
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Pulmonary artery sarcoma masking as pulmonary embolism: A case report
Effrosyni Dima1*; Dimitra Fasfali1; Panagiotis Deleilias2; Christina Vourlakou3; Konstantina Dede1; Andreas Asimakos1; Ioanna Sigala1; Ioannis Kalomenidis1; Paraskevi Katsaounou1; Anastasia Kotanidou1; Anastasia Anthi1; Stylianos Ε Orfanos1; Ioanna Dimopoulou1
11st Department of Critical Care, National and Kapodistrian University of Athens (NKUA) Medical School, Evangelismos General Hospital, Athens, Greece.
2Department of Cardiothoracic and Vascular Surgery, Evangelismos General Hospital, Athens, Greece.
3Department of Pathology, Evangelismos General Hospital, Athens, Greece.
*Corresponding Author : Effrosyni Dima
1st Department of Critical Care, National and Kapodistrian University of Athens (NKUA) Medical School Evangelismos General Hospital, 45-47, Ipsilandou St., Athens 10676, Greece.
Tel: +30-6948481432;
Email: efi_dima@yahoo.gr
Received : Mar 25, 2024
Accepted : Apr 26, 2024
Published : May 03, 2024
Archived : www.jcimcr.org
Copyright : © Dima E (2024).
Abstract
Introduction: PAS is a rare mesenchymal tumour originating from the intimal layer of the pulmonary artery, that is usually misdiagnosed as acute or chronic PE, leading to delayed diagnosis and treatment.
Case presentation: We present a 41 years old woman with PAS treated initially as PE. Imaging studies, particularly CTPA and PET/CT contributed to the correct diagnosis. Definite diagnosis required biopsy. Although PAS carries a poor prognosis, it may be treated by surgery; the fact that pulmonary track and right pulmonary artery in this case were almost occluded, surgery was considered to be the best approach offering both definite diagnosis and treatment. The patient underwent complete tumour resection and subsequent chemotherapy, and has survived to the present day, approximately 2.5 years following diagnosis.
Discussion: Because of its scarcity, PAS is often misdiagnosed as thromboembolic disease. However, there are indications that lead to the correct diagnosis. Clinical signs that should raise the suspicion of PAS include the lack of symptom improvement despite adequate anticoagulation, non-acute symptom onset and the presence of systemic symptoms. Imaging indications of diagnosis include the “wall eclipsing sign”, lobulated bulging margins, gadolinium enhancement during MRI, and FDG uptake during PET/CT. Early and aggressive surgical removal seems to play a vital role in patients’ survival. Perioperative and late mortality, however, remain high. A variety of imaging modalities including CT, MRI, cardiac echocardiogram and PET/CT may be required to diagnose, assess disease extent, and aid clinicians to design the treatment plan before surgery.
Conclusion: The poor prognosis of PAS is often due to delayed diagnosis. Identifyingclinical and radiological characteristics of PAS early on can facilitate accuratediagnosis and timely surgical intervention.
Keywords: Pulmonary artery sarcoma; Pulmonary embolism; Chronic thromboembolic disease; Diagnosis; Treatment.
Citation: Dima E, Fasfali D, Deleilias P, Vourlakou C, Dede K, et al. Pulmonary artery sarcoma masking as pulmonary embolism: A case report. J Clin Images Med Case Rep. 2024; 5(5): 3027.
Introduction
Pulmonary Artery Sarcoma (PAS) is a misdiagnosed medical entity, often initially diagnosed as acute or chronic pulmonary embolism (PE) or pulmonary hypertension. Patients present with nonspecific symptoms [1,2], and diagnosis tends to be both challenging and delayed. Imaging test such as Computed Tomographic Pulmonary Angiography (CTPA), Magnetic Resonance Imaging (MRI), cardiac echocardiogram and Positron Emission Tomography/Computed Tomography (PET/CT) have been described to depict characteristic images suggestive of PAS [3-5]. Patients’ survival is poor. Although the optimal treatment plan is not yet clarified, early and aggressive surgical removal seems to play a crucial role in extending the patient’s lifespan [6,7]. This case report aims at raising awareness of an often initially underdiagnosed medical condition, which, however, calls for a prompt diagnosis and early surgical intervention.
