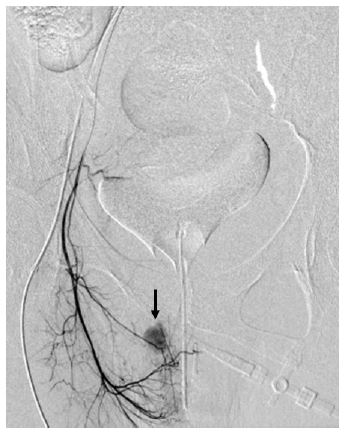
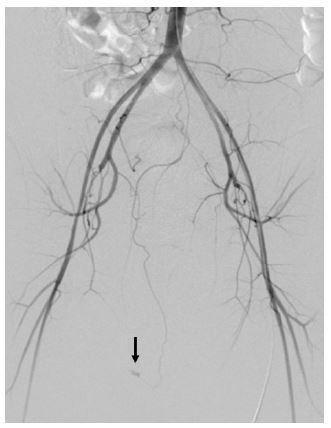
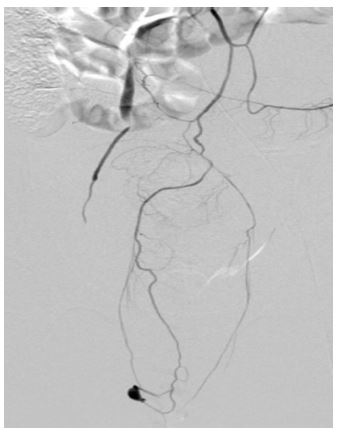
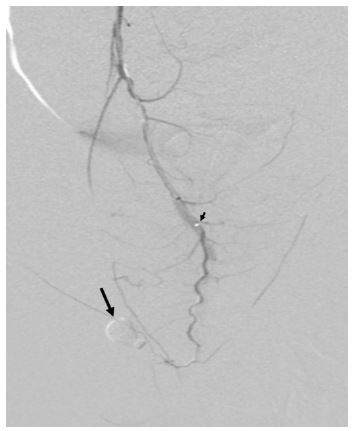
Contrast-Enhanced Computed Tomography (CECT) revealed an abnormal spotty contrast enhancement, suggesting a contrast leak or pseudoaneurysm on the right posterior vaginal wall. The pelvic angiogram revealed an abnormal stain, which was suspected to be due to leakage of a contrast from the right internal pudendal artery (Figure 1). We advanced a microcatheter into the peripheral portion of the artery. During the catheter maneuver, an arterial dissection occurred. Fluorography with manual injection of contrast indicated severely decreased flow in the artery. The pelvic angiogram obtained after this event showed that the stain had disappeared. Although the embolotherapy was halted, vaginal bleeding did not subside. The CECT image obtained 3 hours after the first angiography showed the abnormal contrast enhancement at the same position as on the previous scan. We decided to perform an angiography again. The bilateral iliac arteriography did not detect the bleeding point. Subsequently, aortography was used for the evaluation, whereupon it clearly revealed a contrast leak (pseudoaneurysm) from the superior rectal branch of the IMA (Figure 2). After placing a guiding catheter at the IMA, we coaxially advanced a triaxial microcatheter system (Carnelian, HF 2.7 Fr and MARVEL S 1.3 Fr; Tokai Medical Product Inc., Aichi, Japan) as close as possible to the bleeding point. Under digital subtraction angiography, we carefully injected 0.3 ml of an NBCA mixture [NBCA (Hystoacryl; B Braun, Melsungen, Germany) mixed with iodized oil (Lipiodol Ultra Fluid; Guerbet, Roissy, France) at a ratio of 1:3] and successfully embolized the artery (Figure 3). No complications were observed after the embolotherapy. Bleeding did not recur and the patient was discharged 2 days after the TAE procedure.
Discussion
Vaginal laceration caused by the expansion of the birth canal is responsible for approximately 2% of PPH cases [10]. In most patients, it is treated and controlled by surgical repair and/or vaginal packing [11]. When conservative approaches fail to stop the bleeding, TAE is commonly the next-line of therapy, with a high success rate [4,8]. In our patient, the superior rectal artery was mainly responsible for the vaginal bleeding and is generally the cause for approximately 5-10% of bleeding due to vaginal lacerations [4,6]. The potential mechanism of IMA involvement in PPH is as follows: shearing of the vaginal wall causes injury to the branch of the superior rectal artery [12] and/or communication between the vaginal and superior rectal arteries [13]. We should bear in mind that the IMA may be injured in patients with vaginal lacerations. Anatomically, it is also reasonable that the external pudendal artery can be a source of bleeding [4].
