
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Antenatally detected megaurethra: A challenging prenatal diagnosis of Prune Belly syndrome
Ben El Haj Chirine1*; Ben Ali Azza1; Chaibi Onss2; Masmoudi Aida3; Douira Khomsi Wiem4
1Department of Pediatric Medical Imaging, Radiology Resident, Bechir Hamza Hospital, Beb Saadoun, Tunisia.
2Department of Pediatric Medical Imaging, Radiology Consultant, Bechir Hamza Hospital, Beb Saadoun, Tunisia.
3Department of Embryo-Foetopathology, Professor in Embryology, Maternity Center, Tunis, Tunisia.
4Chief of Pediatric Medical Imaging Department, Radiology Professor, Bechir Hamza Hospital, Beb Saadoun, Tunisia.
*Corresponding Author : Ben El Haj Chirine
Department of Pediatric Medical Imaging, Radiology Resident, Bechir Hamza Hospital, Medical University of Tunis, Beb Saadoun, Tunisia.
Tel: +21-627185409;
Email: benelhajchirine@gmail.com
Received : Mar 05, 2024
Accepted : May 03, 2024
Published : May 10, 2024
Archived : www.jcimcr.org
Copyright : © Chirine BEH (2024).
Abstract
Prune Belly Syndrome (PBS) is a rare congenital disorder characterized by a triad of urinary tract dilatation, abdominal wall musculature deficiency and bilateral cryptorchidism. Here, we present a case report of a 31-year-old woman referred to our department for ultrasound examination at 22 weeks and 2 days of gestation due to fetal bladder dilation. Ultrasound findings revealed bilateral ureterohydronephrosis, megacystis, dilated proximal and penile urethra, empty scrotal sacs suggestive of cryptorchidism, and muscle hypoplasia in the abdominal wall. Additionally, a cleft palate was detected. Following counseling, the parents opted for medical termination of pregnancy due to the poor prognosis associated with potential renal and sexual dysfunctions. Autopsy confirmed the prenatal diagnosis of PBS in the 385 g male fetus, while the cleft palate diagnosis was inconclusive, with evidence of a cup-shaped hard palate. This case underscores the importance of recognizing the association between megaurethra and PBS, as it can lead to severe manifestations and necessitate careful management to mitigate potential complications, particularly in prenatal diagnosis and counseling scenarios.
Keywords: Prune belly syndrome; Urinary tract dilatation; Megaurethra; Prenatal diagnosis; Abdominal wall musculature deficiency.
Abbreviations: PBS: Prune Belly Syndrome.
Citation: Chirine BEH, Azza BA, Onss C, Aida M, Wiem DK. Antenatally detected megaurethra: A challenging prenatal diagnosis of prune belly syndrome. J Clin Images Med Case Rep. 2024; 5(5): 3042.
Introduction
Dilatation of anterior urethra, also known as megaurethra, is a rare congenital malformation caused by primary or secondary agenesis of corpora spongiosa and cavernosa. Its association with Prune Belly syndrome has been postulated by some authors as it’s a form of lower urinary tract obstruction resulting in bilateral ureterohydronephrosis and thus abdominal distension with defect in the development of abdominal wall musculature layers and failure of both testes to descend into the scrotum (bilateral cryptorchidism).
Researchers in a review of literature [1] reported 10 cases of antenatally diagnosed megaurethra with their autopsy/clinical findings showing the different associations with other malformations and syndromes. Prune belly syndrome was found in 3 cases out of 10. Other associations with imperforate anus, clubfoot, sacrum malformation and hypospadias were found.
Prune belly syndrome is a rare congenital disorder that mainly affects male sex with an incidence of 1:35,000 to 1:50,000 live births [2]. It is characterized by a triad of urinary tract dilatation, abdominal wall musculature deficiency and bilateral cryptorchidism.