Case presentation
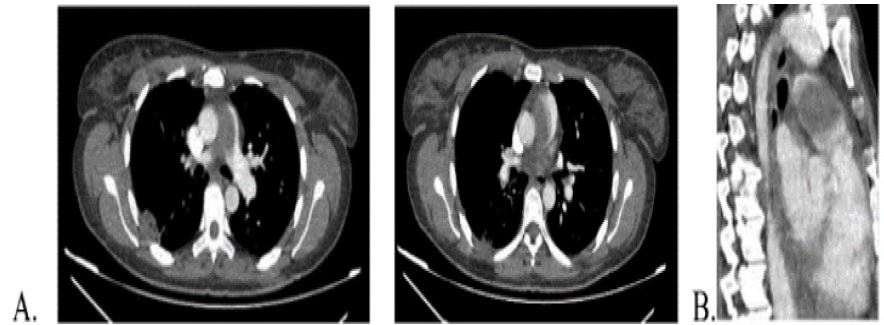
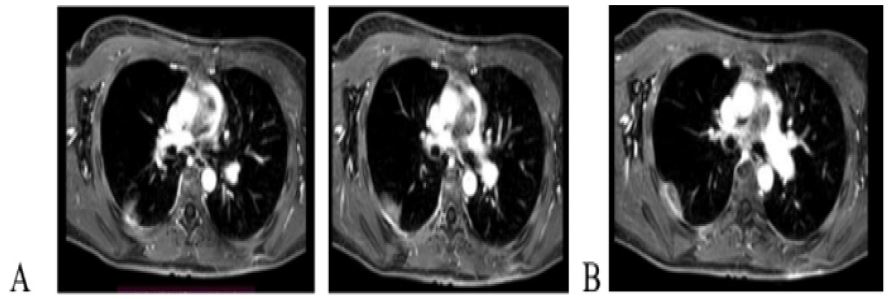
A 41-year-old woman was transferred to our hospital from a regional hospital, where she had been hospitalized for 2 weeks. The patient reported progressive exertional dyspnoea and fatigue for 6 weeks and thoracic pain, non-productive cough and intermittent fever for two weeks. Her past medical history was unremarkable. At the first hospital, there were not significant pathological findings on clinical examination. Patient’s vital signs upon admission were within normal limits (oxygen saturation=97% on FiO2=21%, hemodynamically stable, afebrile). Electrocardiogram, chest XR and an initial laboratory investigation (cell blood count (CBC), d-dimers, biochemistry and troponin) were normal. PCR test for COVID 19 was also negative. The patient underwent CTPA, which revealed a large filling defect in the pulmonary artery trunk and the right main pulmonary artery, as well as a peripheral ground-glass opacity with areas of consolidation (Figure 1). A transthoracic echocardiogram was also carried out, with no pathological findings. The patient was started tinzaparin and antibiotics. The patient reported no change in symptoms, and a second CTPA was carried out after two weeks. The CTPA report described: “I) a hypodense lesion (43 mm x 36 mm x 37 mm) that originates from pulmonary artery valves, ascends to pulmonary artery occluding almost 80% of its lumen, overrides to the right and left main pulmonary arteries, extends further to the right main pulmonary artery, causing almost a full occlusion, II) hilar lymphadenopathy, and III) a triangular consolidation in the right lower lung lobe”. An abdominal CT was also carried out, that had no pathological findings. A lung MRI was also performed describing the mass as an intraluminal lesion of the pulmonary artery trunk and right main branch, which was giving the impression of extending to the aortopulmonary window, with a mild dilation of pulmonary artery (Figure 2). After injection of gadolinium, no enhancement was observed. The study was inconclusive as to whether the finding depicted a tumour or thrombus. The patient was transferred to our hospital for further investigation; she presented with mild tachycardia and tachypnoea. Laboratory investigation yielded normal CBC and troponin, increased Erythrocyte Sedimentation Rate (ESR) and C-Reactive Protein (CRP). Transthoracic cardiac echogram did not reveal futures of pulmonary hypertension and did not show the presence of a mass in the right ventricular outflow track or in the pulmonary artery.
