
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Thrombo-hemorrhagic complications in 37 years-old ethanolic: Superior mesenteric vein thrombosis and upper GI bleeding as a first presenting feature of polycythemia rubra vera
Khin Phyu Pyar1*; Tin Mar Yee2; Than Naing Tun2; Aung Htet3; Win Myint4; Aung Aung5; Kyaw Zay Ya5; Soe Bo Bo Thet5; Nyan Naing Soe6; Min Ko6; Ye Min Thu6; Sein Kyaw7; Kaung Myat Oo8; Lwin Myo9; Htain Tauk6
1Department of Medicine/ Department of Nephrology, Professor and Head/Senior Consultant Physician, Defence Services Medical Academy/ No. (1) Defence Services General Hospital (1000-Bedded), Myanmar.
2Senior Consultant Surgeon, No. (1) Defence Services General Hospital (1000-Bedded), Myanmar.
3Senior Consultant Radiologist, No. (1) Defence Services General Hospital (1000-Bedded), Myanmar.
4Senior Consultant Physician, No. (1) Defence Services General Hospital (1000-Bedded), Myanmar.
5Consultant Hematologist, No. (1) Defence Services General Hospital (1000-Bedded), Myanmar.
6Consultant Physician, No. (1) Defence Services General Hospital (1000-Bedded), Myanmar.
7Consultant Radiologist, No. (1) Defence Services General Hospital (1000-Bedded), Myanmar.
8Consultant Pathologist, No. (1) Defence Services General Hospital (1000-Bedded), Myanmar.
9Internal Medicine Fellow, Defence Services Medical Academy, Myanmar.
*Corresponding Author : Khin Phyu Pyar
Department of Medicine/ Department of Nephrology,
Professor and Head/Senior Consultant Physician,
Defence Services Medical Academy/ No. (1)
Defence Services General Hospital (1000-Bedded),
Myanmar.
Email: khinphyupyar@gmail.com
Received : Mar 12, 2024
Accepted : May 02, 2024
Published : May 09, 2024
Archived : www.jcimcr.org
Copyright : © Pyar KP (2024).
Abstract
A 37 years-old man, chronic alcoholic and chronic smoker, presented with abdominal pain and fever. Full blood count was suggestive of polycythemia rubra vera with high packed cell volume of 57%. Contrast Enhanced Computed Tomography (CECT) abdomen showed portal/superior mesenteric vein thrombosis. Venesection, fluid replacement, heparin therapy and antibiotics were initiated; heparin therapy was withheld for 72 hours as he was having hematemesis and melaena. This case described the difficult clinical dilemma as he had both thrombo- hemorrhagic complications simultaneously. He died of ARDS and septic shock. Autopsy findings were reported. We reviewed the current literature.
Keywords: Polycythemia rubra vera; Portal/Superior mesenteric vein thrombosis; Alcoholic; Smoker; Hematemesis; Melaena.
Citation: Pyar KP, Yee TM, Tun TN, Htet A, Myint W, et al. Thrombo-hemorrhagic complications in 37 years-old ethanolic: Superior mesenteric vein thrombosis and upper GI bleeding as a first presenting feature of polycythemia rubra vera. J Clin Images Med Case Rep. 2024; 5(5): 3040.
Introduction
Acute Vascular Insufficiency of intestines (AVI) is a rare cause of severe abdominal pain contributing to 0.09% to 2% of admissions in surgical emergency; however, it needs early recognition because of its high mortality of 40% to 80% requiring timely diagnosis and prompt intervention. Mesenteric vein thrombosis is a rare but potentially lethal cause of abdominal pain. Acute thrombosis often presents with abdominal pain, whereas chronic disease manifests either as an incidental finding on Contrast- Enhanced Computed Tomography (CECT) or with features of portal hypertension. The presence of collateral circulation and cavernoma around a chronically thrombosed vein differentiates chronic from acute disease. CECT diagnoses about 90% of cases. The prevalence of mesenteric venous thrombosis has increased over the past 2 decades with the routine use of CECT in patients presenting with abdominal pain and those with portal hypertension. The superior mesenteric vein is often involved, whereas involvement of the inferior mesenteric vein is rare. Associated portal venous thrombosis can be seen if the disease originates in the major veins instead of the small vena rectae.
