
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Rare case of unilateral phlebectasia of the internal jugular vein in an adult: A case report
Pushkar Mendiratta1*; Saikat Bhattacharjee2; Saurabh Maheshwari3
1Department of Radiodiagnosis, Military Hospital, Mathura, India.
2Department of Radiodiagnosis, Command Hospital, Lucknow, India.
3Department of Radiodiagnosis, Military Hospital, Shimla, India.
*Corresponding Author : Pushkar Mendiratta
Department of Radiodiagnosis, Military Hospital Mathura, Mathura, 281001, Uttar Pradesh, India.
Tel: +91-9731159681,
Email: pushkar_indian@yahoo.co.in
Received : Apr 13, 2024
Accepted : Apr 29, 2024
Published : May 06, 2024
Archived : www.jcimcr.org
Copyright : © Mendiratta P (2024).
Abstract
Introduction: Phlebectasia is a non-tortuous saccular or fusiform dilatation of a vein. Commonly encountered in the paediatric age group, it usually involves upper extremity and neck veins. Phlebectasia of the internal jugular vein presents as a soft compressible, transient swelling in the neck, which increases in size on straining and Valsalva manoeuvre.
Case presentation: We report an infrequent case of an adult female, with a painless unilateral neck swelling of insidious onset and no other associated symptoms, diagnosed as internal jugular vein phlebectasia on ultrasound findings alone. Internal jugular vein phlebectasia is an uncommon cause of neck swelling in an adult.
Conclusion: Findings of unilateral right sided neck swelling with characteristic increase in size on Valsalva manoeuvre as in our case are the typical clinical and ultrasonographic findings noted. This case emphasises the need to consider phlebectasia in the differential diagnosis when dealing with a neck mass even in an adult. Investigation by ultrasonography and colour Doppler is adequate and further diagnostic and surgical interventions may well be avoided.
Keywords: Phlebectasia; Internal Jugular Vein; Ultrasonography; Case report; Valsalva manoeuvre.
Abbreviations: IJV: Internal Jugular Vein; USG: Ultrasonography; PTFE: Polytetrafluoroethylene.
Citation: Mendiratta P, Bhattacharjee S, Maheshwari S. Rare case of unilateral phlebectasia of the internal jugular vein in an adult: A case report. J Clin Images Med Case Rep. 2024; 5(5): 3031.
Introduction
ChordomasPhlebectasia, an abnormal saccular or fusiform dilatation of the vein without concomitant tortuosity, is an infrequently encountered venous malformation with unclear etiology. Usually seen in paediatric age group, it can affect any vein, though it involves the upper extremity and neck veins more than the lower extremity veins. Among the neck veins, it affects the internal and the external jugular veins more than the anterior jugular and the superficial communicus veins. Among the neck veins, two-thirds involve the Internal Jugular Vein (IJV) [1]. It differs from venous varix, which is tortuous and from venous aneurysms, which are usually segmental and secondarily acquired, presenting in adulthood.
IJV phlebectasia presents as a soft, painless, compressible right-sided neck mass [2]. It increases in size on straining by coughing, crying and with the Valsalva manoeuvre. Patient presents because of the neck swelling or due to rarely associated symptoms of hoarseness of voice and dysphagia. We report a case of an adult female with a unilateral, painless neck swelling, diagnosed to be IJV phlebectasia, an uncommon diagnosis in adulthood [3]. The case description is followed by a brief narrative of the entity and its imaging findings, highlighting the need to include it in differentials even in an adult with neck swelling.