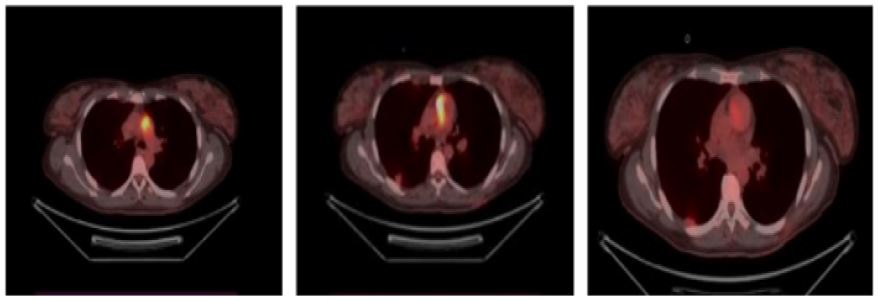
Taking all of the laboratories and imaging findings into account, as well as the patient’s gradual initiation of symptoms, the presence of systemic symptoms, and theabsence of patient’s response to full anticoagulation, the possibility of a neoplasm was highly considered. The patient underwent a PET/CT, which revealed a lesion of maximum standardized uptake value (SUVmax) 17 in the lumen of the pulmonary artery at the level of the pulmonary artery trunk to right main pulmonary artery and the pulmonary artery valves, and an area of SUVmax 3 in the right lung with hypo pleural distribution.
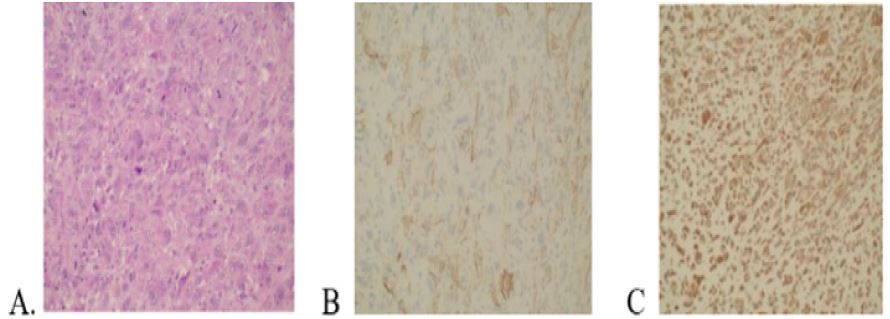
Due to high suspicion of PAS and the fact that pulmonary track and right pulmonary artery were almost occluded, the patient underwent a complete surgical resection of the tumour. The pulmonary artery valves were not affected. Macroscopically it was described by pathology as a neoplastic-appearing lesion with lobular outline and partial polypoid configuration, 4.8 x 3.7 x 2.7 cm, solid, (Figure 4), with elastic texture in cross sections and locally mucosal/necrotic appearance. The histopathological findings were compatible with pulmonary artery intima sarcoma/low-grade sarcoma with FNCLCC grade G3 differentiation. The pathologic stage was pT1N0 (8th edition AJCC 2017) [8]. Immunohistohemichal stain revealed intense and diffuse nuclear expression of cyclic-dependent kinase 4 (CDK4), no expression of MDM-2 protein, focal expression of α-smooth muscle actin (α-SMA), as well as intense and diffuse expression of vimentin and p53 (Figure 5). FISH testing revealed no amplification of the MDM2 and CDK4 genes. The patient’s post-operative course was uncomplicated, and was referred to Oncology for the continuation of treatment with the antineoplastic agents doxorubicin and ifosfamide. After almost 2.5 years the patient is alive, having a very good performance status.

