
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 5
Evaluation of orofacial therapies on saliva of patients with down syndrome and obstructive sleep apnea
Mônica Fernandes Gomes1,2*; Renata Dos Santos Nudi1; Lilian Chrystiane Giannasi1,2; Marignês Theotonio Dos Santos Dutra1; Cristiane Yumi Koga-Ito1,2; Bruna Dicieri Pereira1; José Benedito Oliveira Amorim1,2; Sigmar De Mello Rode; Luis Vicente Franco De Oliveira3; Miguel Angel Castillo Salgado1,2
1Institute of Science and Technology, Campus of São José Dos Campos, São Paulo State University (UNESP), Brazil.
2Center of Bioscience Applied for Patients with Special Health Care Needs (Known as CEBAPE), Brazil.
3Centro Universitário de Anapolis - UniEvangelica-GO, Brazil.
*Corresponding Author : Mônica Fernandes G
Institute of Science and Technology, Campus of São José dos Campos, São Paulo State University (known as UNESP), Engenheiro Francisco José Longo Avenue, number 777, ZIP Code: 12.245-000, São José dos Campos, São Paulo, Brazil.
Tel: 055-12-3947-9086 & 055-12-99715-1009;
Email: monica.gomes@unesp.br
Received : Dec 19, 2023
Accepted : May 02, 2024
Published : May 09, 2024
Archived : www.jcimcr.org
Copyright : © Gomes MF (2023).
Abstract
Objective: Assess the effects of surface Neuromuscular-Electrical Stimulation (sNMES), Masticatory-Device with Hyperboloid (MDHB), and mandibular-advancement-intraoral-appliance (OAm) on salivary parameters in patients with Down Syndrome and Obstructive Sleep Apnea (DS-OSA).
Design: Among 23 adults patients with DS-OSA, 18 patients underwent the three therapies for 60 days who were divided into three groups: sNME (n=7), MDHB (n=4), and OAm (n=7). Before and after the therapies, saliva tests were done, including Salivary Flow Rate (SFR), pH value (pH), buffering capacity (TC), morning (mSC) and night (nSC) salivary cortisol, and identification of Pseudomonas aeruginosa (Pa) species.
Results: Although the SFR had reduced values, the saliva production was increased after the therapies. The statistical difference was only found in OAm (p< 0.022). There was statistical difference in sNME (p< 0,034). Although no statistical difference was found in TC, the normality values were reached in 29% to OAm and MDHB and in 14% to sNME. nCS levels was only statistically increased in sNME (p< 0,036) and between the sNME and OAm (p< 0.0058) therapies, without affecting their normality values. No Pa species were found.
Conclusion: OAm and DMHB mitigated the salivary reduction in patients with DS-OSA; however, sNME improved the saliva quality. Susceptibility to stress disorders was identified in the OAm in night period. No risk for aspiration pneumonia, before the therapies, and no congenital anomalies of major salivary glands were detected.
Keywords: Down syndrome; Obstructive sleep apnea; Saliva; Electric stimulation therapy; Activator appliances.
Abbreviations: sNME: Surface Neuromuscular Electrical Stimulation; MDHB: Masticatory Device With Hyperboloid; OAm: Mandibular Advancement Oral Appliance; SFR: Salivary Flow Rate; BC: Buffering Capacity; mSC: Morning Salivary Cortisol; nSC: Night Salivary Cortisol
Citation: Gomes MF, Nudi RDS, Giannasi LC, Dutra MTDS, Koga-Ito CY, et al. Evaluation of orofacial therapies on saliva of patients with down syndrome and obstructive sleep apnea. J Clin Images Med Case Rep. 2023; 5(5): 3038.
Introduction
Down Syndrome (DS) is caused by an extra copy of chromosome 21 (Trisomy for human chromosome 21), Hsa21, and its main phenotypic aspects are intellectual disability in varying degrees, short stature, generalized muscular hypotonia, craniofacial dysmorphia, heart congenital, mainly septal defects, and immune system deficit [1,2]. Other comorbidities may be associated with this condition, such as: Gastrointestinal and urogenital problems (cryptorchidism and hypospadias), as well as decreased audio-sensory function, respiratory disorders including Obstructive Sleep Apnea (OSA), thyroid dysfunction, leukemia, neuropathy [3,4]. Some alterations of the stomatognathic system are associated with DS, including periodontal diseases (60 to 100% of cases), fissures on the surface of the lips associated with mouth breathing, bruxism, dental anomalies, malocclusion, temporomandibular dysfunction, labial commissure with descending angle, eversion of the lower lip and, in particular, dry mouth or xerostomia, craniofacial changes and relative macroglossia [5,6]. Although not a recognized manifestation of DS, agenesis, or hypoplasia of major salivary glands, particularly highlighting the parotid and submandibular glands, can be found [7,8]. This can result in expressive alterations in glandular structures and physicochemical properties of salivary secretion in these individuals. Studies describe that the parotid, submandibular and sublingual glands produce serous, sero-mucosal and mucosal saliva respectively [7,9]. It should be noted that serous saliva is essential in taste and swallowing, as well as mucous saliva acts as a lubricant, helping oral comfort [1,9]. The human salivary glands are 18 morphologically developed in intrauterine life, with the parotid glands from the 4th to the 6th week, the submandibular glands from the 6th week and the sublingual glands and minor glands from the 8th to 12th week of embryonic life [10]. Their growths continue to occur during childhood due to the proliferation of parenchymal cells. In general, the maturation process is slower in individuals with DS when compared to individuals without the syndrome. Given the above, the aim of this study was to evaluate the effects of neuromuscular electrostimulation therapies and intraoral biomechanical devices on the physicochemical and microbiological properties of saliva in patients with DS and OSA. Furthermore, we investigated the morphological aspects of the major salivary glands to diagnose possible structural disorders in these individuals.
