
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Ginger in the nose, ginger in the brain
Rituja Chauhan1*; Moinuddin Sultan2; Prabodhini Gadhari3 ; Padma Badhe4
1Junior Resident, Department of Radiology, Vedantaa Institute of Medical Sciences, Dahanu-401606 Maharashtra, India.
2Assistant Professor, Department of Radiology, Vedantaa Institute of Medical Sciences, Dahanu-401606 Maharashtra, India.
3Senior Resident, Department of Radiology, Vedantaa Institute of Medical Sciences, Dahanu-401606 Maharashtra, India.
4Professor, Department of Radiology, Seth GS Medical College and KEM Hospital, Dr Ernest Borges Rd, Parel, Mumbai- 400012, Maharashtra, India.
*Corresponding Author : Rituja Chauhan
Resident, Department of Radiology, Vedantaa Institute of Medical Sciences, Dahanu-401606, Maharashtra, India.
Email: rituja.chauhan@gmail.com
Received : Mar 06, 2024
Accepted : Apr 30, 2024
Published : May 07, 2024
Archived : www.jcimcr.org
Copyright : © Chauhan R (2024).
Citation: Chauhan R, Sultan M, Gadhari P, Badhe P. Ginger in the nose, ginger in the brain. J Clin Images Med Case Rep. 2024; 5(5): 3033.
Case description
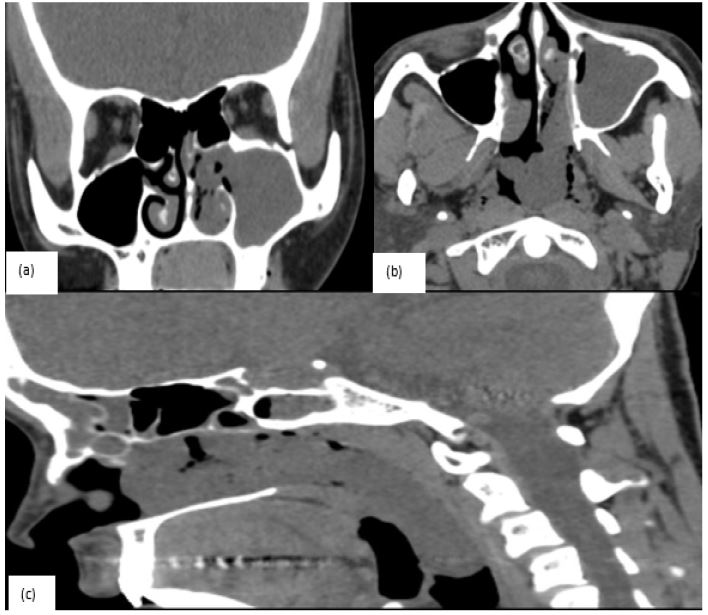
A 35-year-old female with a history of 8 years of amenorrhea presented with complaints of nasal stuffiness, difficulty in swallowing, and gradual onset dyspnoea for the past 15 days. On a detailed account, we found that the patient also suffered from snoring and had oral breathing with few episodes of choking. On clinical examination, a large, smooth, bluish-coloured intranasal polypoidal mass could be seen on the anterior rhinoscopy, extending posteriorly to the oropharynx on the posterior rhinoscopy. On NCCT, a ginger-shaped, lobulated soft tissue mass measuring 9.7 x 1.1 x 1.2 cm with a CT density of 57 HU was seen in the left nasal cavity with multiple projections. One of them occupying the left maxillary antrum, anterior projection through the maxillary ostium into the left anterior nasal cavity between the lateral wall and the middle turbinate, and, posterior projection extending through the left posterior choanae into the oropharynx till the epiglottis.
At the same time, interestingly, a well-defined, lobulated soft tissue density sellar mass lesion was noted in the middle cranial fossa. The patient was further advised dynamic MRI brain contrast study on which the seller lesion was noted to be well-defined T1 isointense, T2 hyperintense, intensely enhancing on gadolinium contrast, measuring 3 x 3 x 4.5 cm (AP x Trans x CC) in the pituitary fossa. The mass superiorly extended to the 3rd ventricle, anteriorly compressing the optic chiasma, and inferiorly extended into the left sphenoid and right posterior ethmoid sinus. Laterally, the mass was invading the bilateral cavernous sinus, encasing the internal carotid arteries, crossing their lateral wall to abut the right temporal lobe on the right, and just touching the left temporal lobe. Routinely, pituitary macro adenoma is seen to give a snowman appearance but, here in our case, it was seen as a large lobulated, irregularly shaped mass giving rise to an appearance of ginger. The final diagnosis was given as pituitary macrodenoma with bilateral Knosp grade III and a left antrochoanal polyp.

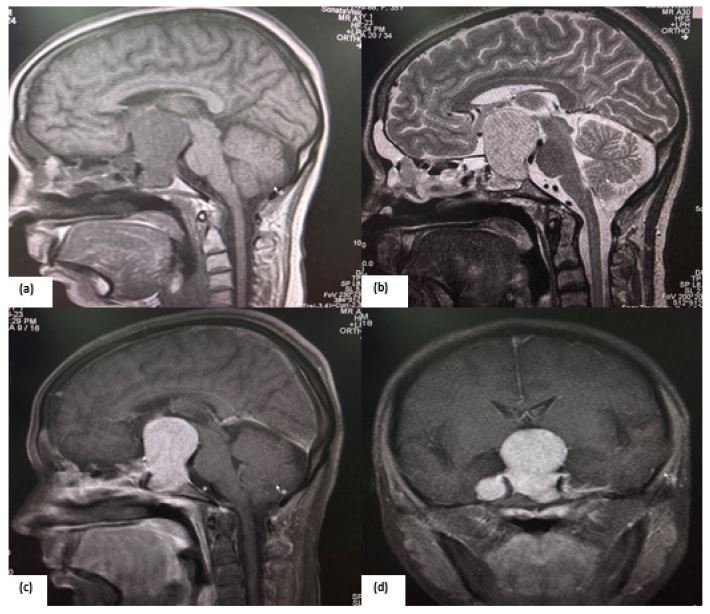
(a) T1 Sagittal non contrast MRI.
(b) T2 Sagittal non contrast MRI.
(c,d) T1 post Contrast PD FS Sequence sagittal and coronal images.
Declarations
Ethics approval and consent to participate: Not applicable.
Funding: None.
Conflict of interest: The authors declare no potential competing interests concerning the case, authorship and manuscript publication.
Patient consent for publication: Consent was obtained from the patient and his Guardian.
Availability of data and material: Some or all the data used to support the findings of the case report shall be made available by the corresponding author upon reasonable request.
Acknowledgement: Not applicable.