Mesenteric vein thrombosis is a rare disorder that is often the first manifestation of a systemic condition such as a hypercoagulable state or cancer. Myeloproliferative disorders can present as mesenteric vein thrombosis even in the setting of relatively normal peripheral blood counts. A recent novel mutation in the Janus activated kinase 2 gene involving a gain-offunction substitute of valine to phenylalanine at position 617 (JAK2 V617F) has been discovered to be prevalent in patients with mesenteric vein thrombosis and myeloproliferative disorder. Rare causes like secondary polycythemia due to androgen gel [12] and local abdominal inflammatory conditions such as inflammatory bowel disease causing mesenteric vein thrombosis were reported [20]. A rare case of polycythemia vera with hyperhomocysteinemia presenting with severe abdominal pain due to portal vein thrombosis was reported [6].
Management of mesenteric vein thrombosis is aimed at preventing bowel infarction and recurrent thrombosis. Anticoagulation is the mainstay of management. Increasing awareness of mesenteric vein thrombosis and frequent use of anticoagulation has reduced the need for surgical intervention; and, outcome is improved at present. However, management on cases having both thrombo-hemorrhagic complications simultaneously is difficult. This case describes the difficult dilemma that occurs when clinical presentation includes both thrombo-hemorrhagic complications simultaneously.
Case presentation
Previously healthy middle age man presented with abdominal pain for 10 days; it was accompanied by 3 days history of fever. He also noticed jaundice for one year. He has history of alcohol drinking for 6 years duration; maximum half bottle per day. He was also a chronic smoker for 13 years duration; 3,4 cheroot/ day (2.6 pack year). There was no history of hematemesis and melaena. In review of past history, he had gastritis; and no other medical problems and no surgical intervention.
Initial examination revealed as follows: mild jaundice; blood pressure was 110/60 mmHg; pulse rate was 64/min; SpO2 was 97% on air; abdomen was soft; mild hepatosplenomegaly; tenderness in periumbilical area and left iliac fossa. Long history of jaundice for one year with hepatomegaly was suggestive of chronic alcoholic hepatitis. Splenomegaly may be due to portal hypertension; it may also be feature of myeloproliferative disorder.
ECG showed heart rate 60/min, sinus rhythm, no ST and T changes. Random blood sugar was 136 mg/dl. He had high hemoglobin 18.5 gm%; high PCV 57%; high RBC 9.65X106 /uL; MCV 59.1fL; neutrophil leukocytosis (total WBC 20.26X10 /L; neutrophil 82.7%); very high platelets 1058X109 /L; normal serum creatinine 0.94 mg/dL; normal blood urea 96 mg/dL; normal ALT 13.9U/L; normal alkaline phosphatase 119 U/L.