Material and methods
This clinical trial was registered in the World Health Organization Universal Trial (UTN; number U1111-1201-3155) and Registro Brasileiro de Ensaios Clínicos (ReBEC; number RBR-3qp5np). It was also approved by the Ethics Committees on Human Research of the Institute of Science and Technology of the São Paulo State University, IST-UNESP (CEPh/CAAE process number 64 173 616.4.0000.0077). The follow, the informed consent form was also signed by the legally responsible person, after the volunteers’ approval.
Subjects
Initially, 23 adults with DS and OSA, of both the genders, with age range from 19 to 40 years old, were invited to participate in this study. Among them, 18 patients concluded the purpose therapies, and they were divided into 3 therapeutics groups: sNME (n=7; patients treated with surface neuromuscular electrostimulation), MDHB (n=4; patients treated with masticatory device with hyperboloid), and OAm (n=7, patients treated with mandibular advancement oral appliance). The inclusion criteria were satisfactory general and oral health, partial preserved cognitive function to understand and to respond verbal commands to perform the therapies. Also, the presence of positive diagnosis of Obstructive Sleep Apnea (OSA), with Apnea/Hypopnea Index (AHI) >5.0/h The exclusion criteria were patients with psychiatric disorders, tooth mobility, absence of posterior teeth, use of continuous drugs that may alter the salivary flow; in additional, patients underwent the speech therapy, the physiotherapy, and orthodontic or functional orthopedic treatment, at least 6 months prior to the beginning of this study.
Orofacial therapeutic stimulation
Surface Neuromuscular Electrostimulation (sNME): The sNME equipment was Neurodyn II (IBRAMED - Indústria Brasileira de Equipamentos Médicos EIRELI, Amparo, São Paulo, Brazil), with 4 channels, that allows the application of electric currents, via electrodes, in direct contact with the patient’s face for neuromuscular dysfunctions therapy. The following parameters were employed: pulse frequency of 50 Hz, pulse width of 300 μs, and on/off ratio of 10 seconds of stimulation and 30 seconds of rest for 20 minutes per session. The intensity of electrical current was determined for each patient, according to the movement amplitude of the temporal and masseter muscles and her/his tolerance. The patients underwent the two weekly 20-minute sessions of sNME of the masseter and temporalis muscles for 8 weeks, a total of 16 sessions.
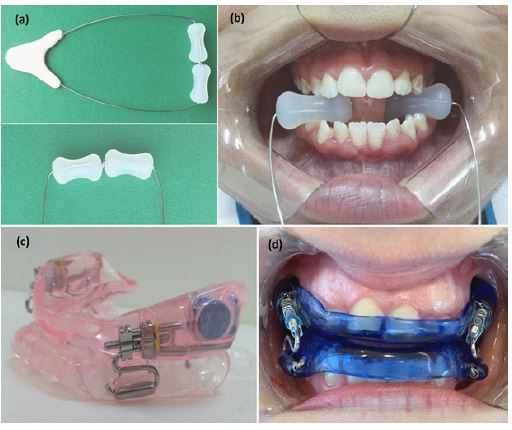
Masticatory Device with Hyperboloid (MDHB): A Masticatory Device with Hyperboloid (MDHB) was used to strengthen, to stimulate, and to modulate the masticatory muscles. This device consists of two hyperboloids (HB, active tip; Hiperboloide; M.C. CHEIDA - ME, São Paulo, Brazil) and a support rod. This rod is an assistive technology instrument of which was developed for people with neuropsychomotor impairments, as peoples with Down syndrome (UNESP Innovation Agency, Invention Communication, code: 18CI038). The HB was positioned between the occlusal surfaces of posterior teeth; then, the patient slowly bit them for 3 seconds and released for 1 seconds. These rhythmic movements were done for 5 minutes, six times per day, in a period of 2 consecutive months. It is noteworthy that the periods to perform the masticatory exercises were 10h-12h AM, 14h-16h PM, and 18h-20h PM. After the masticatory exercises, the patients or caregivers cleaned the MDHB with running water, wiped it with paper towel, and then, stored it at room temperature. To preserve this apparatus, some cares were recommended, such as: to avoid bite the support rod; to use no abrasives, chemical products, or boiling water for cleaning; and no remove the hyperboloid inserted in the steel wire. If there was complain of pain, the patients and/or caregivers were instructed to interrupt this therapy (Figures 1a and 1b).
Mandibular Advancement Oral Appliance (OAm): To treat Obstructive Sleep Apnea (OSA), a mandibular advancement Oral Appliance (OAm) was used. It was done in according to the studies of [11,12]. The OAm was only used during the sleep for a continuous two-month period. The OAm titration was slowly performed with increments of 0.5-1.0 mm, weekly or biweekly, respecting the patients’ physiologic limitations. Furthermore, a thermosensitive microchip (Theramon Microsensor; Lianka Comércio e Representações Ltda EPP, São Paulo, Brazil) was attached to the OAm to monitor the therapeutic adhesion’s patients (Figures 1c and 1d).
Protocol of study
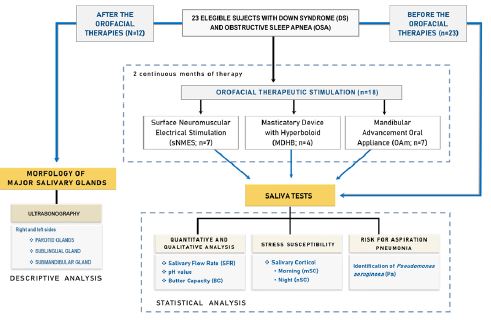
To understand our methodology, a flowchart was done to illustrate the study design, investigating the influences of orofacial therapeutic stimulation on saliva of patients with DS and OSA (Figure 2).