Discussion
Pulmonary artery sarcoma is a rare (0.001-0.03% based on autopsy) aggressive malignancy, originating from the intimal layer of the pulmonary trunk and arteries [9]. First described in 1923 by Mandelstamm, [10] its true incidence is unknown, since a few hundred cases only have been reported, mostly as case reports [6,7]. Both sexes seem to be affected equally, with the mean age of diagnosis being 55 years [11]. Tumours usually arise from the pulmonary trunk (85%), involving the right and left pulmonary arteries in more than 50% of the cases, and may extend to the pneumonic valve and right ventricular outflow tract in 32% and 10% of the respective cases [12]. Patients commonly present with symptoms of dyspnoea, shortness of breath, cough, haemoptysis or chest pain. Symptoms are nonspecific and systemic ones including fatigue and cachexia may also coexist [1,2]. Symptomatology can easily mask as acute or chronic PE. Several authors have tried to identify PAS symptoms and compare them with those of PE in order to facilitate differential diagnosis. Cim et al reported that the symptoms of dyspnoea, chest pain, and haemoptysis were not statistically significantly different between PAS and PE [13]. Longer duration of symptoms and absence of Deep Vein Thrombosis (DVT) were favouring PAS. However, it is not unusual for patients to present with PE without DVT, a clinical presentation that accounts for 20-60% of PE cases [14,15]. On the other hand, PAS-like other malignancies can be associated with DVT. The duration of symptoms, as well as the gradual onset, may help distinguishing PE from PAS [8]; these features however may not be of value in the case of chronic pulmonary thromboembolism. The presence of fever, weight loss, and digital clubbing make PAS more likely [9,16]. Another feature that raises the suspicion of PAS is the lack of patient improvement despite adequate anticoagulation. Laboratory tests such as d-dimers, B-type Natriuretic Peptide (BNP), CRP and ESR can be elevated in both PAS and acute or chronic PE. The values of d-dimers and BNP are lower in PAS, whereas CRP and ESR are higher. Finally, PAS can trigger the presence of coagulators as well as an inflammatory process [5,12,17].
The diagnosis of PAS cannot be based on laboratory tests, and a biopsy is required. The imaging studies may depict features suggestive of PAS aiding the clinician to decide upon further investigation with endovascular catheter performed biopsy or surgery, procedures that may carry complications. Especially surgery carries a high perioperative and late mortality [12]. A variety of imaging modalities including CT, MRI, cardiac echocardiogram and PET/CT are usually required to describe the tumour mass and assess disease extent.
PAS appears as a massive embolus on CTPA, blocking almost the entire lumen of the pulmonary arteries. The tumour mass aligns with the pulmonary vascular tree, and the free end convex to the blood flow, forming the “wall eclipsing sign”, which is a characteristic sign of PAS [3]. The emboli are not usually totally occluding the main pulmonary artery, and the filling defects usually appear flat or cup shaped. In addition, lobulated PAS often creates sharp angles with the vessel wall, whereas chronic PE tends to form a blunt angle [18]. In our case, the CTPA implied that the lesion was not a thrombus, leading to further investigation with MRI. The latter can distinguish PAS from PE by assessing flow and gradients throughout the pulmonary artery vasculature [4]. PAS is usually depicted with aneurysm- or grape-like distal structures having heterogeneous enhancement [18]. The level of enhancement is associated with tumour differentiation [4]. PAS tumours tend to have higher T2 signal intensity compared to PE [19]. In our case, MRI could not distinguish PAS from PE due to no enhancement after gadolinium infusion. In our patient PET/CT was the most helpful in distinguish PAS from PE. PET/CT can provide information regarding the tumour’s metabolic activity and the presence or not of distal metastasis. PET/CT can differentiate between PAS and PE by means of the SUVmax. It has been demonstrated by several studies that the mean PAS SUVmax is significantly higher than this of PE [20,21]. However, it is not the optimal imaging test, as both cases of PAS with low 18F-FDG uptake [22-24] and thrombi with high 18F-FDG uptake have been described [25]. Reasons for the low PAS 18F-FDG uptake have been considered the following: limited presence of tumour cells, an abundance of mucinous tissue [22], tumour necrosis, haemorrhage and calcification [23], or chronic thrombosis [24].