Patient continued to have agonizing pain; not relieved with parenteral morphine and analgesics. Four hours later, areas of tenderness extended to epigastrium, right iliac fossa and left iliac fossa with rebound tenderness indicating peritonitis. Plain X ray abdomen did not reveal gas under diaphragm. USG abdomen was suggestive of acute appendicitis and mild splenomegaly. Possibility of either mesenteric artery occlusion or mesenteric vein thrombosis caused by polycythemia rubra vera was considered in view of high RBC mass, high hemoglobin and high PCV.
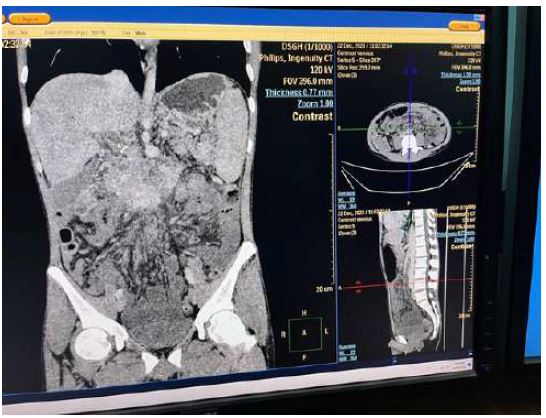
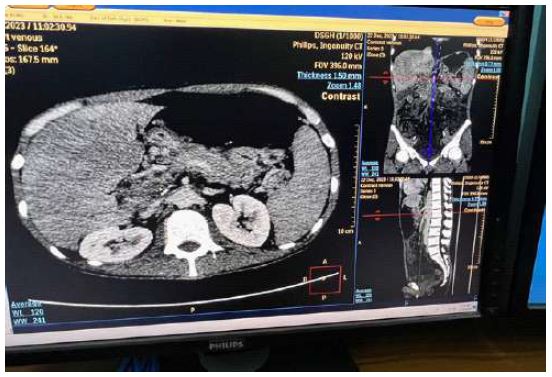
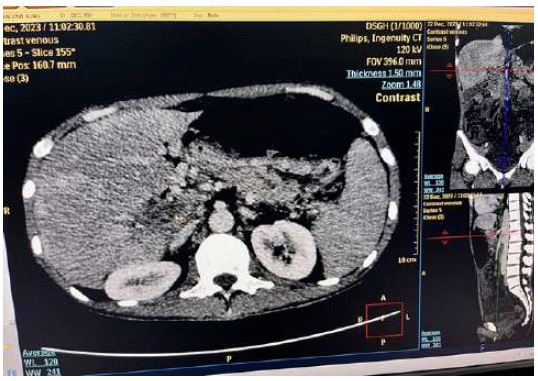
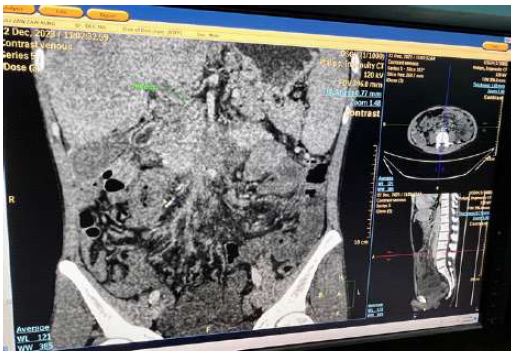
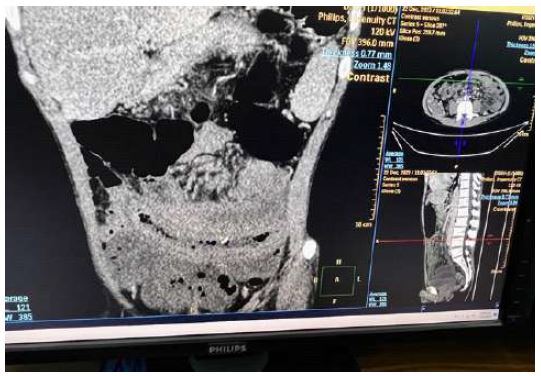
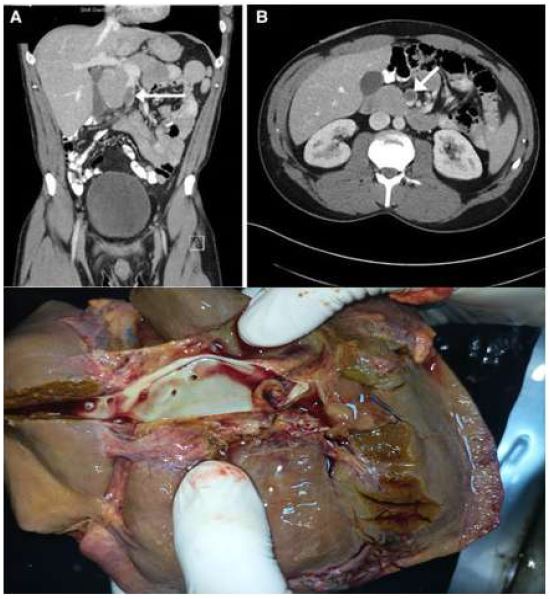
The pain was persistent. Twenty-four hours after admission, the whole abdomen was tender and rebound tenderness was remarkable too. CECT abdomen showed features of mesenteric vein thrombosis with extension to portal vein. Portal cavernosum and mesenteric fat infiltration were not seen. Small bowel walls were oedematous revealing subacute obstruction. They are shown in photo [2-4].
Venesection 500 ml blood 2 times in 2 days followed by rehydration with normal saline was done. Bowel rest, parenteral fluids, antibiotics and anticoagulation with heparin were given.
Other causes of thrombosis in young age were looked for like paroxysmal nocturnal hemoglobinuria (PNH); sugar water test and heat resistance test were negative. ANA (anti-nuclear antibody test) was positive (1/100). Lupus anticoagulant was moderately positive (1.8). Both Anti-cardiolipin (Ig G) and beta2 Glycoprotein (Ig G) were negative.
48 hours later, he vomited coffee ground fluid for 5 times; and he passed melaena stool for one time which was 300 cc approximately. He had high color urine too. He became very weak and ill; temperature was 99* F; blood pressure dropped to 100/70 mmHg; and, pulse rate was 130/min. However, lungs were clear. There was tenderness in lower abdomen with rebound tenderness pointing to intestinal perforation; the abdomen became distended. The abdomen girth increased gradually. The amount of blood loss in hematemesis and melaena was increasing too.
The cause of upper GI bleeding might be bleeding manifestation of polycythemia vera itself or related with heparin. The bleeding might be from underlying alcoholic gastric erosion. Parenteral heparin was stopped temporarily for 72 hours till GI bleeding ceased. We continued bowel rest, parenteral fluids, antibiotics; and, we planned bone marrow biopsy and Janus kinase 2 mutation (JAK2) mutation.
