
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 5
Pulmonary lymphoepithelial carcinoma: Clinical image
Imane Boujguenna1,2,3*; Ayman Ismail1; Hanane Rais1
1Department of Pathology, Mohammed VI University Hospital, MARRAKECH, Morocco.
2Faculty of Medicine and Pharmacy Marrakech, Cadi Ayyad University Marrakech, Morocco.
3Faculty of Medicine and Pharmacy Guelmim, Ibnou Zohr University Agadir, Morocco.
*Corresponding Author : Imane Boujguenna
Department of Pathology, Mohammed VI University Hospital, MARRAKECH, Morocco.
Email: imane.boujguenna1992@gmail.com
Received : Apr 13, 2024
Accepted : Apr 29, 2024
Published : May 06, 2024
Archived : www.jcimcr.org
Copyright : ©Boujguenna I (2024).
Abstract
Pulmonary lymphoepithelial carcinoma is a rare tumor. It most commonly affects organs derived from the primitive foregut: pharynx, thymus, salivary glands. It is exceptional in the lungs and associated with EBV infection. We report a case of pulmonary lymphoepithelial carcinoma collected in the pathology department of the Mohammed VI University Hospital in Marrakech.
Keywords: Lymphoepithelial carcinoma; Diagnosis; Pathology; EBV.
Citation: Boujguenna I, Ismail A, Rais H. Pulmonary lymphoepithelial carcinoma. J Clin Images Med Case Rep. 2024; 5(5): 3030.
Introduction
Pulmonary Lymphoepithelial Carcinoma (PLEC) is a poorly differentiated carcinoma associated with marked lymphocytic inflammatory infiltrate and the presence of Epstein Barr virus (EBV) within the nuclei of tumor cells (WHO 2021). Rare Entity: < 1% of all lung cancers [1].
Materials and methods
We report a case of pulmonary lymphoepithelial carcinoma collected in the pathology department of the Mohammed VI University Hospital in Marrakech.
Medical observation
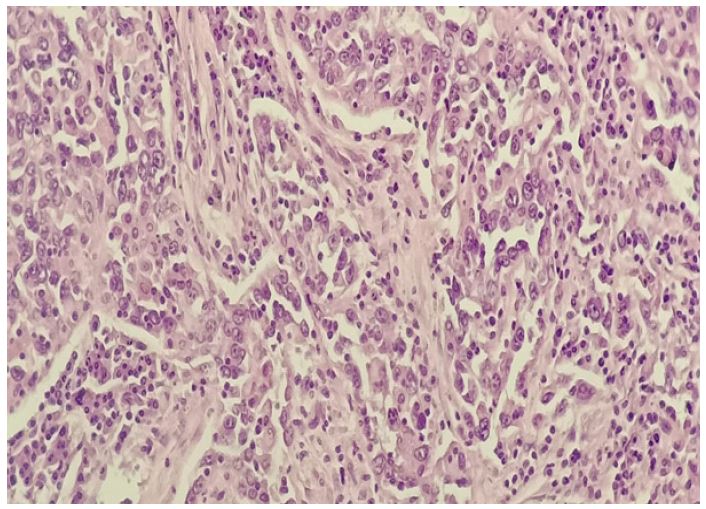
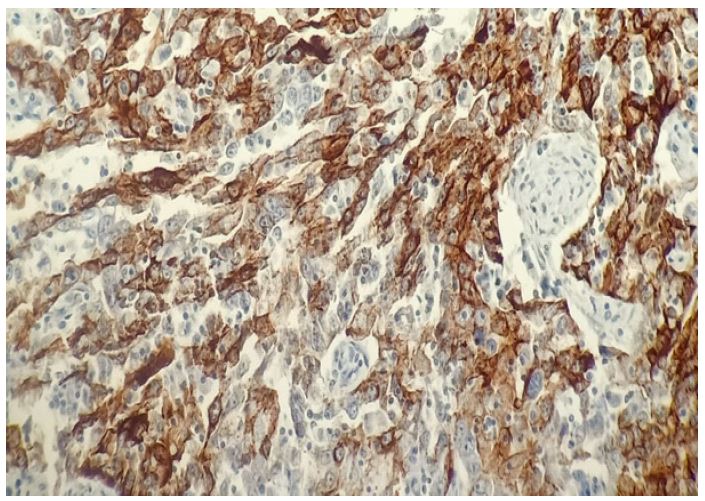
This is a 57-year-old man, non-smoker with no significant medical history. He presented with chest pain, progressive dry cough, and general malaise. Thoracic CT scan revealed an apical mass in the right upper lobe. The management plan was to perform a scanno-guided pulmonary biopsy. Histological examination showed a poorly differentiated and infiltrating carcinoma. Immunohistochemical study showed negativity for TTF1 and P40 antibodies. The therapeutic management plan was to perform a right upper lobectomy. Macroscopic examination revealed a whitish neoplasm measuring 7.5 cm in diameter and firm consistency. Microscopic examination showed infiltrating carcinomatous proliferation arranged in sheets, diffuse nests, and large syncytial masses with indistinct intercellular boundaries of medium to large-sized carcinoma cells. The nuclei were highly nucleolated with vesicular chromatin, finely granular. The stroma showed abundant fibro-inflammatory reaction rich in lymphocytes and plasma cells with a pushing-border invasion front type with extensive tumor necrosis. Immunohistochemistry showed negativity for TTF1, P40, Napsin, ck 20, chromogranin, and synaptophysin antibodies with positivity for CK7, EMA, and EBV antibodies.
Discussion
Pulmonary lymphoepithelial carcinoma is a rare tumor [1]. It most commonly affects organs derived from the primitive foregut: pharynx, thymus, salivary glands. It is exceptional in the lungs and associated with EBV infection [2]. This tumor affects young non-smokers. Macroscopically, it is a solitary, well-circumscribed tumor with a size ranging from 1 to 11 cm in diameter. Histologically, it shows masses and nests of undifferentiated large cells Syncytial appearance with vesicular nuclei, marked anisocytosis, often high mitotic index. The lymphoid stroma consists of small regular lymphocytes. Immunohistochemical study is characterized by negativity for TTFI, P40, Napsin, ck 20, chromogranin, and synaptophysin antibodies with positivity for CK 7, EMA, and EBV antibodies. FISH study shows EBV in tumor cell RNA.
Declarations
Competing interests: The authors declare no conflicts of interest.
Funding: No funding.
Authors’ contributions: All the authors contributed to the conduct of this work.
Acknowledgments: To anyone who has participated in the care of this patient directly or indirectly.
References
- World Health Organization Classification of Lung Tumors. 2021.
- Wong and Teo. Case report: lymphoepithelial-like carcinoma of the lung-a chronic disease? World Journal of Surgical Oncology. 2012; 10: 91.
- Yuan-Chun Huang, Ching Hsueh, Shang-Yun Ho, Chiung-Ying Liao. Lymphoepithelioma-Like Carcinoma of the Lung: An Unusual Case and Literature Review.
- Sakda Sathirareuangchai, Kirk Hirata. Pulmonary. Lymphoepithelioma-like Carcinoma. Arch Pathol Lab Med. 2019; 143.