Therefore, it is imperative to check for Prune belly syndrome triad in the presence of megaurethra as it is a severe manifestation of this disorder that may cause renal dysplasia and oligohydramnios, which in certain circumstances may result in pulmonary hypoplasia [3].
Case presentation
We report the case of a 31-year-old women, gravida 3, para 1 (1 dead baby and 1 alive baby), was referred to our department for an ultrasound examination at 22 weeks and 2 days of gestation for a dilated urinary fetal bladder. We noted a consanguineous marriage with unremarkable family history.
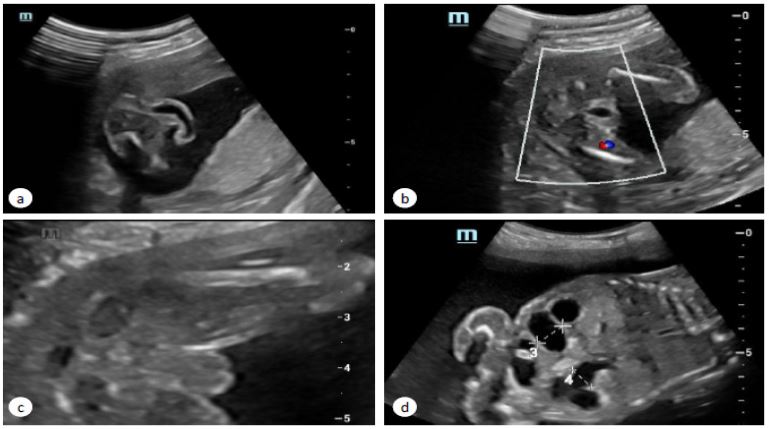
The ultrasound evaluation revealed a single viable male fetus with bilateral ureterohydronephrosis, megacystis presenting a thick wall, dilated proximal urethra and a marked dilatation of the penile urethra. Ultrasound also demonstrated bilateral empty scrotal sac free of echogenicity suggestive of cryptorchidism. In addition, we noted polyhydramnios and a flabby abdominal wall with muscle hypoplasia (Figures 1,2). On the other hand, ultrasound detected a cleft palate.
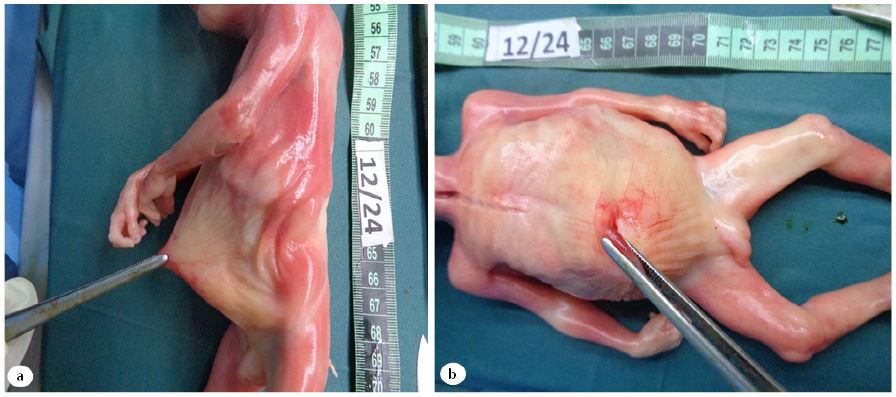
After receiving counseling, the parents opted for medical termination of the pregnancy, mostly due to the poor prognosis brought on by the increased likelihood of serious renal and sexual dysfunctions.The autopsy of the 385 g male fetus confirmed the prenatal diagnosis of Prune belly syndrome (Figures 3-5). The cleft palate diagnosis was declined. However, the autopsy did found a deep cup-shaped aspect of the hard palate.