Table 1: Hematological and biochemical parameters.
| Day ‘0’ | Day ‘5’ | Day ‘6’ | Day ‘7’ | Day‘11’ | Day‘12’ | |
|---|---|---|---|---|---|---|
| Hemoglobin (gm%) | 18.5 | 14.8 | 13.5 | 12.3 | 12.6 | 13.6 |
| RBC mass (million/cumm) (x106 /mL) | 9.65 | 6.8 | 6.98 | 6.42 | 5.48 | 5.96 |
| Packed cell volume (%) | 57 | 43 | 41.5 | 38.5 | 35.4 | 38.4 |
| MCV(mm3 )(fL) | 59.1 | 63 | 59.5 | 60 | 65 | 64 |
| Total WBC (x109 /L) | 20.26 | 28.9 | 30.13 | 33 | 27.0 | 42.3 |
| Neutrophils(%) | 82.7 | 81.8 | 84.2 | |||
| Lymphocyte (%) | 7.2 | 5.0 | 5.9 | |||
| Eosinophils (%) | ||||||
| Monocyte (%) | 9.3 | 3.46 | 2.5 | 2.3 | ||
| Platelets (x109 /L) | 1058 | 950 | 959 | 772 | 868 | 731 |
| Urea (mg%) | 96 | 93.8 | 93.8 | 32 | 55.3 | |
| Creatinine (mg/dL) | 0.94 | 1.02 | 1.0 | 0.56 | 0.75 | |
| Na | 140 | 140 | 140 | 137 | ||
| K | 5.0 | 5.0 | 4.5 | 5.3 | ||
| Cl | 104 | 104 | 99 | 97 | ||
| Total Bilirubin (mg/dl) | 7.19 | 14.8 | 18.3 | |||
| Direct Bilirubin (mg/dl) | 12.9 | |||||
| Indirect Bilirubin(mg/dl) | 1.9 | |||||
| ALT (U/L) | 13.9 | 22 | 35 | 52 | ||
| AST(U/L) | 55 | 78 | 119 | |||
| ALP(U/L) | 119 | 75 | 117 | |||
| Total protein (g/dL) | 6.5 | 5.5 | ||||
| Albumin (g/dL) | 3.2 | 2.2 | ||||
| Globulin (g/dL) | 3.3 | 3.3 | ||||
| LDH (U/L) | 369 | 488 | ||||
| PT (sec) | 20.1 | 18.2 | 13.8 | |||
| INR | 1.86 | 1.63 | 1.07 | |||
| APTT (sec) | 41.2 | 40.5 | ||||
| Fibrinogen (mg/dl) | 390 | |||||
| D-dimer (ng/dl) | 1488 |
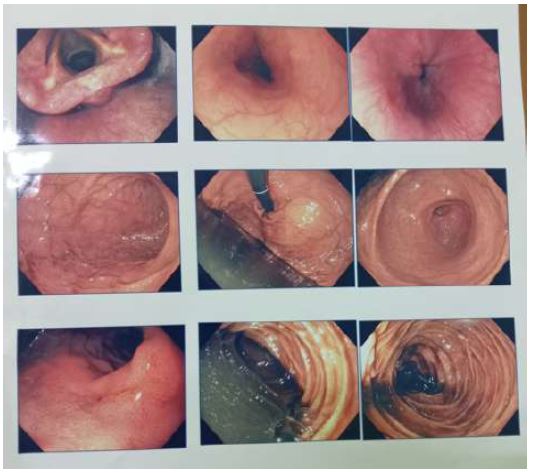
Esophagogastroduodenoscopy revealed small duodenal ulcer, congestion of gastric mucosa and coffee ground residues as shown in photo [1].
On Day 15, he had dyspnea at rest; SpO2 was 90% with oxygen; general condition was very ill; temperature was 99* F; blood pressure fell to 90/60 mmHg; tachycardia of 100/min; air entry reduced in both lower zones. Abdomen became more distended with ascites. All features were suggestive of ARDS and septic shock. SpO2 kept falling to 87% with double oxygen supply; blood pressure dropped further even with inotropes. Patient expired on Day 16.
