
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
The use of mandibular guidance prosthesis to correct mandibular deviation following hemimandibulectomy: A case report
Aishwarya Soni*; Shreyans Damade; Swapnil Parlani
Department of Prosthodontics and Crown & Bridge; Peoples College of Dental Sciences and Research Center, Bhopal, India.
*Corresponding Author : Aishwarya Soni
Department of Prosthodontics and Crown & Bridge; Peoples College of Dental Sciences and Research Center, Bhopal, India.
Email: Soni.aish21@gmail.com
Received : Apr 13, 2024
Accepted : May 03, 2024
Published : May 10, 2024
Archived : www.jcimcr.org
Copyright : © Soni A (2024).
Abstract
The most frequent cause of mandibular deviation is surgical mandibular excision for benign or malignant tumors. Mandibular deviation towards the defect side and subsequent loss of occlusion on the unresected side are the consequences of unilateral loss of mandibular continuity occurring from trauma or surgery. A marginal, segmental, hemi, subtotal, or total mandibulectomy may be the surgical treatment option chosen, depending on the location and size of the tumor in the mandible. Mandibular resections can cause significant facial deformity, poor control over salivary secretions, trouble eating, and reduced speech articulation. The restoration of appropriate occlusal function is one of the main objectives of treatment. Guiding flange prosthesis assists the patient in guiding the mandible consistently and naturally during mastication and speech. In dentate individuals, remaining dentition can be used to verify that the mandibular segments have been properly realigned. This can be accomplished by utilizing different guidance prostheses. Following partial mandibulectomy treatments, the guiding prosthesis can successfully retrain the mandible to achieve a functional occlusal relationship, allowing for an early progression to a virtually flawless functioning permanent restoration. Before they can contemplate the final prosthesis, the clinicians need to wait for a long time for the osseous graft to be accepted and healed completely.Prosthodontic intervention is necessary during this first healing phase to stop the mandibular deviation. This clinical report describes the rehabilitation of two patients exhibiting deviation of the mandible following hemimandibulectomy using mandibular guidance prostheses.
Citation: Soni A, Damade S, Parlani S. The use of mandibular guidance prosthesis to correct mandibular deviation following hemimandibulectomy: A case report. J Clin Images Med Case Rep. 2024; 5(5): 3041.
Introduction
Discontinuity of the mandible after surgical resection destroys the balance and symmetry of mandibular function, which leads to altered mandibular movements and deviation of the residual segment towards the defect side, resulting in loss of occlusion on the unresected side. Loss of mandibular continuity causes deviation of remaining mandibular segment (s) towards the defect and rotation of the mandibular occlusal plane inferiorly. This mandibular deviation is mainly due to uncompensated influence of contralateral musculature particularly the internal pterygoid muscle and pull from the contraction of cicatricial tissue on the resected side. The degree of deviation is dependent on several factors which include the location and extent of osseous and soft tissue resection, the method of surgical site closure, degree of impaired tongue function, the presence and condition of the remaining natural teeth, the degree to which innervation has been involved, the use of adjunctive procedures like radiation therapy and the timing of prosthodontics treatment. The other debilitating consequences following resection are impaired speech articulation, difficulty in swallowing, poor control of salivary secretions, and severe cosmetic disfigurement. If, the continuity of the mandible can be restored with a bone graft, metal plates or a combination of both methods, most of the problems of the discontinuity can be resolved [2]. However for some patients who do not desire reconstruction, or who are medically compromised, mandibular guidance therapy can be instituted to retrain the patient’s neuromuscular system to achieve an acceptable occlusion of the remaining natural teeth. The proprioceptive influence of the remaining teeth in the maxilla and the residual mandibular segment can be used to confirm proper realignment of the mandibular fragments to attain repeatable intercuspal position [1]. This can be achieved by the use of various guidance prosthesis. This clinical report describes the rehabilitation of two patients exhibiting deviation of the mandible following hemimandibulectomy using mandibular guidance prostheses [8].
Case report
A 55 yrs old male patient with resected mandible on the left side, for the removal of carcinoma 5 years back, reported to the department of prosthodontics Peoples College of Dental Sciences and Research Centre Bhopal, for prosthetic rehabilitation. The patient had undergone radiation therapy post operatively. However the patient did not go for any prosthetic rehabilitation. The patient’s chief complaint was inability to chew food. He also complained of difficulty in speech and swallowing. Extraoral examination revealed facial asymmetry on the defect side, with hollowed out appearance.
