
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Columella fistula: A case report
Moujrid Sara*; Jabri Meriem; Bijou Walid; Oukessou Youssef; Rouadi Sami; Abada Reda; Roubal Mohamed; Mahtar Mohamed
Department of Otorhinolaryngology, 20 Août Hospital, Casablanca, Morocco.
*Corresponding Author : Moujrid Sara
Department of Otorhinolaryngology, 20 Août Hospital, Casablanca, Morocco.
Email: saramoujrid9@gmail.com
Received : Mar 21, 2024
Accepted : May 01, 2024
Published : May 08, 2024
Archived : www.jcimcr.org
Copyright : © Sara M (2024).
Abstract
Cysts and fistulas of the dorsum of the nose are rare. These malformations are strictly confined to the midline, extending from the columella to the glabella. Deep extension is possible, with contact with the leptomeningeal spaces. Imaging is performed to determine the deep extension and relationship of the malformation to the cribriform plate and the meninges and the presence of a frontal and/or nasal bone defect on CT scan, or of a transosseous canal with or without cyst on MRI, should raise suspicion of a dermal sinus cyst, and rapid surgical excision is indicated to avoid the complication the most feared: neuro-meningeal superinfection. Surgical excision is preferably carried out before the age of one year, due to the risk of infection, neurosurgical treatment is necessary if communication with the meningeal spaces is suspected. We present the case of a male child aged 4 years, with a history of neonatal suffering with notion of psychomotor delay and epileptic seizures. who presents a fistula at the level of the columella with discharge of pus in a context of dysmorphic syndrome. A brain scan showed the presence of a communication between the fistula and the anterior level of the skull base, then the patient was scheduled for excision of the fistula.
Keywords: Columella fistula; Naso-frontal fistula; Naso dermal sinus.
Citation: Sara M, Jabri M, Walid B, Youssef O, Sami R, et al. Columella fistula: A case report. J Clin Images Med Case Rep. 2024; 5(5): 3035.
Introduction
Naso-frontal fistulas, also known as Naso-Dermal Sinus Cysts (NDSC), are very rare and found in 1/20000 to 1/40000 births [1,2]. A true permanent portal of entry, it can be revealed by a locoregional and especially neuromeningeal infection, which makes this congenital malformation so serious. The most frequent are dermoid cyst-fistulas, nasal fossa gliomas and encephaloceles. They result from congenital anomalies of embryonic development, usually appearing as masses on the midline of the nose, anywhere between the glabella and columella. These patients are at risk of neuromeningeal infectious complications, due to the possibility of an intracranial connection, hence the need for early surgical treatment. Neuroimaging techniques are used to assess the existence of intracranial extension. reporting the case of a 4 year old child with a history of psychomotor delay with dysmorphic syndrome who presents with a columella fistula.
Case report
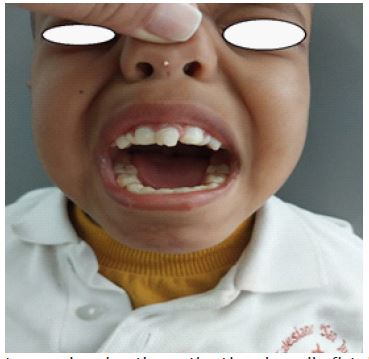
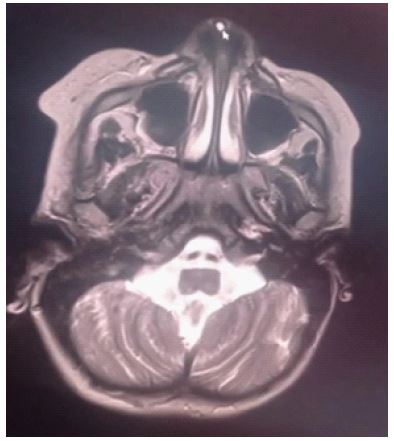
This is a 4-year-old male child, with a history of neonatal suffering following a poorly followed pregnancy, with notion of psycho-motor delay and epileptic seizures. He was referred to us from the pediatric department where he is followed following the observation by his pediatrician of a fistula at the level of the columella with pus coming out in a context of a dysmorphic syndrome (Figure 1). After having carried out the clinical examination, we requested a brain scan to look for a communication between the fistula and the base of the skull, indeed there was communication of the fistula with the anterior level of the skull, we completed the radiological assessment with an MRI which confirmed the presence of a columella fisula without endocranial extension (Figure 2), then the patient was scheduled for excision of the fistula. The chirurgical procedure consists of making an incision next to the cyst at the level of the columella, dissection step by step until the insertion of the cord at the level of the nasal bones, reaming facing the line uniting the nasal bones.