Various embolic materials have been used in previous studies, with gelatin sponge particles being the most popular [4,9,12,13]. The gelatine sponge was not considered for our patient, because the bleeding source was a pseudoaneurysm. Instead, the operator decided to use NBCA as an embolic agent during the procedure. Because the patient did not have coagulopathy, microcoils might also have been a preferable embolic material. Regardless of the type of embolic agent used, we had to pay attention to avoiding reflux and migration of the embolus into non-target territories to reduce bowel ischemia.
Conclusion
In conclusion, the IMA could be a source of bleeding in patients with PPH caused by vaginal lacerations. Aortography should be performed to identify the source of bleeding, especially when pelvic angiography fails to identify this.
References
- Khan KS, Wojdyia D, Say I, Gűlmezoglu AM, Van Look PF. WHO analysis of causes of maternal death: a systematic review. Lancet. 2006; 367: 1066-1074.
- Callaghan WM, Kuklina EV, Berg CJ. Trends in postpartum hemorrhage: United States. 1994-2006. Am J Obstet Gynecol. 2010; 202; 1-6.
- Chichakli LO, Atrash HK, MacKay AP, Musani AS, Berg CJ. Pregnancy-related mortality in the United States due to hemorrhage: 1979-1992. Obstet Gynecol. 1999; 94: 721-725.
- Lee SM, Shin JH, Shim JJ, Yoon KW, Cho KJ, Kim JW, Ko HK. Postpartum haemorrhage due to genital tract injury after vaginal delivery: safety and efficacy of transcatheter arterial embolization. Eur Radiol. 2018; 28: 4800-4809.
- Fargeaudou Y, Soyer P, Morel O, Sirol M, le Dref O, Boudiaf M, Dahan H, Rymer R. Severe primary postpartum hemorrhage due to genital tract laceration after operative vaginal delivery: successful treatment with transcatheter arterial embolization. Eur Radiol. 2009; 19: 2197-2203.
- Koganemaru M, Nonoshita M, Iwamoto R, Kuhara A, Nabeta M, Kugiyama T, Lozuma Y, Nagata S, Abe T. Endovascular management of intractable postpartum hemorrhage caused by vaginal laceration. Cardiovasc Intervent Radiol. 2016; 39: 1159-1164.
- Zhang E, Liu L, Owen R. Pelvic artery embolization in the management of obstetrical hemorrhage: predictive factors for clinical outcomes. Cardiovasc Intervent Radiol. 2015; 38: 1477-1486.
- Chen C, Chu HH, Shin JH, Li HL, Ko HK, Yoon HK. Inferior mesenteric artery embolization for persistent postpartum hemorrhage after sufficient bilateral iliac arteries embolization: safety and efficacy in eight patients. Br J Radiol. 2019; 92: 20180896.
- Kawakami N, Uchiyama F, Harada A, Yamada T, Nishimura J. Two case studies on inferior mesenteric artery embolization for primary postpartum hemorrhage. Intervent Radiol. 2022; 7: 26-29.
- Combs CA. Murphy EL, Laros RK Jr. Factors associated with post-partum hemorrhage with vaginal birth. Obstet Gynecol 1991; 77: 69-76.
- Biehl DR. Antepartum and postpartum hemorrhage. In: Schnider SM, Levinson C (eds). Anesthesia for Obstetrics, 2nd edn. Williams & Wilkins, Baltimore, MD. 1987; 385-394.
- Kim CH, Jeon GS, Lee SJ, Kang SH. Embolization of the inferior mesenteric artery for post-partum hemorrhage with a vaginal laceration: a case with unusual collateral supply. J Obstet Gynecol Res. 2016; 42: 1878-1880.
- Gentric JC, Koch G, Lesoeur M, Hebert T, Nonent M. Diagnosis and management of puerperal hematomas: two cases. Cardiovasc Intervent Radiol. 2013; 36:1174-1176.