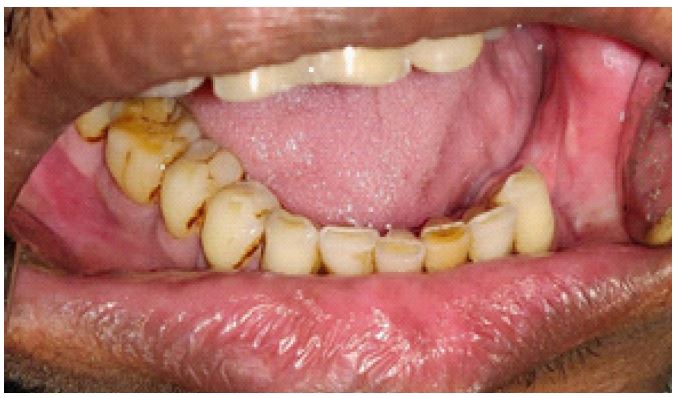
Mandible showed a CLASS 3 defect i.e. Lateral resection of the mandible to the midline (Figure 1).

There was marked deviation of the mandible towards the defect side resulting in disoccclusion of teeth on the normal side. Intraoral examination revealed Teeth present in relation to maxillary left anterior region. The right maxillary anterior and posterior dentition was also intact. Patient was unable to guide the residual mandible to existing occlusion even on application of force.
Diagnosis
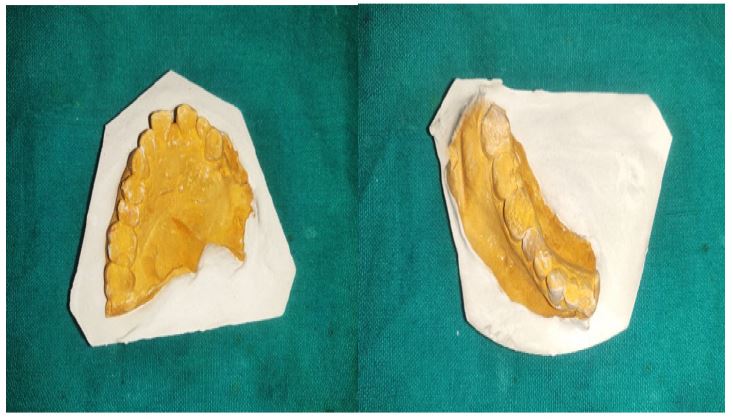
Full mouth radiographs were taken to assess the amount of hard tissue that was left intact and to see the amount of bone that had been resected. The diagnostic Impressions were made of both the upper and lower arches with irreversible hydrocolloid impression material (Figure 2).
The mandible was manually guided into the centric occlusion and a wax interocclusal record was obtained for articulation.

Treatment
Since, it was a longterm case of scarring with marked deviation toward the affected surgical site, a mandible based guidance prosthesis with buccal flange was planned for the patient. Treatment plan with its prognosis was explained to the patient and was accepted by the patient. The guidance prosthesis consisted of a buccal flange extending into the buccal vestibule (Figure 4 ).

The appliance was fabricated in wax before being acrylized in heat cure acrylic resin. The buccal flange was made such that, that it contacted only the buccal surfaces of mandibular and maxillary teeth and it guided - the mandible throughout the opening and closing movements. However the length of the buccal flange was kept sufficient enough to prevent medial deviation of unresected mandible even when the mouth was open (Figure 4). Retention was achieved using interproximal clasps and Adam’s clasps.

The appliance was inserted in the patient’s mouth. The mandible was guided manually so that the residual mandible occluded with the remaining maxillary dentition on the non- defect side. Pressure indicating paste as well as response from the patient was used to locate any regions of soft tissue impingement. The flange was relieved where necessary, by adjusting the acrylic resin. An exercise program was suggested to the patient to assist the patient in improving the symmetrical arc of closure and finding centric occlusal position without guiding the mandible manually. It consisted of simple opening and closure of mandible with and without the appliance and patient grasping the chin and moving the mandible away from the surgical site. After the patient had worn the training flange appliance for a period of 6 months, on the follow up evaluation, he was pleased that more teeth contacted on the right side and that, he was able to chew his food better.