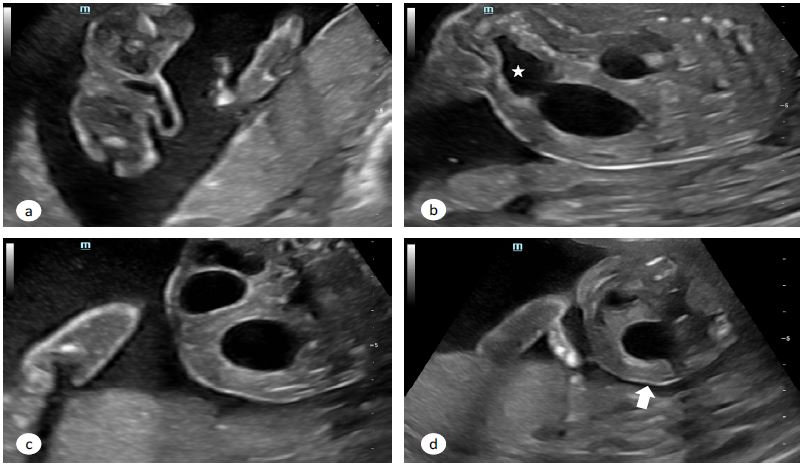
(a) Shows penile urethral dilatation (megaurethra). (b): Shows enlargement of urinary bladder (megacystis) and dilated proximal urethra (asterixis) responsible for keyhole appearance of bladder. (c) Demonstrates bilateral hydronephrosis. (d) Shows a flabby appearance of the abdominal wall with hypoplastic muscles (arrow).


Discussion
Prune-Belly Syndrome, also referred to as Eagle-Barrett syndrome or triad syndrome, is characterized by a combination of deficiency of abdominal wall muscles, bilateral undescended testes and urological abnormalities [4]. In cases where all components of the classic triad aren’t present, it is termed pseudoprune-belly syndrome. The name “prune belly” stems from the wrinkled appearance of the abdominal skin due to the lack of development of abdominal muscles.
The precise cause of Prune-Belly Syndrome remains unclear. Various theories suggest a fetal insult leading to inadequate development of abdominal muscles or muscle atrophy due to chronic distention of the abdomen in utero [5]. Additionally, a familial form of the syndrome exists, though its transmission mode remains uncertain. While Prune-Belly Syndrome predominantly affects males, the familial form shows a slightly higher incidence in females [6].
Structural abnormalities within the genitourinary tract are common, including renal dysplasia of varying degrees, possible bilaterally dilated and tortuous ureters, such the case with our patient, and a capacious bladder often associated with a urachal remnant like a diverticulum or fistula [7].
Urethral abnormalities, such as hypoplasia or atresia, may also be present. Nunn et al. found urethral abnormalities in all the cases diagnosed with Prune Belly syndrome [5]. In our case, we noted a dilated proximal urethra and a marked dilatation of the penile urethra.
The kidneys can be small, with or without dilation of the collecting system. It is important to note that the anatomic abnormalities of the urinary tract in patients with prune-belly syndrome may be caused by primary, intrinsic, and diffuse defects of embryologic development of the structures involved, which are different from the discrete lesions of obstruction or reflux that may occur in the urinary tract of otherwise normal newborns [8]. However, the abnormalities may appear similar to those that occur in prune-belly syndrome. For example, the large, thick-walled bladder of patients with prune-belly syndrome may occur in the absence of bladder outlet obstruction, although the bladder may bear a resemblance to that of a patient with PUV. Similarly, although ureteral dilation in otherwise normal infants is commonly associated with vesicoureteral reflux or obstruction, a similar ureteral lesion in a patient with prune-belly syndrome may occur in the absence of reflux or obstruction [1].
Prune-Belly Syndrome is often associated with musculoskeletal, cardiovascular, gastrointestinal and pulmonary anomalies. Crompton et al. [9]. Evaluated respiratory function in 11 patients with prune-belly syndrome. Nine had evidence of gas trapping and six of restrictive lung disease. Gastrointestinal anomalies include malrotation, imperforate anus, and Hirschsprung’s disease. Congenital cardiac disease includes atrial septal defect, tetralogy of Fallot and ventricular septal defect. Lung hypoplasia is a severe associated anomaly that will determine the prognosis in the neonatal period.