Discussion
Cysts and fistulas of the dorsum of the nose are rare. These malformations are strictly confined to the midline, extending from the columella to the glabella [2-4]. Occasionally, one or more hairs are present, centered on the fistula. Deep extension is possible, with contact with the leptomeningeal spaces. Imaging is systematically carried out preoperatively to determine deep extension and the malformation’s relationship with the cribriform lamina and meninges. Surgical excision is preferably performed before the age of one, due to the risk of infection, neurosurgical management is required if a communication with the meningeal spaces is suspected.
Among the various pathological theories proposed, the most widely accepted is that proposed by Grunwal in 1910 and later developed by Pratt [4-6].
Embryologically, between the frontal and nasal bones lies a membrane called phonticulus nasofrontalis [7-9]. Behind it, an extension of the dura mater insinuates itself. With development, this extension is enveloped by a bony canal whose entrance is called the foramen caecum, which eventually closes completely with growth. When it’s not the case, herniations of the cerebral envelopes occur, sometimes accompanied by cerebral parenchyma [10,11].
In fact, the development of mesoblastic tissue has stopped. Remnants of nervous tissue may remain in the same region, giving rise to gliomas, or ectodermal tissue forming dermoid cysts [11,12].
Gliomas, dermoid cysts and meningoencephaloceles are the differential diagnoses to be considered in the presence of a medial frontal malformation or malformation of the dorsum of the nose. Nasal gliomas are rare congenital tumors composed of heterotopic neuroglial tissue. Because of the risk of meningeal or ependymal communication, it is imperative to perform MRI and/or CT scans systematically in the presence of any congenital nasal median swelling [3,4]. Fernàndez P et al, reported five cases of cysts with dermoid fistulas and one meningoencephalocele that presented with recurrent meningitis. ENT examination revealed a polypoid mass in the nasal cavity, which was punctured, and study of the fluid obtained was compatible with CSF. One case was associated with a frontal hemangioma and another with mental retardation.
When faced with a mid-nasal mass, CT and high-resolution MRI are essential to define the extent and location of the mass and specify its intracranial-extradural extension [12,13]. When the foramen cecum is enlarged and the crista galli bifid this indicates intracranial involvement of the NDSC. Sessions described in its overview that the most proximal part often consists of a fibrous tract or stem. The histological assessment confirmed this finding. The MRI will provide more detail regarding the relationship of the lesion to the spinal parenchyma and dura mater.
However, definitive diagnosis of the lesion’s relationship with endocranial structures can only be made by surgical exploration [1,2,6,12,13]. During surgery, fibrous tracts in contact with the dura may be observed, without the relationship between the lesion and the dura being clearly demonstrated.
As of the surgical approaches, several approaches were suggested in different studies. To have a radical treatment of the NDSC it is necessary to expose the proximal end of the fistula. The simplest exposure to access the foramen cecum and crista galli is the vertical incision [7,13]. It is fundamental that facial skin growth may have influenced scar formation despite correct skin incisions. The risk of recurrent and serious preoperative fistula infection is present and can result in visible scarring [12,13].