Laboratorial analysis of salivary parameters
Initially, saliva was stimulated by using a HB (hyperboloid) and then, the samples were collected into a sterile cup for 15 min, between 8 and 10 AM and 9 and 11 PM. The first saliva sample was discarded to ensure the fidelity of subsequent microbiological analysis. Following this, salivary test was done to assess the microbiological and physicochemical properties of saliva, including salivary flow rate (SFR; mL/min), salivary pH, buffer capacity (BC; pH value), and concentration levels of morning (mSC, μg/dL) and night (nSC, μg/dL) salivary cortisol. Furthermore, the identification of Pseudomonas aeruginosa species was done to assess risk for occurrence of aspiration pneumonia. The protocols of the salivary test and the reference values are detailly described in the study [11-13]. It is important to emphasize that the SC levels were analyzed in according with the age and gender, using the reference values determined by the Salimetrics’ manufacturer of the Expanded Range High Sensitivity Salivary Cortisol Enzyme Immunoassay Kit.This laboratorial analysis was performed at the Center of Bioscience Applied for Patients with Special Health Care Needs, known as CEBAPE (https://www.ict.unesp.br/#!/sobre-o-ict/depto-ensino/biociencias-e-diagnostico-bucal/laboratorios/cebape). The results were evaluated using the following statistical tests: Wilcoxon signed-rank test, Kruskall-Wallis test, and Dunn’s multiple comparison test. The Wilcoxon signed-rank test showed the correlation among the therapies and the exploratory variables of salivary parameters; while the Kruskall-Wallis test associated with the Dunn’s test were used to compare the three therapies with the salivary parameters.
Ultrasonography of major salivary glands
The major salivary glands, including the parotid, sublingual submandibular glands, in both sides, were examined thought the Ultrasonography (USG) and its analysis was just descriptive. The Doppler ultrasound exam was recommended when the patients had any structural disorder of gland. The limitations of this study are related to the pandemic outbreak of COVID-19 that jeopardized the completion of some therapies. It is important to highlight that this population is group risk for opportunist infections due to the deficit of the immune system. Therefore, this fact strongly interfered in the low number of the subjects who could carry out the therapies and its analysis.
Results
Salivary parameters
The results of the saliva tests and their interpretation criteria, before and after the therapies, are demonstrated in the (Table 1). About the SFR, all patients had reduced salivary flow, before and after the therapies. The hyposalivation, found in the P6sNME, P3MDHB, P4MDHB, and P2OAm, was eliminated in the post-therapies; however, these patients remained the decrease saliva production. The OAm therapy promoted a slight increase in saliva production in 100% of the patients, followed by the MDHB (75% of patients), and sNME (43% of patients). The pH value showed no change in normality, before and after the therapies with MDHB and OAm. In contrast, after the sNME therapy, the high pH value of the P3sNME reached the normal value. After the therapies, there was an increase of BC in the following proportions of patients: 71% patients treated with sNME (5/7 patients), 50% of patients treated with MDHB (2/4 patients), and 43% patients treated with OAm (3/7 patients). Moreover, the BC values were changed from borderline to normal values in the patients: P3sNME, P4sNME, P1MDHB, P3MDHB, P4AIOm, and P5AIOm (6/18 patients). On the other hand, the P2sNME (1/18 patients) had altered BC, ranging from normal to borderline values.
In post-therapies, the increased levels of mSC and nSC were found in the following proportions of patients: 50% and 71% of patients to OAm, 50% and 50% of patients to MDHB, and 43% and 0% of patients to sNME, respectively. After the therapies, the susceptibility to stress disorders was detected in the following patients: P4sNME and P2MDHB (morning period) and P2OAm, P3OAm, and P4OAm (night period). It is important to highlight that we identify mSC levels highly elevated in the P1sNME, before and after the therapy. Regarding the identification of Pseudomonas aeruginosa, no patient was positive before the three therapies. Given this fact, it was presumed the irrelevance to repeat this analysis after the three therapies, since our patients showed good general and oral health during the development of this study. Statistically, comparing the results of the saliva tests before and after the therapies, the Wilcoxon test revealed that there was a statistically significant difference in the SFR to OAm therapy (p=0.0225), pH value to sNME therapy (p=0.0346), and nSC levels to NMES therapy (p=0.0360). These findings are demonstrated in the (Table 2). Also, Kruskall-Wallis test and Dunn’s multiple comparison test showed statistical significance in the variations of the nCS levels between the therapies with NMES, MDHB, and NMES (p=0.0223); however, when we compare these three therapies, we can find a significant difference (p=0.0058) between the therapies with sNME and OAm (Tables 3 and 4).
Ultrasonography of major salivary glands
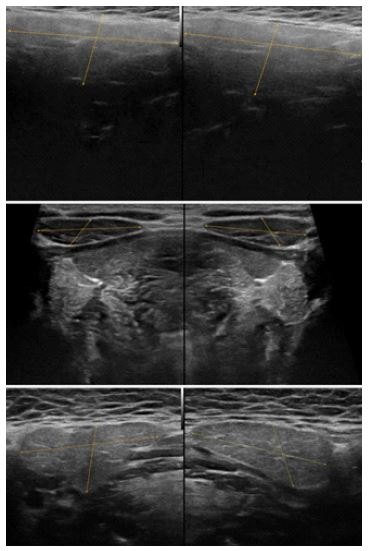
Among the 23 patients, 12 patients underwent the UltraSound exam (USG) in the regions of major salivary glands, including the parotid, sublingual, and submandibular glands, on both sides. The areas adjacent to these structures were also analyzed.
The images showed that the major salivary glands were present in all patients. Eleven patients had major salivary glands with normal morphological aspects; in contrast, one patient (P5MDHB) had alteration in both the parotid glands, suggesting chronic sialadenitis. Concerning the adjacent areas, enlarged cervical lymph node were found in the P6sNME, P2OAm, and P3OAm. Furthermore, the images suggested the presence of Inflammation of thyroid gland in the P3sNME (Table 5 and Figure 3).
It is important to highlight that 11 patients did not perform the ultrasound imaging due to intercurrences reported by the caregivers, such as: patient’s unsatisfactory general health, recurrent opportunistic infections during the study because of the immune system deficit, and difficulty of public transportation on the day of the scheduled exam.