In our case, although the PET/CT was the most informative, all imaging modalities aided to design the surgical plan, as surgery was considered the best approach for our patient, offering simultaneously both diagnosis and treatment. Due to low 18F-FDG uptake, a biopsy of the triangle, hypopleural consolidation was not considered, as it most likely represented a pulmonary infract. Surgical treatment offers a chance for improved symptoms and long-term outcome [6]. Surgery is considered successful only when tumour resection is complete [26], however it depends on its location and its distant spread [27]. Incomplete resection has been shown to lead to a lower median survival from those who undergo complete resection [28,16]. Comparison between endarterectomy and complete resection is difficult due to the scarcity of cases [21]. Neoadjuvant chemotherapy may shrink the tumour size, facilitating its resection. Further chemotherapy during follow-up seems to reduce the risk of metastasis, although it does not affect local recurrence. There are no standard chemotherapy guidelines. Doxorubicin and ifosfamide are advocated as first choice [11,16,3]. Furthermore, patients undergoing multimodality treatment had an improved median survival compared to those having a single modality approach [16].
Conclusion
Until now PAS has been considered a malignant tumour with very poor prognosis. Misdiagnosis as acute or chronic PE contributes to the delayed treatment. Although early and aggressive tumour resection offers a chance for better survival, surgery carries various complications. Furthermore, multimodality treatment has been shown to improve mortality rates. Knowing the clinical and radiologic features of PAS, and combing the imaging modalities, can lead to the correct diagnosis in time and plan the best surgical/treatment approach, resulting finally to better survival.
References
- Pu X, Song M, Huang X, et al. Clinical and radiological features of pulmonary artery sarcoma: A report of nine cases. Clin Respir J. 2018; 12(5): 1820-29.
- Baker PB, Goodwin RA. Pulmonary artery sarcoma. ArchPathol Lab Med. 1985; 109: 35-39.
- Gan HL, Zhang JQ, Huang XY, Yu W. The wall eclipsing sign on pulmonary artery computed tomography angiography is pathognomonic for pulmonary artery sarcoma. PLoS ONE. 2013; 8(12): e83200.
- Von Wyler MC, Chan EY, Reardon MJ. Imaging and Surgical Treatment of Primary Pulmonary Artery Sarcoma. Int J Cardiovasc Imaging. 2019; 35(8): 1429-33.
- Liu MX, Ma ZH, Jiang T, et al. Differential diagnosis of Pulmonary Artery Sarcoma and Central Chronic Pulmonary Thromboembolism using CT and MR Images. Heart Lung Circ. 2018; 27(7): 819-27.
- Yin K, Zhang Z, Luo R, et al. Clinical features and surgical outcomes of pulmonary artery sarcoma. J Thorac Cardiovasc Surg. 2018; 155(3): 1109-15.
- Srivali N, Yi ES, Ryu JH. Pulmonary artery sarcoma mimicking pulmonary embolism: a case series. QJM. 2017; 110: 283-86.
- Amin MB, Edge SB, Greene FL, et al. editors. AJCC Cancer Staging Manual. 8th ed. Switzerland: Springer, 2017.
- Miura S, Meirmanov S, Nakashima M, et al. Intimal sarcoma of the pulmonary artery: report of an autopsy case. Pathol Res Pract; 2005; 201(6): 469-74.
- Mandelstam M. Über primäre Neubildungen des Herzens. Virchows Arch. 1923; 245: 43-54
- Bandyopadhyay D, Panchabhai TS, Bajaj NS, Patil PD, Bunte MC. Primary pulmonary artery sarcoma: a close associate of pulmonary embolism-20-year observational analysis. J Thorac Dis. 2016; 8(9): 2592-601.
- Rabah Al-Mehisen et al. Primary pulmonary artery sarcoma: A rare and overlooked differential diagnosis of pulmonary embolism. Clues to diagnosis. Int J Surg Case Rep. 2019; 65: 15-19.