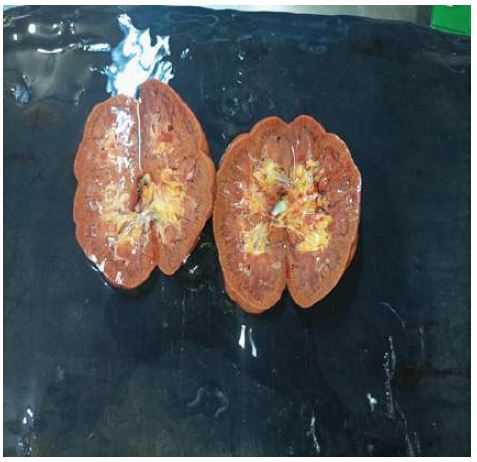
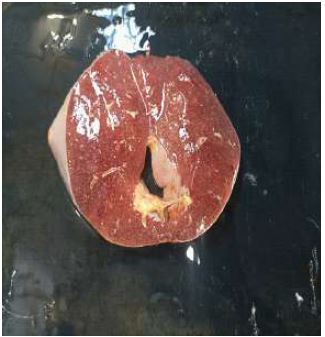
Autopsy revealed cut section of inferior vena cava; thrombosis in superior mesenteric vein extending to part of portal vein. It is shown in photo [5]. Kidneys were normal. It can be seen in photo [6]. Lungs were heavily stained with nicotine; cut section revealed brownish fluid indicating oedema. Photo [7] demonstrates them. Liver did not show features of cirrhosis; chronic hepatitis only. Photo [8] demonstrates smooth surface of liver and its cut section. Spleen was normal; cut section was septic. It is shown in photo [9]. Pancreas was normal as shown in photo [10]. Mucosal surface of stomach was erythematous; congested vessels were noted. It is demonstrated in photo [11]. Both small intestine and large intestine till transverse colon were discolored; oedematous; brownish black. It is revealed in photo [12].










Discussion
Acute Vascular Insufficiency of intestines (AVI) is a rare cause of severe abdominal pain contributing to 0.09% to 2% of admissions in surgical emergency; however, it needs early recognition because of its high mortality of 40% to 80% requiring timely diagnosis and prompt intervention. According to Reinus et al., the frequency distribution of occlusion of mesenteric vessels by arterial embolism was recorded in half of them; one- quarter of occlusion was due to thrombosis. And, venous thrombosis was seen in only 5% of them [19]. Therefore, this case was one of the rare cases of acute vascular insufficiency of intestines due to superior mesenteric vein.
Acute vascular insufficiency of intestines may be arteriopathy or venopathy. Acute superior mesenteric arteriopathy is caused by a mesenteric embolus, thrombus, or vasospasm (i.e., nonocclusive vasculopathy) whereas acute superior mesenteric venopathy is caused by a thrombus, which is often associated with a hypercoagulopathy. This case was a good example as its underlying cause was hypercoagulopathy (polycythemia).
The clinical presentation of both arteriopathy or venopathy is often subtle and nonspecific at an early stage. It becomes overt and specific only when advanced and severe; and, when ischemia progresses to necrosis. This patient had abdominal pain for 10 days prior to admission; it became progressive over succeeding 2 weeks during hospital stay. In fact, this patient followed the natural course of acute superior mesenteric venopathy.
According to Cappell, the mortality pattern of superior mesenteric venopathy is less rapidly progressive and lower than that of acute superior mesenteric arteriopathy; nonetheless, it still has significant mortality [7].
Blood supply and venous drainage of intestine have some peculiar points in preventing bowel ischemia. Acute vascular insufficiency of intestines may be nonocclusive in 20% to 30% of the patients [7]. Normally intestinal ischemia is prevented by its high perfusion through celiac mesenteric artery, superior mesenteric artery/inferior mesenteric artery, and a parallel system of venous drainage [17]. Therefore, bowel ischemia can occur only when blood supply is markedly reduced to 75% or more leading to a continuum of intestinal necrosis, perforation, infarction, or gangrene [1]. Therefore, early diagnosis and timely anticoagulation have high chances of intestinal survival.
Early diagnosis and aggressive therapy on intestinal vasculopathy significantly reduces the mortality rate of them [7]. Endovascular therapy may be an option in the few patients with mesenteric venous thrombosis who do not respond to anticoagulation therapy. The concept of damage-control surgery is recommended after intestinal revascularization [1]. Early diagnosis and prompt anticoagulation are the mainstay of therapy unless there are signs of peritonitis that necessitate surgical resection of the infarcted bowel [8]. In this patient, anticoagulation was initiated early. However, it was withheld temporarily for several days as he had bleeding. It led to ongoing ischemia and peritonitis. Because of simultaneous thrombosis and hemorrhage, laparotomy and resection of gangrenous bowel had several disadvantages like uncontrolled bleeding during surgery. And, the surgical team decided ‘not to do laparotomy’.
