
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Acute posterior multifocal placoid pigment epitheliopathy (APMPPE): Case report
Monika Sarna; Michal Wilczynski; Arleta Waszczykowska*
Department of Ophthalmology, Medical University of Lodz, Poland.
*Corresponding Author : Arleta Waszczykowska
Department of Ophthalmology, Medical University of Lodz, Poland.
Tel: +48-42-67-76-800;
Email: [email protected]
Received : Apr 16, 2024
Accepted : May 06, 2024
Published : May 13, 2024
Archived : www.jcimcr.org
Copyright : © Waszczykowska A (2024).
Abstract
An 18-year-old patient came to our Ophthalmology Department due to significant bilateral vision loss. The vision impairment in the left eye, lasting for ten days, had progressively worsened. There was a sudden deterioration of visual acuity in the right eye for two days. The ophthalmological symptoms followed an infection likely of viral origin. On the day of admission, the Best Corrected Visual Acuity (BCVA) was 0.9 in the right eye and 0.025 in the left eye. The anterior segment and vitreous body of both eyes showed no signs of inflammation. Multiple yellow-white, plaque-like lesions of the retina and choroid were observed in both eyes. A diffuse area of damage with foveal involvement was visible in the left eye.
The performed examinations of Optical Coherence Tomography Angiography (OCTA), optical coherence tomography, fluorescein angiography, fundus autofluorescence, electroretinography and visual field enabled the diagnosis of Acute Posterior Multifocal Placoid Pigment Epitheliopathy (APMPPE). The patient’s immunogenetic test showed the presence of HLA-B15 and HLA-B35.
Due to bilateral macular involvement, significantly reduced BCVA and previous infection, treatment with oral methylprednisolone and intravenous acyclovir was administered. BCVA improved after just one day of treatment. BCVA was then 0.9 in the right eye and 0.25 in the left eye. After 5 weeks of treatment, the patient regained full visual acuity in both eyes.
The clinical case we describe enriches knowledge about the disease and underscores the crucial role of optical coherence tomography angiography in its diagnosis. It also highlights the effectiveness of treatment with methylprednisolone and acyclovir in APMPPE cases preceded by a viral infection.
Keywords: APMPPE; Treatment; HLA; OCT; OCTA; Vascular changes.
Abbreviations: APMPPE: Acute Posterior Multifocal Placoid Pigment Epitheliopathy; OCT: Optical Coherence Tomography; OCTA: Optical Coherence Tomography Angiography BCVA: Best Corrected Visual Acuity; ERG: Electroretinogram; RPE: Retinal Pigment Epithelium; FAF: Fundus Autofluorescence; CRP: C-Reactive Protein; SARS: Cov-2- Severe Acute Respiratory Syndrome Coronavirus 2; RSV: Respiratory Syncytial Virus; HLA: Human Leukocyte Antigens; MRI: Magnetic Resonance Imaging; FA: Fluorescein Angiography; HIV1: Human Immunodeficiency Virus Type 1; HIV2: Human Immunodeficiency Virus Type 2; HBV: Hepatitis B Virus; HCV: Hepatitis C Virus.
Citation: Sarna M, Wilczynski M, Waszczykowska A. Acute posterior multifocal placoid pigment epitheliopathy (APMPPE): Case report. J Clin Images Med Case Rep. 2024; 5(5): 3045.
Introduction
Acute Posterior Multifocal Placoid Pigment Epitheliopathy (APMPPE) is a rare disease, first described by Gass [1] in 1968. The disease presents with sudden, bilateral vision loss, without gender predilection, more commonly affecting young and middle-aged individuals, and in one-third of cases preceded by a flu-like infection [2,3]. Defining the primary site of inflammation is challenging clinically due to the interdependence of the vascular membrane and the retina. The pathophysiology of the disease is not fully understood. It is believed that inflammation leads to choriocapillaris occlusion and secondary hypoxia of the adjacent retina. Choriocapillaris nourish the outer layers of the retina, while the RPE provides nutrients and growth factors to the retina and removes metabolites. Choriocapillaris hypoperfusion results in damage to the Retinal Pigment Epithelium (RPE) and secondary atrophy of the choroid and adjacent photoreceptors [4,5]. Treatment of APMPPE remains controversial as many clinicians believe the disease resolves spontaneously [6].
The gold standard for diagnosing APMPPE remains Optical Coherence Tomography Angiography (OCTA), which allows non-invasive assessment of blood flow through the retinal and choroidal vessels [7,8].
Based on the evolution of choriocapillaris changes observed in OCTA, four stages of the disease are distinguished: choroidal, chorioretinal, transitional, and resolution phase. In the first “choroidal” phase, only choriocapillaris hypoperfusion may be visible in OCTA, while Optical Coherence Tomography (OCT) and Fundus Autofluorescence (FAF) results are normal. At this stage, the disease may completely resolve or progress to the next “chorioretinal” phase. During the second phase, in addition to persistent choriocapillaris hypoperfusion, characteristic changes occur in the outer retinal layers as hyper-reflectivity and loss of integrity. These changes are hypoautofluorescent. In the third “transitional” phase, persistent choriocapillaris hypoperfusion, thinning of the outer retinal layers, and progressive central hyperautofluorescence are noted. In the final “resolution” phase, normalization of choriocapillaris flow occurs with persistent thinning of the outer retinal layers and hypo-reflectivity of RPE. FAF shows intensified hypoautofluorescence [5,7,8].