Case presentation
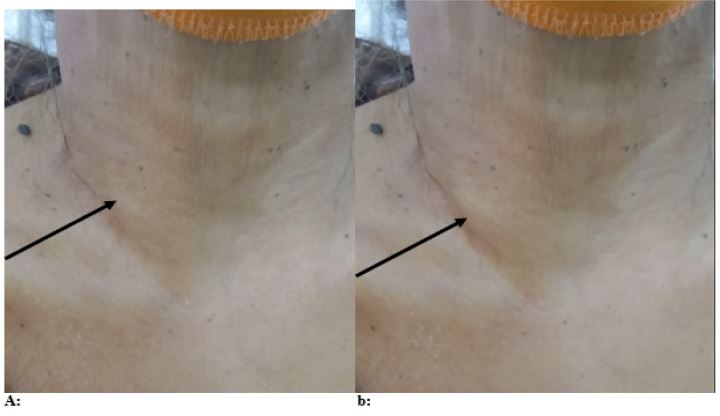
A 60-years-old, female patient presented to our hospital with a right-sided neck swelling (Figure 1a). The swelling had an insidious onset of six months, without any obvious progression in size. It was painless, without any history of facial puffiness, dyspnoea, dysphagia, change in voice or any other neck mass. There was no history of neck trauma or surgery. The swelling was clinically localised to the anterior triangle, being pulsatile on inspection and nontender, soft, and compressible on palpation. There was no associated venous bruit. It was noted to reduce incompletely in size on lying down and become mildly prominent on standing and with the Valsalva manoeuvre (Figure 1b).
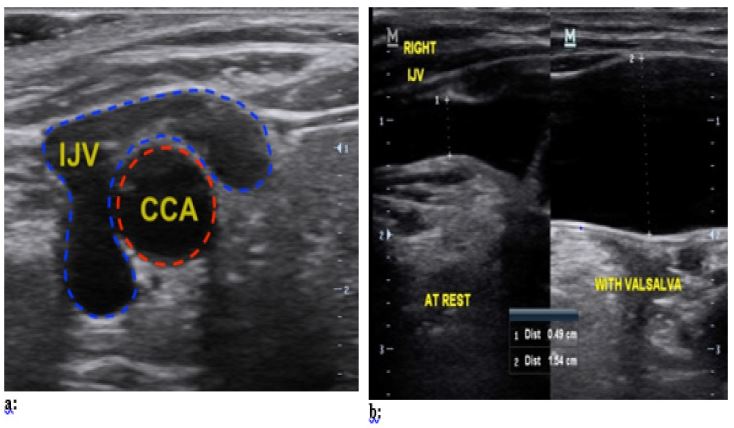
Ultrasonography (USG) revealed a dilated right IJV (Figure 2a and 2b), in the lower neck, just short of its drainage into the right subclavian vein. On performing the Valsalva manoeuvre, the dilated IJV was noted to increase in calibre from 4.9 mm to 15.4 mm (Figure 2b). Colour Doppler revealed a complete luminal filling of the vein with transmitted arterial pulsations from the Common Carotid artery. The patient was diagnosed as a case of phlebectasia of the right IJV. No further investigations were required since the findings were typical of phlebectasia. The patient was explained about its benign course. The treatment options, both conservative and surgical were elucidated to the patient. The patient was managed conservatively with regular follow up with the surgical outpatient department.
Internal jugular vein phlebectasia was first described as early as in 1928 by Zukschwerdt and got its present name by Gerwig. It has been described by several pseudonyms such as venous aneurysm, venous cyst, aneurysmal varix and venectasia [4]. It is characterised by thinning of the venous muscle layer, hypertrophy of connective tissue and focal intimal thickening histopathologically [2]. More common in the paediatric age group, its differentials are a broad group. However, change in size with Valsalva manoeuvre narrows the differentials to include tumours or cysts of the superior mediastinum, external laryngeal diverticulae and laryngocoeles [5,6].
A few plausible etiologies have been postulated, most notable being an increased scalenus anterior muscle tone, compression of the IJV between clavicular head and the cupola of the right lung, trauma and congenital primary weakness of the venous muscle layer [7]. It is more commonly unilateral and five times more common on the right, which may be due to the close contact of right innominate vein with the right apical pleura, leading to augmented transmission of increased intrathoracic pressure to the right IJV [2,6]. Another reason may be higher placement of valves in the right IJV than the left with absent valves in the right brachiocephalic vein, expediting retrograde flow on the right. Overall, the condition is reported more in males than in females.