Table 1: Comparison between the results of the saliva parameters in patients with DS, before (n=23) and after (n=18) therapies with sNME (n=7), MDHB (n=4), and OAm (n=7).
| Patients | Ages (years) | Gender | SFR | (%) of ↑ | pH | (%)of ↑ |
BC | (%) of ↑ |
mSC | (%)of ↑ |
nSC | (%)of ↑ |
PA | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Before | After | Before | After | Before | After | Before | After | Before | After | Before | After | ||||||||||||||||||
| sNME | 43% | 14% | 71% | 43% | 0% | ||||||||||||||||||||||||
| P1* | 21 | M/td> | 0.3 | ↓ | 0.4 | ↓ | ↑ | 7.6 | N | 6.9 | N | ↓ | 5.5 | N | 6.1 | N | ↑ | 0.984 | ↑ | 7.404 | ↑ | ↑ | 0.058 | N | 0.028 | N | ↓ | Negative | (▲) |
| P2 | 18 | M | 0.2 | ↓ | 0.2 | ↓ | (~) | 6.8 | N | 5.2 | ↓ | ↓ | 5.7 | N | 4.9 | L | ↓ | 0.117 | N | 0.039 | N | ↓ | 0.097 | N | 0.018 | ↓ | ↓ | Negative | |
| P3 | 20 | F | 0.5 | ↓ | 0.5 | ↓ | (~) | 8.1 | ↑ | 5.6 | N | ↓ | 4.1 | L | 5.3 | N | ↑ | 0.683 | N | 0.074 | ↓ | ↓ | 0.045 | N | 0.023 | ↓ | ↓ | Negative | |
| P4 | 26 | M | 0.2 | ↓ | 0.2 | ↓ | (~) | 7.1 | N | 6.3 | N | ↓ | 5.0 | L | 5.6 | N | ↑ | 0.106 | ↓ | 0.796 | ↑ | ↑ | 0.844 | ↑ | 0.022 | ↓ | ↓ | Negative | |
| P5 | 25 | F | 0.3 | ↓ | 0.6 | ↓ | ↑ | 6.5 | N | 6.7 | N | ↑ | 6.1 | N | 6.2 | N | ↑ | 0.088 | ↓ | 0.106 | ↓ | ↑ | 0.106 | N | 0.017 | ↓ | ↓ | Negative | |
| P6 | 21 | M | 0.1 | ● | 0.5 | ↓ | ↑ | 6.8 | N | 6.0 | N | ↓ | 4.7 | L | 4.9 | L | ↑ | 0.073 | ↓ | 0.041 | ↓ | ↓ | 0.100 | N | 0.089 | N | ↓ | Negative | |
| P7 | 22 | F | 0.6 | ↓ | 0.6 | ↓ | (~) | 7.1 | N | 6.7 | N | ↓ | 5.2 | N | 5.1 | N | ↓ | 0.129 | ↓ | 0.039 | ↓ | ↓ | ■ | 0.022 | ↓ | - | Negative | ||
| P8 | 28 | M | 0.3 | ↓ | (/) | - | 7.9 | ↑ | (/) | - | 5.4 | N | (/) | - | 0.196 | N | (/) | - | 0.061 | N | (/) | - | Negative | ||||||
| P9 | 29 | M | 0.1 | ↓ | (/) | - | 6.2 | N | (/) | - | 5.2 | N | (/) | - | 0.108 | ↓ | (/) | - | 0.055 | N | (/) | - | Negative | ||||||
| DMHB | 75% | 25% | 50% | 50% | 50% | ||||||||||||||||||||||||
| P1 | 25 | M | 0.5 | ↓ | 0.5 | ↓ | (~) | 6.5 | N | 6.6 | N | ↑ | 4.9 | L | 5.1 | N | ↑ | 0.528 | N | 0.178 | N | ↓ | 0.191 | N | 0.021 | ↓ | ↓ | Negative | (▲) |
| P2 | 20 | M | 0.2 | ↓ | 0.4 | ↓ | ↑ | 7.8 | N | 7.5 | N | ↓ | 5.8 | N | 5.2 | N | ↓ | 0.050 | ↓ | 1.302 | ↑ | ↑ | 0.054 | N | 0.106 | N | ↑ | Negative | |
| P3 | 19 | M | 0.1 | ● | 0.6 | ↓ | ↑ | 7,3 | N | 6.9 | N | ↓ | 4.3 | L | 5.1 | N | ↑ | 0.132 | N | 0.047 | N | ↓ | 0.174 | N | 0.031 | N | ↓ | Negative | |
| P4 | 18 | M | 0.1 | ● | 0.4 | ↓ | ↑ | 6.3 | N | 6.1 | N | ↓ | 6.7 | N | 5.9 | N | ↓ | 0.073 | N | 0.177 | N | ↑ | 0.093 | N | 0.142 | N | ↑ | Negative | |
| P5 | 19 | M | 0.2 | ↓ | (/) | - | 7.4 | N | (/) | - | 6.1 | N | (/) | - | 0.215 | N | (/) | - | 0.050 | N | (/) | - | Negative | ||||||
| P6 | 18 | M | 0.3 | ↓ | (/) | - | 7.0 | N | (/) | - | 5.6 | N | (/) | - | 0.138 | N | (/) | - | 0.056 | N | (/) | - | Negative | ||||||
| P7 | 24 | M | 0.5 | ↓ | (/) | - | 7.5 | N | (/) | - | 5.4 | N | (/) | - | 0.076 | ↓ | (/) | - | 0.136 | N | (/) | - | Negative | ||||||
| OAm | 100% | 43% | 43% | 50% | 71% | ||||||||||||||||||||||||