Another surgical approach consists of exposing the dorsum of the nose and the foramen cecum based on a coronal transfrontal approach was proposed by Kellman et al. In their study, they recommended a coronal approach with osteotomy of the frontal bone. The subcranial approach provides excellent exposure, minimizes frontal lobe retraction, reduces the risk of cerebrospinal fluid leak, and achieves excellent cosmetic results [8,13-15].
Conclusion
Naso-dermal sinus cysts should be suspected in any child presenting with a nasal or nasofrontal cutaneous disruption from the glabella to the collumella, with or without fluid issue. Similarly, the presence of a frontal and/or nasal bone defect on CT scan, or a transosseous canal with or without cyst on MRI, should raise the suspicion of dermal sinus cysts, and prompt surgical excision is indicated to avoid the most dreaded complication: neuro-meningeal surinfection.
References
- Zheng Y, Ye B, Lv J, Xiang M. Progress of the diagnosis and treatment of congenital nasal dermoid sinus cysts. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2021; 35(2): 176‑80.
- Holzmann D, Huisman TAGM, Holzmann P, Stoeckli SJ. Surgical approaches for nasal dermal sinus cysts. Rhinology. 2007; 45(1): 31‑5.
- Fernández Pérez AJ, Burgos Sánchez AJ, Gras Albert JR. [Congenital lesions of the naso-frontal midline]. Acta Otorrinolaringol Esp. 2001; 52(5): 404‑8.
- Bigorre M. Kystes et fistules congénitaux de l’enfant. Annales de Chirurgie Plastique Esthétique. 2016; 61(5): 371‑88.
- Posnick JC, Bortoluzzi P, Armstrong DC, Drake JM. Intracranial nasal dermoid sinus cysts: computed tomographic scan findings and surgical results. Plast Reconstr Surg. 1994; 93(4): 745‑54, 755-756.
- Sessions RB. Nasal dermal sinuses--new concepts and explanations. Laryngoscope. 1982; 92(8 Pt 2 Suppl 29): 1‑28.
- Morimoto K, Takemoto O, Nishikawa M, Umegaki M, Nishino A. Nasal dermal sinus with a dermoid cyst. Pediatr Neurosurg. 2002; 36(4): 218‑9.
- Kellman RM, Goyal P, Rodziewicz GS. The transglabellar subcranial approach for nasal dermoids with intracranial extension. Laryngoscope. 2004; 114(8): 1368‑72.
- Thomas Karl Hoffmann, Marc Oliver Scheithauer, Fabian Sommer, Jörg Lindemann, Ernst-Johannes Haberl, Ulrike Friebe-Hoffmann, Marie-Nicole Theodoraki. Ann, Surgery of Anterior Skull Base Lesions in Children. Otol Rhinol Laryngol. 2017; 126(3): 245-253. doi: 10.1177/0003489416685321.
- R Locke 1, H KubbaJ. Unusual variants of midline nasal dermoid cysts: a series of three cases. Laryngol Otol. 2012; 126(1): 83-7. doi: 10.1017/S0022215111002891.
- G Cotin, H Muler, S Baux, J M Basset. Midline congenital fistulas of the nose. Fourteen cases. Ann Otolaryngol Chir Cervicofac. 1979; 96(10-11): 733-43.
- Katharina Moratin, Philipp-Sebastian Koch, Johannes Benecke, Azadeh Orouji, Corinne Bauer, Jörg Faulhaber, Wolfgang Koenen, Moritz Felcht J Cutan. Reconstruction of Nasal Defects With Dermal Skin Substitutes-A Retrospective Study of 36 Defects. Med Surg. 2019; 23(4): 413-420.
- Katherine E Kormanik, Edward T Bersu, Michael L Bentz. Dermoid sinus and cyst of the lip. J Craniofac Surg. 2006; 17(1): 162-6.
- J A Lehman Jr Br. Secondary repair of bilateral cleft lip deformities. J Plast Surg. 1976; 29(2): 116-21.
- Eelam Adil, Reza Rahbar. Paediatric nasal dermoid: evaluation and management. Curr Opin Otolaryngol Head Neck Surg. 2021; 29(6): 487-491.