
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 5
“What’s left after the drama?”- Emergency obstetric hysterectomies’ macroscopic images
Karamaroudis Stefanos1*; Papageorgiou Thomas1; Alexiou Nikolaos1; Papakonstantinou Eleni2; Katopodis Dionisios1; Rokkos Theodoros1
1Department of Obstetrics and Gynecology, General Hospital of Elefsis “Thriassio”, Elefsis, Attiki, Greece.
2Department of Pathology, General Hospital of Elefsis “Thriassio”, Elefsis, Attiki, Greece.
*Corresponding Author : Karamaroudis Stefanos
Department of Obstetrics and Gynecology, General Hospital of Elefsis “Thriassio”, Elefsis, Attiki, Greece.
Email: stefanos.karamaroudis@gmail.com
Received : Apr 15, 2024
Accepted : May 01, 2024
Published : May 08, 2024
Archived : www.jcimcr.org
Copyright : © Stefanos K (2024).
Abstract
Postpartum Haemorrhage (PPH) is the leading cause of maternal mortality world-wide. Many times, the only solution is surgical intervention by performing a caesarean (or emergency obstetric) hysterectomy. These cases are the most dramatic expression of the so called “miracle of childbirth” with disastrous outcomes for the mother and the neonate. With literary mood we publish three macroscopic images of pathologic specimens after caesarean hysterectomies.
Keywords: Emergency Obstetric Hysterectomy; Caesarean Hysterectomy; Hysterectomy Histopathology.
Abbreviations: CS: Caesarean Section; GA: Gestational Age; ICU: Intensive Care Unit; Rbcs: Red Blood Cells; EOH: Emergency Obstetric Hysterectomy; DIC: Disseminated Intravascular Coagulation.
Citation: Stefanos K, Thomas P, Nikolaos A, Eleni P, Dionisios K, et al. “What’s left after the drama?”- Emergency obstetric hysterectomies’ macroscopic images. J Clin Images Med Case Rep. 2024; 5(5): 3036.
Description
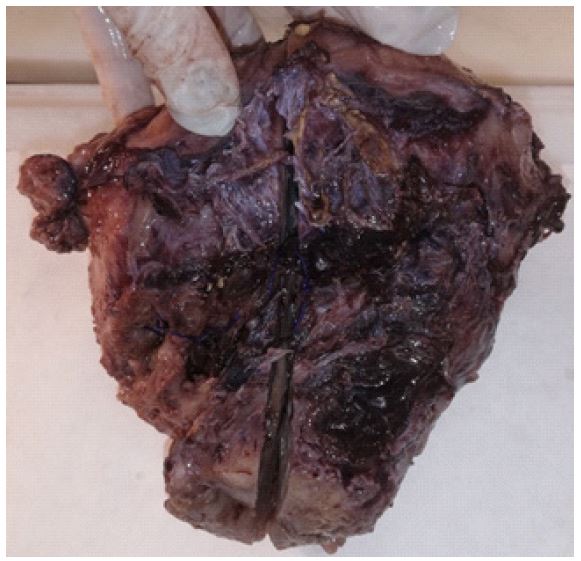
We report three cases of EOH, and we present one macroscopic image from each pathology specimen to point out the specific issues that arose in each patient.
Case 1
A hospitalized due to COVID-19 respiratory failure, gravida two, GA 33w+2, 42-years-old woman, started to have tetanic uterine contractions and soon fainted. She was severely unstable and transferred in hemorrhagic shock in the operating room. After a successful delivery of liveborn singleton through massive hemoperitoneum, a catastrophic uterus rupture was apparent with bladder cyst rupture. The woman was transferred to the ICU after a hysterectomy and discharged after two months of hospitalization and an odyssey journey through postoperative and hospital acquired infections, DIC and other complications.
Case 2
A 37-year-old woman, gravida six, 37w+2 of GA, with five previous CS and limited prenatal care presented in the emergency department reporting minor vaginal bleeding. She was assessed by ultrasound and was diagnosed with a complete placenta praevia from the posterior uterine wall. After an uncomplicated delivery of a liveborn singleton efforts made to manually remove the placenta and preserve the uterus as this was the patient’s will. Unfortunately, the placenta was strongly adhered to the uterus wall and after its removal massive bleeding started. The patient quickly became unstable, and an EOH was performed. She discharged in good condition after five days.

Case 3
A 36-year-old woman underwent a planned CS at a GA of 38w+3 due to two previous CS. After delivery of a liveborn singleton and continuous suturing of the hysterotomy, the lower segment of the anterior uterus wall was presented oedematose and with excessive myometrial atony. Vaginal bleeding and bleeding through the sutured hysterotomy were displayed and despite uterotonics and tranexamic acid the patient became unstable. Emergency EOH was performed, and the patient was transferred stable in the ward been transfused with only two units of packed RBCs.

Declarations
Acknowledgments: We would like to thank the three patients for allowing us to share these clinical images.
Disclosure: The authors declare no potential conflict of interest.
References
- Shahid R, Abbas H, Mumtaz S, et al. Emergency Obstetric Hysterectomy, the Histopathological Perspective: A Cross-Sectional Study from a Tertiary Care Hospital. Cureus. 2020; 12(7): 9094. Published 2020 Jul 9. doi:10.7759/cureus.9094.