| P1 | 18 | F | 0.5 | ↓ | 0.8 | ↓ | ↑ | 7.1 | N | 6.8 | N | ↓ | 5.2 | N | 5.2 | N | (-) | 0.444 | N | 0.015 | ↓ | ↓ | 0.039 | N | 0.058 | N | ↑ | Negative | (▲) |
| P2 | 18 | F | 0.1 | ● | 0.2 | ↓//td> | ↑ | 6.3 | N | 6.7 | N | ↑ | 4.7 | L | 4.5 | L | ↓ | 0.382 | N | IS | - | 0.054 | N | 0.301 | ↑ | ↑ | Negative | ||
| P3 | 29 | F | 0.4 | ↓ | 0.6 | ↓ | ↑ | 6.8 | N | 7.1 | N | ↑ | 5.3 | N | 6.2 | N | ↑ | 0.254 | ↓ | 0.023 | ↓ | ↓ | 0.072 | N | 0.965 | ↑ | ↑ | Negative | |
| P4 | 18 | F | 0.2 | ↓ | 0.3 | ↓ | ↑ | 6.7 | N | 6.2 | N | ↓ | 5.0 | L | 5.6 | N | ↑ | 0.087 | N | 0.328 | N | ↑ | 0.046 | N | 0.467 | ↑ | ↑ | Negative | |
| P5 | 27 | F | 0.2 | ↓ | 0.4 | ↓ | ↑ | 7.3 | N | 6.8 | N | ↓ | 4.6 | L | 5.1 | N | ↑ | 0.130 | ↓ | IS | - | 0.035 | N | 0.023 | ↓ | ↓ | Negative | ||
| P6 | 18 | F | 0.2 | ↓ | 0.4 | ↓ | ↑ | 7.6 | N | 7.2 | N | ↓ | 5.3 | N | 5.3 | N | (-) | 0.172 | N | IS | - | 0.044 | N | 0.035 | N | ↓ | Negative | ||
| P7 | 23 | F | 0.4 | ↓ | 0.8 | ↓ | ↑ | 7.1 | N | 7.3 | N | ↑ | 7.1 | N | 6.8 | N | ↓ | 0.081 | ↓ | 0.101 | ↓ | ↑ | 0.023 | ↓ | 0.165 | N | ↑ | Negative | |
Table 2: Probability value of association between the categorical variable in each therapy and the exploratory variables of the salivary parameters using the Wilcoxon signed-rank test.
| Salivary parameters | sNME | MDHB | OAm | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| V | Expected value | Variance | p-value | V | >Expected value | Variance | p-value | V | Expected value | Variance | p-value | |
| SFR | 0 | 5.0000 | 7.5000 | 0.1003 | 0 | 3.0000 | 3.5000 | 0.1814 | 0 | 14.0000 | 35.0000 | 0.0225 |
| pH value | 27 | 14.0000 | 35.0000 | 0.0346 | 9 | 5.0000 | 7.5000 | 0.2012 | 20 | 14.0000 | 35.0000 | 0.3525 |
| BC | 7 | 14.0000 | 35.0000 | 0.2719 | 5 | 5.0000 | 7.5000 | 1.0000 | 8 | 14.0000 | 35.0000 | 0.3525 |
| mSC | 14 | 14.0000 | 35.0000 | 1.0000 | 4 | 5.0000 | 7.5000 | 0.8551 | 6 | 5.0000 | 7.5000 | 0.8551 |
| nSC | 21 | 10.5000 | 22.7500 | 0.0360 | 7 | 5.0000 | 7.5000 | 0.5839 | 6 | 14.0000 | 35.0000 | 0.0759 |
* The significance level is p-value< 0,05 (α=0.05).
Table 3: Probability value of the association between the three therapies and the exploratory variables using Kruskal-Wallis test.
| Kruskal-Wallis test | sNME vs MDHB vs Oam | ||||
|---|---|---|---|---|---|
| SFR | pH value | BC | mSC | NSC | |
| K (observed value) | 0.1733 | 4.8195 | 0.4916 | 2.0286 | 7.6084 |
| K (Critical value) | 5.9915 | 5.9915 | 5.9915 | 5.9915 | 5.9915 |
| p-value | 0.9170 | 0.0898 | 0.7821 | 0,3627 | 0.0223 |
* The significance level is p< 0.05 (α=0.05).
Table 4: Paired multiple comparisons using Dunn’s test, after three therapies.
| Sample | Frequency | R-sum | R-mean | Groups | |
|---|---|---|---|---|---|
| sNME (nSC) | 7 | 38.5000 | 5.5000 | A | |
| MDHB (nSC) | 4 | 39.0000 | 9.7500 | A | B |
| OAm (nSC) | 7 | 93.5000 | 13.3571 | B | |
| p-value | |||||
| sNMS (nSC) | MDHB (nSC) | OAm (nSC) | |||
| sNME (nSC) | 1 | 0.2036 | 0.0058 | ||
| MDHB (nSC) | 0.2036 | 1 | 0.2805 | ||
| OAm (nSC) | 0.0058 | 0.2805 | 1 | ||
* The significance level is p< 0.05 (α=0.05).
Table 5: Descriptive analysis of ultrasound exam of the major salivary glands.