A 38 year old patient who had a resection of the left mandible for the removal of a carcinoma 6 months back reported to the department of prosthodontics at peoples college of dental sciences and research centre, Bhopal, with the chief complaint of lack of contact of the remaining teeth that resulted in inability to chew food effectively. Examination revealed facial asymmetry along with the presence of the scar tissue on the defect side. The mouth opening of the patient was reduced considerably. Mandible exhibited a Class 2 defect i.e. Lateral resection of mandible distal to cuspid (Figure 5).

Maxillary arch showed intact dentition. There was deviation of the mandible towards the defect side thus, disoccclusion of the teeth on the normal side.
Diagnosis
Full mouth radiographs were taken to assess the amount of hard tissue that was left intact and to see the amount of bone that had been resected (Figure 6). Diagnostic Impressions were made of both the upper and lower arches with irreversible hydrocolloid impression material.

The mandible was manually guided into the centric occlusion and a wax interocclusal record was obtained which was then used to mount the diagnostic casts on an articulator.
Treatment
The patient had reduced mouth opening so palatal guide flange guidance prosthesis would be difficult to insert or remove. Therefore, maxillary inclined plane prosthesis was planned for the patient. Treatment plan with its prognosis was explained to the patient and was accepted by the patient. The guidance prosthesis consisted of an occlusal table on the non-defect side which sloped occlusally away from the natural teeth. Because the residual mandible deviated medially, mandibular closure would result in the progressive sliding of the remaining mandibular teeth up the incline in a superior and lateral direction until the occlusal contact is reached. The appliance was fabricated in wax from a functionally generated occlusal record before being acrylized in heat cure acrylic resin. Retention was achieved using Adam’s clasps. Appliance was inserted in the patients mouth and was checked for the progressive sliding of the remaining mandibular teeth up the incline until the occlusal contact was reached. Any high points were checked using an articulating paper and were removed. An exercise program was suggested to the patient same as for the previous patient. After that, the patient had worn the training flange appliance for a period of three months. The occlusion as well as mastication on the non-defect side was restored completely. Once the patient was able to repeatedly approximate the maxillary and mandibular teeth without the use of the guidance prosthesis a definitive prosthesis would be planned. Instructions were given to the patient for maintenance of the oral hygiene and a regular follow up [3].
Discussion
are many surgical treatment options such as marginal, segmental, hemi, subtotal, or total mandibulectomy depending on the location and extent of the tumor in the mandible. A mandibular resection patient is left with numerous physiologic and cosmetic deficits, one of which being an inability to masticate in a way that is efficient or acceptable. It is difficult to provide prosthodontic therapy for these individuals [2]. When a segment of the mandible is removed, immediate reconstruction is usually recommended to improve both facial symmetry and masticatory function. Despite advances in prosthodontic rehabilitation and reconstructive surgery, over half of patients with head and neck cancer who have undergone reconstruction still experience difficulties with their ability to eat and swallow. Mandibular deviation toward the defect side occurs primarily because of the loss of tissue involved in the surgical resection [2]. During this initial healing period early prosthodontic intervention by mandibular guide flange and maxillary stabilization prosthesis serve the purpose of reducing the mandibular deviation, preventing extrusion of the maxillary teeth and improving the masticatory efficiency. Financial constraints of the patients limited our treatment options and precluded the selection of cast partial framework or treatment with dental implants so a simple acrylic obturator was planned for the patient [2]. Usually the material of choice for such cases, with constricted mouth opening. The impression is of an elastomer because of its elasticity and hydrophobic nature which is of benefit in most post-radiation, xerostomic maxillectomy patients. One of the primary goals of treatment is the restoration of acceptable occlusal function. The degree of success is related to the location and extent of the mandibular resection, the amount of adjacent soft tissue removed during surgery and the presence or absence of natural teeth [2]. The methods used to minimize this deviation include use of skin grafts and flaps for wound closure, intermaxillary fixation at the time of surgery, guidance restorations and intensive physiotherapy to decrease fibrosis [2]. The use of simple guidance prosthesis can effectively retrain the mandible after partial mandibulectomy procedures to achieve a functional occlusal relationship which can be maintained throughout the post- operative healing period [1]. The prosthesis components were kept apart in order to avoid disturbing the GFP in the anterior region [4].