Patients with prune-belly syndrome often have additional problems, including scoliosis due to weakened abdominal muscles, Potter facies (flattening of the nose, redundant skin, recedingchin, ocular hypertelorism, and low-set ears), hip dislocation or subluxation, talipes equinovarus. Loder et al [10], studied 12 cases of Prune Belly syndrome and found 9 cases having musculo-squelettic abnormalities.
Sonographic evaluation can reveals dilated and tortuous ureters, bilateral hydronephrosis, and dysmorphic or cystic changes in the kidneys [1,2,4,11]. Voiding cystourethrography commonly shows a large, elongated bladder, often with anurachal diverticulum or fistula, with 85% of patients exhibiting vesicoureteral reflux, usually bilateral [2,11].
Prognosis varies among patients, with some experiencing significant genitourinary abnormalities and pulmonary hypoplasia, leading to stillbirth or early death, while others may have adequate renal function but remain at risk for obstruction, sepsis, and chronic renal failure, often resulting in death within the first two years of life. Notably, dilatation of the urinary tract does not necessarily correlate with renal function [8].
Features of prune bell syndrome can be diagnosed by prenatal ultrasonography, especially in the second trimester while identifying the classic findings of ureterohydronephrosis, megacystis, dilated proximal urethra and muscle hypoplasia of the in the abdominal wall.
Conclusion
The case highlights the critical role of prenatal ultrasound in early detection of Prune Belly syndrome, particularly through recognition of associated megaurethra. Timely identification enables informed decision-making and tailored management strategies, underscoring the importance of early intervention in optimizing patient outcomes.
Declarations
Conflict of interest statement: The authors have no conflicts of interest to declare.
Ethical consideration: Written informed consent was obtained from the parents regarding the publication of this case report and images.
References
- Amsalem H, et al. Congenital megalourethra: Prenatal diagnosis and postnatal/autopsy findings in 10 cases. Ultrasound Obstet. Gynecol. 2011; 37: 678-683.
- Xu, W., Wu, H., Wang, D.-X. & Mu, Z.-H. A Case of Prune Belly Syndrome. Pediatr. Neonatol. 2015; 56: 193-196.
- Prune Belly Syndrome - an overview ScienceDirect Topics. https://www.sciencedirect.com/topics/medicine-and-dentistry/prune-belly-syndrome.
- Sutherland RS, Mevorach RA, Kogan BA. The prune-belly syndrome: Current insights. Pediatr. Nephrol. 1995; 9: 770-778.
- Nunn IN, Stephens FD. The Triad Syndrome: A Composite Anomaly of the Abdominal Wall, Urinary System and Testes. J. Urol. 1961; 86: 782-794.
- Ramasamy R, Haviland M, Woodard JR, Barone JG. Patterns of inheritance in familial prune belly syndrome. Urology. 2005; 65: 1227.
- Das Narla L, Doherty RD, Hingsbergen EA, Fulcher AS. Pediatric case of the day. Prune-belly syndrome (Eagle-Barrett syndrome, triad syndrome). RadioGraphics. 1998; 18: 1318-1322.
- Woodhouse CR, Ransley PG, Innes-Williams D. Prune belly syndrome-report of 47 cases. Arch. Dis. Child. 1982; 57: 856-859.
- Crompton CH, MacLusky IB, Geary DF. Respiratory function in the prune-belly syndrome. Arch. Dis. Child. 1993; 68: 505-506.
- Loder RT. Musculoskeletal Aspects of Prune-Belly Syndrome: Description and Pathogenesis. Am. J. Dis. Child. 1992; 146: 1224.
- Nunn, I. N. & Stephens, F. D. The Triad Syndrome: A Composite Anomaly of the Abdominal Wall, Urinary System and Testes. J. Urol. 1961; 86: 782-794.