It is usually asymptomatic with a benign course, but rare complications like thrombosis, congestive heart failure and hemorrhage secondary to trauma have been reported [8]. Horner’s syndrome is also reported to be associated with IJV phlebectasia, due to post-ganglionic disruption of third order neurons of the oculo-sympathetic pathway and is characterised by a clinical triad of ipsilateral miosis, partial ptosis and hemifacial anhidrosis [4]. Its association with Menke’s disease has been postulated and a case of its intracranial extension has also been described [9]. Clinically, IJV phlebectasia presents as a neck swelling with typical clinical, USG and Doppler findings, as described in our case [2]. The characteristic increase in size on coughing, sneezing, crying and Valsalva manoeuvre clinches the diagnosis, with USG and colour Doppler imaging usually enough for its confirmation. USG accurately defines its extent and its relationship with other neck structures. Duplex sonogram shows a venous waveform. Further evaluation may be done when in doubt or suspecting a complication, by contrast enhanced Computerised Tomography, Magnetic Resonance Imaging, Magnetic Resonance Angiography, CT Angiography or Digital Subtraction Angiography [2,4].
Choice of management for both paediatric and adult IJV phlebectasia is usually conservative, with monitoring required for any change in size, necessitating follow-up, since they are not reported to regress on their own [5]. It is advisable to caution the patient to avoid any direct trauma to the neck to prevent hemorrhage. In patients with phlebitis, thrombus formasurgical treatment is recommended. The conventional surgical options include ligation of the affected vein, resection of the dilated segment, sheathing of the affected segment in a Polytetrafluoroethylene (PTFE) tube graft or longitudinal constriction suture venoplasty. In recent years, constriction suture venoplasty and encapsulation are being preferred since they avoid venous occlusion. Anticoagulation therapy however is not recommended [2,4,10].
Conclusion
IJV phlebectasia, an uncommon diagnosis for an adult with neck mass, requires a high index of suspicion on the part of the clinician. Change in size with Valsalva narrows the probable diagnosis and appropriate investigation with USG and colour Doppler usually confirms it. Hence going overboard with superfluous investigations can be avoided.
Declarations
Ethics approval and consent to participate: Not applicable.
Consent for publication: Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Competing interests: The authors declare that they have no competing interests.
Funding: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Acknowledgements: Nil.
References
- Bhattacharya D, Endrakanti M, Kumar R. Right Internal Jugular Vein Phlebectasia: A Rare Cause of Neck Swelling. Case Rep Pediatr. 2017; 2017(1): 1-3.
- Malik V, Kumari A, Murthy T. Unusual case of focal neck swelling: Phlebectasia of internal jugular vein with intracranial extension. Int J Appl Basic Med Res. 2015; 5(1): 58-60.
- Husain P, Saxena S, Ahmed SK, Tapparwal A. Jugular Vein Phlebectasia (IJP): Surgically Manageable But Ignored Entity. Indian J Otolaryngol Head Neck Surg. 2022; 74(2): 2372-2375.
- Başbuğ HS, Göçer H, Günerhan Y, Erdem A, Özışık K. A rare internal jugular vein phlebectasia: Review of the literature. Turk Gogus Kalp Dama. 2016; 24(4): 759-762.
- Baker JB, Ingraham CR, Fine GC, Iyer RS, Monroe EJ. Pediatric jugular vein aneurysm (phlebectasia): report of two cases and review of the literature. Radiol Case Rep. 2017; 12(2): 391-395.
- Matsunaga K, Kishi K. Phlebectasia of the external jugular vein with thrombosis: report of a case. Surg Today. 2014; 44(6): 1180-3.
- Bora MK. Internal Jugular Phlebectasia: Diagnosis by Ultrasonography, Doppler and Contrast CT. J Clin Diagn Res. 2013; 7(6): 1194-6.
- Figueroa-Sanchez JA, Ferrigno AS, Benvenutti-Regato M, Caro-Osorio E, Martinez HR. Internal jugular phlebectasia: A systematic review. Surg Neurol Int. 2019; 10: 106.
- Reede DL, Garcon E, Smoker WR, Kardon R. Horner’s syndrome: clinical and radiographic evaluation. Neuroimaging Clin N Am. 2008; 18(2): 369-85.
- Alenezi M, Alaglan A, Almutairi A, Alanazy S, Al Wutayd O. Unilateral internal jugular vein phlebectasia in an adult: Management and one year follow-up. SAGE Open Med Case Rep. 2019; 7: 1-4.