Systematic review done from 2015 to 2020 on acute mesenteric ischemia mentioned that anticoagulation therapy is necessary to be able to have a succesful non-operative succesful course [2]. The increasing use of anticoagulant medication as initial treatment and the widespread use of abdominal CT have improved the outcome in patients with mesenteric vein thrombosis. A high index of suspicion, recognition of known risk factors, or a previous history of venous thrombosis coupled with a history of nonspecific abdominal symptoms should alert clinicians to the possibility of mesenteric vein thrombosis [8]. This patient had correct diagnosis early.
Various treatments on myeloproliferative disorder such as plasma exchange and cytoreduction, venesection, hydroxyurea, interferon, busulfan, pipobroman, radioactive phosphorus, aspirin, anagrelide, ruxolitinib were reviewed in hopes of preventing further bleeding or thrombotic complications [11,13] . However, management of cases having both thrombosis and hemorrhage simultaneously was rarely reported. Amaria et al described a patient with isolated splenic vein thrombosis due to polycythemia vera presenting as upper gastrointestinal hemorrhage; he was cured by splenectomy [4]. This patient received anticoagulation therapy early after computed tomography with intravenous contrast-enhancement. Moreover, venesection was done early and packed cell volume dropped to normal with fluid replacement. He developed upper gastro-intestinal bleeding; therefore, heparin therapy was withheld till bleeding ceased. This case described the difficult clinical dilemma as he had both thrombo-hemorrhagic complications simultaneously. Withholding heparin for 3 days lead to progression of mesenteric vein thrombosis and bowel ischemia; a continuum of intestinal necrosis, perforation, infarction and gangrene. This is another reason to share difficult clinical dilemma in resource poor setting.
Polycythemia vera is a chronic myeloproliferative disorder characterized by clonal proliferation of bone marrow progenitors. Polycythemia vera usually cause acute thrombosis of either mesenteric artery or mesenteric vein; however, a case of ileal stricture resulting from ischemic enteritis caused by polycythemia vera was reported in the literature [22]. The prevalence of polycythemia vera is 0.3 per 100,000 people; and, a peak prevalence is the sixth and seventh decades of life [16]. This patient was 37 years old; relatively young. This is one reasons for case writing.
If we had given advanced management like percutaneous treatment of a superior mesenteric vein thrombosis using both mechanical thrombectomy and pharmacologic fibrinolytic strategies [5,10], the patient would have survived. The JAK2 sequence variation is a new noninvasive marker for diagnosing underlying thrombophilia and myelodysplastic syndrome among patients with mesenteric vein thrombosis. The activation of Janus kinase/transducer signaling pathway is proposed as an underlying mechanism for mesenteric ischemia [15]. It was beyond our reach being resource limited country. The presence of the JAK2 mutation is an important prothrombotic risk factor; it can contribute to large venous thrombosis [3]. This patient might have JAK2 mutation.
Several treatment options for myeloproliferative disorder on 6062 articles by McMullin et al; and, they were cytoreduction, venesection, hydroxyurea, interferon, busulfan, pipobroman, radioactive phosphorus, aspirin, anagrelide, ruxolitinib, pruritus surgery and management [13]. Owen et al reported cases with mesenteric vein thrombosis in patients with polycythemia rubra vera even though they had relatively normal peripheral cell count [18]. De Stefano studied 181 cases with myeloproliferative neoplasms presented with splenic vein thrombosis. They reported that despite anticoagulation treatment, the recurrence rate after splenic vein thrombosis in patients with myeloproliferative neoplasms is high; and, they suggests the exploration of new avenues of secondary prophylaxis with new antithrombotic drugs and JAK-2 inhibitors [9]. This patient had ongoing bowel ischemia though hemoglobin and packed cell volume became normal. It indicated the thrombotic tendency of myeloproliferative disorder. It is another reason for case reporting.
Vietti Violi et al analyzed the determinant factors for mesenteric venous thrombosis evolution. In 20 cases with acute mesenteric vein thrombosis. radiologic evolution of isolated acute mesenteric venous thrombosis and associated prognostic factors were studied. And, they found that anticoagulation did not influence recovery [21]. Those with less frequent central lesion, longer thrombosed segment, larger transverse diameter of thrombus and mesenteric fat infiltration at diagnosis were prone to chronic mesenteric venous thrombosis. In this patient, thrombosis in superior mesenteric vein extended to portal vein indicating involvement of larger longer segment. He would have developed chronic mesenteric venous thrombosis if he had not died.
Zhang raised the issue ‘early antithrombotic therapy can reduce complications patients with polycythemia with portal hypertension’ because they are at risk of thrombosis and bleeding [23]. This patient did not have signs of chronic liver disease though he noticed jaundice for one year. He was a chronic alcoholic; autopsy finding was compatible with chronic hepatitis without evidence of cirrhosis. Esophagogastroduodenoscopy done at the time of upper gastrointestinal bleeding showed gastritis; however, autopsy of stomach showed very congested gastric vessels.