| Pacients | Description | Suggestive Diagnosis |
|---|---|---|
| P3sNME | Parotid and submandibular glands of normal dimensions, regular contours, and normal gland echotexture; and absence of enlarged cervical lymph node. Thyroid gland showed heterogeneous parenchy- ma, suggesting thyroiditis. | Normal major salivary glands; and Inflammation of thyroid gland |
| P4sNME | Parotid, sublingual, and submandibular glands of normal dimensions, contours, and echotexture; and absence of enlarged cervical lymph node. | Normal major salivary glands |
| P5sNME | Parotid, sublingual, and submandibular glands of normal dimensions, contours, and echotexture. | Normal major salivary glands |
| P6sNME | Parotid, sublingual, and submandibular glands of normal dimensions, contours,and echotexture; and a hypoechoic lymph node with regular contours was noted at the nodal level IIA (left side), exhibiting regular contours and size of 1.9 x 0.6 x 1.0 cm. | Normal major salivary glands; and enlarged cer- vical lymph node (left side). |
| P7sNME | Major salivary glands showed normal shape, contours, echotexture, and dimen-sions; moreover, there was absence of cystic or solid expansive lesion inside these glands. | Normal major salivary glands |
| P1MDHB | Parotid, sublingual, and submandibular glands of normal dimensions, contours, and echotexture; and absence of enlarged cervical lymph node. | Normal major salivary glands |
| P3MDHB | Parotid, sublingual, and submandibular glands of normal dimensions, contours, and echotexture; and absence of enlarged cervical lymph node. | Normal major salivary glands |
| P4MDHB | Parotid, sublingual, and submandibular glands of normal dimensions, contours, and echotexture; and absence of enlarged cervical lymph node. | Normal major salivary glands |
| P5MDHB | Parotid glands with heterogeneous texture and reduced echogenicity; submandibular and sublingual glands of normal shape, contours, echotexture, and dimensions absence& of cystic or solid expansive lesion inside the salivary glands and adenopathy in the different cervical chains. | Normal lingual andsubman- dibular salivary glands; and sug- gestive of chronic sialadenitis of the parotid salivary glands |
| P2OAm | Parotid, sublingual, and submandibular glands of normal dimensions, contours, and echotexture; absence of enlarged cervical lymph node; and a hypoechogenic lymph node was noted at the nodal level IIA (right side),exhibiting regular contours, preserved fatty hilum,absence> of calcifica- tions, and sizeof 1.8 x 0.9 cm. | Normal major salivary glands; and enlarged cer- vical lymph node (right side) |
| P3OAm | Parotid, sublingual, and submandibular glands of normal dimensions, contours, and echotexture. A solid and hypoecho- genic nodule was identified in the right submandibular space in intimate contact with the submandibular gland, showing regular contours, well-defined limits, withoutvascularization on Doppler exam, and size of1.3 x 0.8 x 1.2 cm. | Normal majorsalivary glands; and enlarged cer- vical lymph node (right side) |
| P5OAm | Parotid, sublingual, and submandibular glands of normal dimensions, contours, and echotexture. No sign of ductal dilata- tion was evidenced in these structures; and adjacent lymph nodes showed no abnormality. | Normal major salivary glands |
Discussion
The oral hygiene is unsatisfactory in people with DS due to their cognitive deficits, leading to accumulation of dental biofilm and debris. This condition become them more susceptible to caries and periodontal diseases. Another factor is how the homeostasis of the physical-chemical and microbiological properties of saliva can favor the general and oral health, especially in DS. Thus, we consider the saliva as an important biological vehicle of study to equalize the influence of orofacial therapeutic stimulation on saliva of patients with DS and OSA. The saliva test has been effective and accurate for individuals with neuro psychomotor disabilities, as DS, such as: safe, easy handling, comfortable and non-invasive method; accessible to repeat; and minimal risk of tampering. Our results showed that the SFR was reduced before and after the proposed therapies, agreeing with the studies of [12]. We hypothesize that this quantitative alteration could occur due to the dysfunction of the production mechanism of saliva caused by the impaired cytophysiological activities of mitochondria and/or protein-forming organelles, and/or autonomic nervous system failures in the neurosensory stimulation of the secretory units, including acinar cells and myoepithelial cells, affecting the major salivary glands. The severity of salivary reducing was eliminated after application of all therapies; on the other side, the OAm (100% of patients) and MDHB (75% of patients) exhibited better effect in saliva production when compared with sNME. Presumably, mechanical effects of the OAm and MDHB stimulated the salivary glands by means of masticatory movements. We still infer that this activity could activate parasympathetic nervous system receptors and, consequently, favor the performance of morphofunctional units of the salivary glands, known as adenomers. These structures are responsible for synthesis and secretion of saliva. In all therapies, there was a slight reduction in salivary pH, however the rate of values remained normal. Among them, sNME revealed statistical difference in salivary pH; thus, we conjectured that sNME led to a better balance of the salivary buffering capacity. We consider that this balance kept the oral homeostasis, hampering the development of oral diseases as caries, periodontitis, and halitosis [14]. Reported that high salivary pH indicates patients susceptible to salivary calculus formation and may influence on the exacerbation of periodontal diseases. As discussed earlier, we proven that the BC was improve in the therapy with sNME (71% of patients), follow by MDHB (50% of patients) and OAm (43% of patients). Probably, this fact occurred due to electric current emitted by the electrostimulating device, resulting in an increased recruitment of motor units of the masticatory muscles and better cellular excitability of terminal secretory units (acinar and myoepithelial cells) of the minor and major salivary glands. Thus, we can infer that the patients treated with sNME showed better resistance to caries, despite the reduced salivary flow. Some authors reported that the prevalence of caries is low in DS. This condition could be related to the high salivary concentration of specific anti-Streptococcus mutans IgA [2,15-17]. Others described different levels of cariogenic microorganisms in the saliva, mainly in children with DS. It is suggested that children with DS could have a low profile of cariogenic Streptococcus mutans or differences in acidogenicity and aciduricity of strains which could be associated with the low prevalence of caries in this population [2]. The analysis of the SC levels is accurate, safe, and similar to serum levels, being well-used as a good physiological biomarker to determine the real emotional conditions, identifying the susceptibility to physical and/or psychological stress [13]. The cortisol is a steroid hormone, produced in the cortical layer of the adrenal gland, being directly involved in stress disorders. Concerning its body distribution, 90% of plasma cortisol is bound to cortisol-binding globulin (CBG), 5% bound to generic binding proteins as albumin and α-1 glycoprotein, and 5% unbound or free [18,19]. According to [20], the biological activity of a hormone