The guidance prosthesis that can be used may be:
1. Palatal based guidance prosthesis which include Maxillary inclined plane prosthesis, Positioning prosthesis with palatal flange, widened maxillary occlusal table.
2. Mandibular based guidance prosthesis which include Mandibular lateral/ oblique guide flange prosthesis [1].
Guidance prosthesis has the following advantages:
1. Effectively realigns the residual mandible to occlude with the opposing maxillary dentition.
2. Improved mastication.
3. Improved speech and swallowing.
4. Ease of fabrication and economical.
5. Good patient compliance.
6. Facilitates early progression to an early perfect functioning permanent restoration [1].
The retentive components were modified and incorporated into the prosthesis as a wire substructure. The earlier the mandibular guidance therapy is initiated in the course of treatment, the more successful is the patient’s definitive occlusal relationship [2]. The flange of GFP was localized to three teeth (two premolars and a first molar) to avoid possible dislodging forces in the anterior lingual sulcus area (i.e. junction between mandible and fibula) and to minimize the display due to the esthetic concerns. Though the lingual flange of the GFP was short in length, it was sufficient to stabilize the GFP (in this particular patient) as the deviation force was lesser than the stability of the GFP. The lingual flange extension on the entire lingual surfaces of the three teeth and deep in the lingual sulcus also helps increasing the stability of the prosthesis [2]. The GFP can be extended as long as possible to improve the stability of the appliance as esthetics and comfort permits [2]. The GFP is no different from that of any other removable prosthesis, the natural teeth and the residual alveolar ridge being the primary sources. Multiple retentive clasps in widely distributed areas of the arch would be the best approach, but actual placement would be determined by the position of the teeth. Retentive elements should be no more rigid than necessary, but they require a more rigidity with a decreasing number of teeth [2]. When the prosthetic therapy is combined with a wellorganized exercise regimen, improved results can be achieved within a short span of time [1]. The objective of these exercise programs is to reprogram the remaining musculature, improve the maxillo-mandibular relationship, reduce the scar contracture and to decrease the trismus [1]. This enables the patient to masticate appropriately, to lead a healthy, good quality of life. It also helped patient to deal with the physical and psychological disabilities [3].
References
- Gupta SG, Sandhu D. The use of mandibular guidance prosthesis to correct mandibular deviation following hemimandibulectomy - Case reports.
- Patil PG, Patil SP. Guide flange prosthesis for early management of reconstructed hemimandibulectomy: a case report. J Adv Prosthodont. 2011; 3(3): 172-176. https://doi.org/10.4047/jap.2011.3.3.172.
- Schneider RL, Taylor TD. Mandibular resection guidance prostheses: A literature review. J Prosthet Dent. 1986; 55: 84-6.
- Martin JW, Shupe RJ, Jacob RF, King GE. Mandibular positioning prosthesis for the partially resected mandibulectomy patient. J Prosthet Dent. 1985; 53(5): 678-80.
- Cantor R, Curtis TA. Prosthetic management of edentulous mandibulectomy patients. I. Anatomic, physiologic, and psychologicconsiderations. J Prosthet Dent. 1971; 25(4): 446-57.
- Taylor TD. Diagnostic considerations for prosthodontic rehabilitation of the mandibulectomy patient. In: Taylor TD, editor. Clinical maxillofacial prosthetics. Chicago; Quintessence Publishing; 2000. p. 155-70. 3. Olson ML, Shedd DP. Disability and rehabilitation in head and neck cancer patients after treatment. Head Neck Surg. 1978; 1: 52-8.
- Ravi sureja, Naveen YG, Rajesh Sethuraman, Paranjay Prajapati, Jayatilal R Patel. Twin occlusion prosthesis: a ray of hope for hemimandibulectomy patient- a case report. European journal of dental therapy and research. 2014; 3: 231-33.
- McConnel FM, Teichgraeber JF, Adler RK. A comparison of three methods of oral reconstruction. Arch Otolaryngol Head Neck Surg. 1987; 113: 496-500.
- Pauloski BR, Rademaker AW, Logemann JA, McConnel FM, Heiser MA, Cardinale Set al. Surgical variables affecting swallowing in patients treated for oral/oropharyngeal cancer. Head Neck. 2004; 26: 625-36.
- Desjardins RP. Occlusal considerations for the partial mandibulectomy patient. J Prosthet Dent. 1979; 41(3): 308-15.