Conclusion
Mesenteric venous thrombosis is not common but it is important clinical entity. Diagnosis of this condition is sometimes difficult; and treatment is often delayed because patients usually present with nonspecific abdominal symptoms. The hallmark is pain that is out of proportion to the physical findings. A high index of suspicion is required for the diagnosis of mesenteric venous thrombosis. The widespread use of abdominal computed tomography has improved diagnoses of mesenteric venous thrombosis. The increasing use of anticoagulant medication as initial treatment can improve the outcome. Early diagnosis and prompt anticoagulation are the mainstay of therapy unless there are signs of peritonitis that necessitate surgical resection of the infarcted bowel. Thrombo-hemorrhagic complications in polycythemia rubra vera are difficult clinical dilemma.
Declarations
Acknowledgements: The authors would like to thank the patient and family for giving consent to this article. Also, to all doctors and nursing team for making great efforts in caring him. The authors acknowledged the following team; Professor Tin Mar Yee and surgical team, Professor Ohmar Hlaing and radiology team, Professor Thet Naing, Professor Myint Zaw, Professor Kyaw Zay Ya and Professor Ko Ko Lwin for administrative support.
Conflict of interest: The authors declared no potential conflicts of interests with respect to authorship and publication of this article.
Ethical approval: Our institution does not require ethical approval for reporting cases.
Funding: The authors received no financial support for publication of this article.
Informed consent: The informed consent for publication in this article was obtained from patient.
References
- Acosta S. Mesenteric ischemia. Current Opinion in Critical Care. 2015; 21(2): 171-178. https://doi.org/10.1097/ MCC.0000000000000189.
- Acosta S, & Salim S. Management of Acute Mesenteric Venous Thrombosis: A Systematic Review of Contemporary Studies. Scandinavian Journal of Surgery. 2021; 110(2): 123-129. https:// doi.org/10.1177/1457496920969084.
- Agrawal S, Rayamajhi S, Rayamajhi A, Karki S, Deo A, Kharel KK, Lamsal M, & Hama R. Spontaneous bacterial peritonitis complicating extensive splanchnic vein thrombosis, a rare manifestation of essential thrombocythemia: A case report. Clinical Case Reports. 2023; 11(7): e7634.
- Amaria YN, Mittal V, & Hans SS. Splenic Vein Thrombosis Secondary to Polycythemia Vera-A Case Report. Vascular Surgery. 1988; 22(4): 275-279. https://doi.org/10.1177/153857448802200410.
- Araki N, Takimoto R, Chiba H, Araki H, Sato T, Iyama S, Hirakawa M, Ono K, Kawano Y, Takada K, Miyanishi K, Kobune M, Matsunaga T, Kato J, Nakamura T, & Niitsu Y. [Superior mesenteric and portal vein thrombosis in a polycythemia vera patient with JAK2 mutation]. [Rinsho ketsueki] The Japanese journal of clinical hematology. 2007; 48(7): 554-558.
- Behshad Pazooki, Hanieh Radkhah, & Alborz Sherafat. Portal Vein Thrombosis and Budd-Chiari Syndrome as the Inital Symptom of Polycythemia Vera and Hyperhomocysteinemia. Case Reports in Clinical Practice. 2019; 4(2). https://doi.org/10.18502/ crcp.v4i2.1704.
- Cappell MS. Intestinal (mesenteric) vasculopathy. I. Acute superior mesenteric arteriopathy and venopathy. Gastroenterology Clinics of North America. 1998; 27(4): 783-825, vi. https://doi. org/10.1016/s0889-8553(05)70033-9.
- Choudhary AM, Grayer D, Nelson A, & Roberts I. Mesenteric Venous Thrombosis: A Diagnosis not to Be Missed! Journal of Clinical Gastroenterology. 2000; 31(2). https://journals.lww.com/ jcge/fulltext/2000/09000/mesenteric_venous_thrombosis__a_ diagnosis_not_to.21.aspx.
- De Stefano V, Vannucchi AM, Ruggeri M, Cervantes F, Alvarez- Larrán A, Iurlo A, Randi ML, Pieri L, Rossi E, Guglielmelli P, Betti S, Elli E, Finazzi MC, Finazzi G, Zetterberg E, Vianelli N, Gaidano G, Nichele I, Cattaneo D, … Barbui T. Splanchnic vein thrombosis in myeloproliferative neoplasms: Risk factors for recurrences in a cohort of 181 patients. Blood Cancer Journal. 2016; 6(11): 493- 493. https://doi.org/10.1038/bcj.2016.103.