is determined by the concentration of free hormone. Then, the measurement of cortisol levels is strongly recommended in saliva than in blood since free cortisol is more available in the salivary fluid. Authors describe that this biomarker is also used to study the functioning of the hypothalamic-pituitary-adrenal axis [21,22]. In our study, before and after the therapy with sNME, one patient had exacerbated morning SC levels. We conjecture a possible hormonal dysfunction of the hypothalamus, pituitary, and/or adrenal glands; the follow, this patient was referred to an endocrinologist for further investigations. We identified a discrete increase of morning SC levels in 50% of patients treated with MDHB and OAm; in contrast, all patient treated with some exhibited reduction of night CS. Furthermore, when we separately compared the therapies, the number of patients treated with OAm showed statistically significant difference in the night CS levels; therefore, we infer that these individuals had high susceptibility to stress disorders. We cannot still claim if this therapy directly influenced on this variation; hence, we suggested more researches to validate the OAm action on the nSC levels. Considering some phenotypical features in DS, the effects of stress together with poor sleep quality could trigger an increase in cardiovascular tone, alter heart rate variability, and generate an imbalance of microorganisms in the oral cavity. This fact reinforces the importance of routine saliva test for this population, aiming to intervene early on the onset of stress symptoms and to identity the imbalance of microorganisms in the saliva. Still about the SC, [23] reported that the prolonged reduction of CS levels can lead to fatigue, weight loss, and muscle weakness. It is still noteworthy that patients with DS, severe dysphagia, and low immunity are risk of occurrence of aspiration [11]. Given that, we assess the presence of Pseudomonas aeruginosa (Pa) species on saliva of our patients. The samples showed that no patient had culture-positive to Pa species before the proposed therapies. Then, we presume that no Pa species would be detected after the therapies, since our patients maintained a satisfactory general and oral health during all study period. Researches have described structural and physiological alterations in the salivary glands’ parenchyma in Down syndrome [8,12]. According to [7], congenital absence and atrophy of major salivary glands were identified in DS, especially in the submandibular glands. These findings strengthened the recommendation of ultrasound exam, with and without Doppler, in our studies, aiming to diagnose morphological abnormalities of the parotid, sublingual, and submandibular salivary glands. Our results showed that no patient (12/23 patients with DS) had congenital abnormalities of major salivary glands, however, chronic sialadenitis in the parotid glands was suggested in one patient (1/12 patients with DS; P5MDHB). Some adjacent alterations were suggestively found as cervical lymphadenopathy (2/12 patients with DS; P2OAm, P3OAm) and inflammatory process in thyroid gland (1/12 patients with DS; P3sNME). Theses imaging alterations were investigated by a specialized medical staff and, the follow, the patients were duly treated. Other patients (11/23) did not undergo the USG due to the follows intercurrences: Unstable general health status and lack of collective public transport on the day of the exam scheduling. The variation in the general health condition surely occurred due to high susceptibility to recurrent infections in DS, caused by the molecular mechanisms disorders of their immune system. In additional information, our patients had OSA, most likely resulting from airway abnormalities associated with orofacial hypotonia, agreeing with the studies of [24,12]. We infer that these factors could damage the saliva production and release. Considering the increase in life expectancy in DS and the effects of orofacial therapies on the physical, chemical, and microbiological properties of saliva, we indicate saliva test as an alternative diagnostic technique to investigate the oral and general manifestations of patients, especially people with neuropsychomotor disability and/or with loss of autonomy and functional capacity in their daily living.
Conclusion
We can conclude that the saliva production had reduced values in all patients with DS and OSA, before and after the therapies; however, the therapies with OAm followed by the DMHB mitigated its severity. The sNME improved the saliva quality, ph value and BC, when compared with others. Susceptibility to stress disorders was identified in patients treated with OAm in the night period; and no risk for aspiration pneumonia was detected before the therapies. Congenital anomalies of major salivary glands were not found; however, some acquired alterations were evidenced in this population.
Reference values (Source: Gomes et al., 2020; Gomes et al., 2023)
SFR (salivary flow rate; mL/min): normal flow (N;>1.0), limit value (L; until 1.0), reduced flow (≤0.7), and hyposalivation/xerostomia condition (≤0.1); pH value: normal (N; from 5.3 to 7.8); BC (buffer capacity) normal (pHfinal = 5.1 to 7.0), limit value (pHfinal = 4.0 to 5.0), and low (pHfinal < 4.0); mSC (morning salivary cortisol concentration): female and male adolescents, ages 12 to 18 years (range: 0.021 to 0.883), adult men, ages 21 to 30 years (range: 0.112 to 0.743), and adult women, ages 21 to 30 years (women; range: 0.272 to 1.348); and nSC (night salivary cortisol concentration): female and male adolescents, ages 12 to 18 years (range: ≤0.028 to 0.259), adult men, ages 21 to 30 years (man; range: ≤0.028 to 0.308); and adult women, ages 21 to 30 years (women; range: ≤0.028 to 0.359). Based on the SC values found in our studies, patients with 19 years-old were inserted into age groups between 12 to 18 years-old; and the patients with 20 years-old were inserted into age groups of 21 to 30 years-old. PA: identification for Pseudomonas aeruginosa
Symbols for results: (□black) reduced flow rate or low salivary cortisol concentration; (λ) hyposalivation/xerostomia condition; (□black) high pH value and increased salivary cortisol concentration; (~) no alteration of values; (IS) insufficient amount of saliva; (‘) salivary cortisol test no done; (Π) identification for PA was not performed after the therapies because the colonies of PA was not found in all patients before the therapies, become unnecessary to repeat this testing; (/) therapy not completed due to the Covid-19 pandemic; and (□ or □ blue) comparison between the salivary parameters, before and after the therapies.
Note: (∟) Adrenal gland functions were investigated due to the accentuated SC levels.
Declarations
Acknowledgements: The authors would like to thank all patients and caregivers who participated in this study.
Funding:enter for Bioscience Applied to Patients with Special Health Care Needs (known as CEBAPE), Institute of Science and Technology, São Paulo State University, UNESP, Brazil, received funding from State of São Paulo Research Foundation (FAPESP) – grant number 2017/06835–8, contact telephone number + 55 11 3838 4000.
Institutional review board statement: The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committees on Human Research of the Institute of Science and Technology of the São Paulo State University, IST-UNESP (CEPh/CAAE process number 64 173 616.4.0000.0077).
Conflicts of interest: The authors declare no conflicts of interests.