- Kim C, Kim MY, Kang JW, Song JS, Lee KY, Kim SS. Pulmonary artery intimal sarcoma versus pulmonary artery thromboembolism: CT and clinical findings. Korean J Radiol. 2018; 19(4): 792-802.
- Palareti G, Antonucci E, Dentali F, et al. Patients with isolated pulmonary embolism in comparison to those with deep venous thrombosis. Differences in characteristics and clinical evolution. Eu J Intern Med. 2019 Nov; 69: 64-70.
- Van Gent JM, Zander AL, Olson EJ, et al. Pulmonary embolism without deep venous thrombosis: De novo or missed deep venous thrombosis? J Trauma Acute Care Surg. 2014; 76(5): 1270-4.
- Blackmon SH, Rice DC, Correa AM, et al. Management of primary pulmonary artery sarcomas. Ann Thorac Surg. 2009 Mar; 87(3): 977-84.
- Sakai K, Minoura Y, Matsui T, Kaneko K, Kobayashi Y. Primary pulmonary artery intimal sarcoma case with elevated coagulation markers. J. Clin. Diagn. Res. 2017; 11(4) OD10-OD11.
- Wittram C, Maher MM, Yoo AJ, Kalra MK, Shepard JA, McLoud TC. CT angiography of Pulmonary Embolism: diagnostic criteria and causes of misdiagnosis. Radiographics. 2004; 24(5): 1219-38.
- Kronzer E, Robinson SI, Collins DA, McBane RD. Primary pulmonary artery sarcoma versus pulmonary thromboembolism: a multimodal imaging comparison. J Thromb Thrombolysis. 2021; 52(4): 1129-32.
- Ito K, Kubota K, Morooka M,et al. Diagnostic usefulness of 18F-FDG PET/CT in the differentiation of pulmonary artery sarcoma and Pulmonary Embolism. Ann Nucl Med. 2009; 23(7): 671-6.
- Xi XY, Gao W, Gong JN, et al. Value of (18)F-FDG PET/CT in differentiating malignancy of pulmonary artery from pulmonary thromboembolism: a cohort study and literature review. Int J Cardiovasc Imaging. 2019; 35(7): 1395-403.
- Koike T, Iwata H, Hirose K, Minamino T. A case report of pulmonary artery intimal sarcoma negative for 18F-FDG mimicking pulmonary thromboembolism. Eur Heart J Case Rep. 2023; 7(4): ytad140.
- Lee DH, Jung TE, Lee JH, Shin DG, Park WJ, Choi JH. Pulmonary artery intimal sarcoma: poor 18F-fluorodeoxyglucose uptake in positron emission computed tomography. J Cardiothorac Surg. 2013; 8: 40.
- Liu Z, Fan L, Liang S, Wund Z, Huang H. A primary pulmonary artery sarcoma masquerading pulmonary embolism: a case report and literature review. Thrombosis Journal. 2024; 22: 4.
- Triantafyllidi H, Iordanidis D, Mpahara A, et al. Giant Pulmonary Artery Thrombotic Material, Due to Chronic Thromboembolic Pulmonary Hypertension, Mimics Pulmonary Artery Sarcoma. Medicina (Kaunas). 2021; 20; 57(9): 992.
- Viana-Tejedor A, Mariño-Enríquez A, Sánchez-Recalde A, López-Sendón JL. Intimal sarcoma of the pulmonary artery: diagnostic value of different imaging techniques. Rev. Esp. Cardiol. 2008; 61(12): 1363-65.
- Grazioli V, Vistarini N, Morsolini M, et al. Surgical treatment of primary pulmonary artery sarcoma. J Thorac Cardiovasc Surg. 2014 Jul; 148(1): 113-8.
- Mussot S, Ghigna MR, Mercier O, et al. Retrospective institutional study of 31 patients treated for pulmonary artery sarcoma. Eur J Cardiothorac Surg. 2013; 43(4): 787-93.