- Goldberg MF, & Kim HS. Treatment of Acute Superior Mesenteric Vein Thrombosis with Percutaneous Techniques. American Journal of Roentgenology. 2003; 181(5): 1305-1307. https://doi. org/10.2214/ajr.181.5.1811305.
- Rapidly Progressive Case of Hemorrhagic Pancreatitis in a Patient with Polycythemia Vera, or Not?: 821. Official Journal of the American College of Gastroenterology | ACG. 2012; 107. https://journals.lww.com/ajg/fulltext/2012/10001/a_rapidly_ progressive_case_of_hemorrhagic.821.aspx.
- Katz H, Popov E, Bray N, & Berman B. Mesenteric vein thrombosis caused by secondary polycythaemia from AndroGel. BMJ Case Reports. 2014. https://doi.org/10.1136/bcr-2014-206023.
- McMullin MFF, Mead AJ, Ali S, Cargo C, Chen F, Ewing J, Garg M, Godfrey A, Knapper S, McLornan DP, Nangalia J, Sekhar M, Wadelin F, Harrison CN. & the British Society for Haematology Guideline. A guideline for the management of specific situations in polycythaemia vera and secondary erythrocytosis. British Journal of Haematology. 2019; 184(2): 161-175. https://doi. org/10.1111/bjh.15647.
- McMullin MF, Mead AJ, Ali S, Cargo, C, Chen F, Ewing J, Garg M, Godfrey A, Knapper S, McLornan DP, Nangalia J, Sekhar M, Wadelin F, Harrison CN, & the British Society for Haematology Guideline. A guideline for the management of specific situations in polycythaemia vera and secondary erythrocytosis: A British Society for Haematology Guideline. British Journal of Haematology. 2019; 184(2): 161-175. https://doi.org/10.1111/bjh.15647.
- Moiz B, Muslim Z, Siddiqui ZF, & Zafar H. Acute Mesenteric Thrombosis: A Hematologist Perspective. Clinical and Applied Thrombosis/Hemostasis. 2020; 26. 1076029620932999. https:// doi.org/10.1177/1076029620932999.
- Ntounis T, Zioutos KA, Koutras A, Prokopakis I, Fasoulakis Z, Sapantzoglou I, Perros P, Samara AA, Spanoudakis E, Valsamaki A, Krouskou SE, Nikolettos K, Palios VC, Mousios P, Goula K, Konis K, Chionis A, & Kontomanolis EN. Portal Vein Thrombosis after CSection in a Patient with Polycythemia Vera (PV) Due to Pregnancy and Iron Deficiency Anemia (IDA). Clinics and Practice. 2022; 12(6): 1069-1077. https://doi.org/10.3390/clinpract12060109.
- Nuzzo A, & Corcos O. Reversible Acute Mesenteric Ischemia. The New England Journal of Medicine. 2016; 375(15): 31. https:// doi.org/10.1056/NEJMicm1509318.
- Owens CD. JAK2 V617F mutation, mesenteric vein thrombosis, and myeloproliferative disorders. Journal of Vascular Surgery. 2010; 52(1): 205-207. https://doi.org/10.1016/j. jvs.2010.01.097.
- Reinus JF, Brandt LJ, & Boley SJ. Ischemic diseases of the bowel. Gastroenterology Clinics of North America. 1990; 19(2): 319- 343.
- Russell CE, Wadhera RK, & Piazza G. Mesenteric Venous Thrombosis. Circulation. 2015; 131(18): 1599-1603. https://doi. org/10.1161/CIRCULATIONAHA.114.012871.
- Vietti Violi N, Fournier N, Duran R, Schmidt S, Bize P, Guiu B, & Denys A. Acute Mesenteric Vein Thrombosis: Factors Associated With Evolution to Chronic Mesenteric Vein Thrombosis. American Journal of Roentgenology. 2014; 203(1): 54-61. https://doi. org/10.2214/AJR.13.11527.
- Yagi S, Kioka K, Koizumi Y, Nakai T, Kawasaki Y, Tsutsumi M, Ishii N, Yamasaki T, Nebiki H, & Maeda K. Ischemic enteritis resulting from polycythemia vera. Clinical Journal of Gastroenterology. 2022; 15. https://doi.org/10.1007/s12328-022-01673-x.
- Zhang L, Wang Y, Lv W, Hu J, & Gou C. Association of polycythemia vera with non‑cirrhotic portal hypertension in five patients: A case series. Experimental and Therapeutic Medicine. 2023; 25(4): 149. https://doi.org/10.3892/etm.2023.11848.