Author contribution: All the authors contributed to the conception, design and performance of the study. MFG, LCG, RSN, MACS and JBOA provided the idea for the study, established the hypothesis and wrote the original proposal. LCG provided training for the sNMES and HB for all team. LCG performed the assembly of the all PSG II exam. LVFO and LCG performed PSG interpretation. MTSD performed the saliva collection. MTSD and CYKI were responsible for interpretation of salivary data. RSN performed Ultrasonography exam and its interpretation. BDP collected all demographic and anthropometric. LVFO performed the data tabulation. MFG contributed to statistical analysis. JBOA, MACS, MFG and LCG were involved in critically revising the manuscript. LCG, MASC, JBOA, SMR and MFG supervised this study, participated in its design and coordination and, revised the manuscript that lead to the final approval of the current submission. All authors read and approved the final manuscript.
References
- Davidovich E, Aframian DJ, Shapira J, Peretz B. A comparison of the sialochemistry, oral pH, and oral health status of Down syndrome children to healthy children. Int J Paediatr Dent. 2010; 20: 235-41.
- Domingues NB, Mariusso MR, Tanaka MH, Scarel-Caminaga RM, Mayer MPA, et al. Reduced salivary flow rate and high levels of oxidative stress in whole saliva of children with Down syndrome. Spec Care Dentist. 2017; 37: 269-76.
- Bermudez BE, Medeiros SL, Bermudez MB, Novadzki IM, Magdalena NI. Down syndrome: Prevalence and distribution of congenital heart disease in Brazil. Sao Paulo Med J. 2015; 133: 521-4.
- Duarte RL, Magalhães-da-Silveira FJ. Factors predictive of obstructive sleep apnea in patients undergoing pre-operative evaluation for bariatric surgery and referred to a sleep laboratory for polysomnography. J Bras Pneumol. 2015; 41: 440-8.
- Komatsu T, Duckyoung Y, Ito A, Kurosawa K, Maehata Y, et al. Increased oxidative stress biomarkers in the saliva of Down syndrome patients. Arch Oral Biol. 2013; 58:1246-50.
- Schwertner C, Moreira MJ, Faccini LS, Hashizume LN. Biochemical composition of the saliva and dental biofilm of children with Down syndrome. Int J Paediatr Dent. 2016; 26: 134-40.
- Odeh M, Hershkovits M, Bornstein J, Loberant N, Blumenthal M,et al. Congenital absence of salivary glands in Down syndrome. Arch Dis Child. 2013; 98: 781-3.
- Odeh M, Bronshtein M, Bornstein J. Congenital absence of salivary glands in fetuses with trisomy 21. Isr Med Assoc J. 2017; 19: 12-4.
- Odeh M, Bronshtein M, Bornstein J. Congenital absence of salivary glands in fetuses with trisomy 21. Isr Med Assoc J. 2017; 19: 12-4.
- Nanci A. Ten Cate Histologia Oral (7a. edição) Rio de Janeiro, RJ Elsevier. 2008.
- Giannasi LC, Dutra MTS, Tenguan VLS, Mancilha GP, Silva GRC, et al. Evaluation of the masticatory muscle function, physiological sleep variables, and salivary parameters after electromechanical therapeutic approaches in adult patients with Down syndrome: A randomized controlled clinical trial. Trials. 2019; 20: 215.
- Gomes MF, Giannasi LC, Fillietaz-Bacigalupo E, de Mancilha GP, de Carvalho Silva GR, et al. Evaluation of the masticatory biomechanical function in Down syndrome and its Influence on sleep disorders, body adiposity and salivary parameters. J Oral Rehabil. 2020; 47: 1007-22.
- Gomes MF, Abreu MFF, Giannasi LC, Silva DBR, Koga-Ito CY, et al. An exploratory study of the overall systemic and oral health status in older patients with Alzheimer’s Disease. J Alzheimers Dis Parkinsonism. 2023; 13: 564.
- Baliga S, Muglikar S, Kale R. Salivary pH: A diagnostic biomarker. J Indian Soc Periodontol. 2013; 17: 461-5.
- Lee SR, Kwon HK, Song KB, Choi YH. Dental caries and salivary immunoglobulin A in Down syndrome children. J Paediatr Child Health. 2004; 40: 530-3.
- Gufran K, Alqutaym OS, Alqahtani AAM, Alqarni AM, Hattan EAE, et al. Prevalence of dental caries and periodontal status among Down’s syndrome population in Riyadh city. J Pharm Bioallied Sci. 2019; 11: S252-S5.
- Willis JR, Iraola-Guzmán S, Saus E, Ksiezopolska E, et al. Oral microbiome in Down syndrome and its implications on oral health. J Oral Microbiol. 2020; 13: 1865690.
- Granger DA, Hibel LC, Fortunato CK, Kapelewski CH. Medication effects on salivary cortisol: tactics and strategy to minimize impact in behavioral and developmental science. Psychoneuroendocrinology. 2009; 34: 1437-48.
- Elder GJ, Wetherell MA, Barclay NL, Ellis JG. The cortisol awakening response-applications and implications for sleep medicine. Sleep Med Rev. 2014; 18: 215-24.
- Blair J, Adaway J, Keevil B, Ross R. Salivary cortisol and cortisone in the clinical setting. Curr Opin Endocrinol Diabetes Obes. 2017; 24: 161-8.
- Bella GP, Garcia MC, Spadari-Bratfisch RC. Salivary cortisol, stress, and health in primary caregivers (mothers) of children with cerebral palsy. Psychoneuroendocrinology. 2011; 36: 834-42.
- Šupe-Domić D, Milas G, Stanišić L, Drmić Hofman I, Martinović Klarić I. Reference intervals for six salivary cortisol measures based on the croatian late adolescence stress study (CLASS). Biochem Med (Zagreb). 2018; 28: 010902.
- Sesay AM, Micheli L, Tervo P, Palleschi G, Virtanen V. Development of a competitive immunoassay for the determination of cortisol in human saliva. Anal Biochem. 2013; 434: 308-14.
- Ram G, Chinen J. Infections and immunodeficiency in Down syndrome. Clin Exp Immunol. 2011; 164: 9-16.