Case presentation
An 18-year-old patient came to the Clinical Department of Ophthalmology in Norbert Barlicki University Teaching Hospital No. 1 in Lodz, Poland, due to bilateral, significant loss of visual acuity. Vision impairment in the left eye had lasted for approximately ten days and had intensified over time. There had been a sudden deterioration of visual acuity in the right eye for two days. The patient reported a gray ‘spot’ in the center of the visual field of the left eye and several smaller gray dots in the right eye’s visual field. The ophthalmological symptoms were preceded by an infection of probable viral etiology. On the day of admission, the patient reported significant body weakness, headache and mentioned that he’d had upper respiratory tract infection ten days before. The patient denied having chronic diseases, taking chronic medications, contacting with animals, eating raw meat, having risky sexual contacts, contacting with a person suffering from tuberculosis, having joint pain, or disturbing skin lesions, as well as autoimmune diseases and cancer in the family.
A week before coming to our department, the patient had an ophthalmological examination in another hospital. He then reported decreased visual acuity in the left eye that had been present for several days. Slit lamp examination and ultrasound examination did not reveal any abnormalities. Best Corrected Visual Acuity (BCVA) was 1.0 in both eyes. OCTA examination was not performed at that time. The patient received treatment with ascorbic acid and rutoside orally and pranoprofen and dexamethasone drops topically to the left eye. Clinical symptoms suggest that the patient may have been in the choroidal phase of the disease at the time.
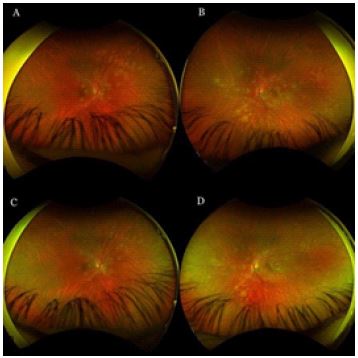
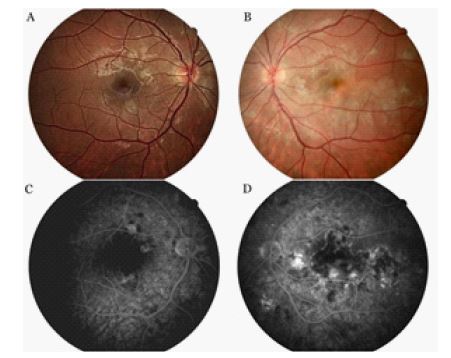
On the day of admission to our department the patient was already presenting the chorioretinal phase of the disease. The best corrected visual acuity in the left eye was 0.025 and 0.9 in the right eye. On physical examination, the anterior segment and vitreous body of both eyes showed no signs of inflammation. In the right eye, scattered yellow-white lesions of the retina and choroid were observed, located near the optic disc, in the upper hemisphere of the retina and three foci were present in the macula. In the left eye, there were more numerous, plaque-like lesions, forming a diffuse area of damage, with involvement of the fovea. There were many smaller, scattered lesions on the mid-periphery of the retina in the left eye (Figure 1).
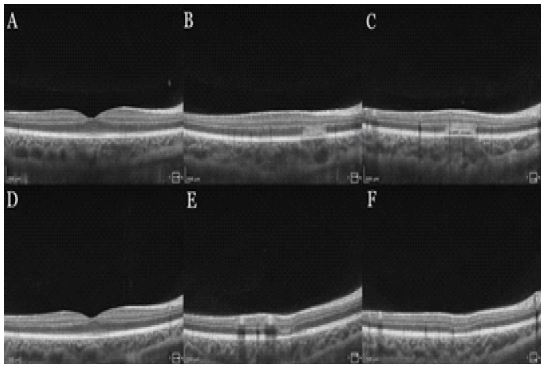
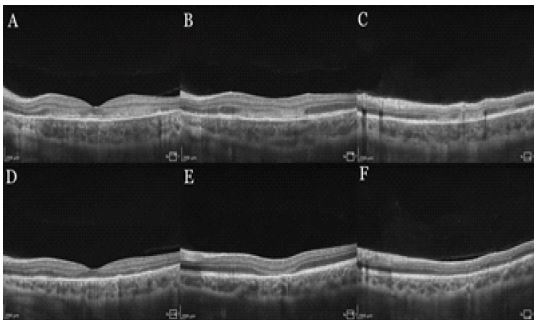
OCT scans (SOCT REVO NX 130, Optopol) of both eyes showed active, hyperreflective changes in the outer layers of the retina, a distorted line of photoreceptors and RPE. There was thickening of the uveal membrane, which suggested inflammation (Figures 2,3).
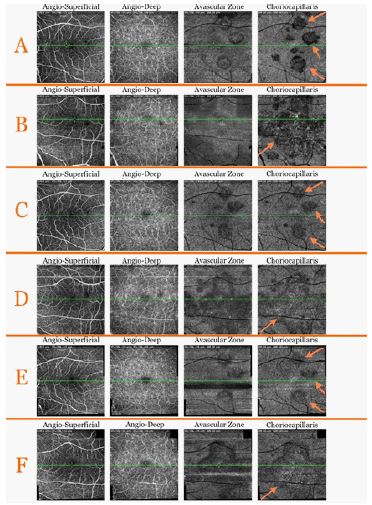
Ischemic changes were observed at the choriocapillaris level of both eyes on OCTA scans, the right eye had ischemic lesions and the left eye had a diffuse area of ischemia (Figure 4).
The superficial capillary plexus vessel density ratio of the examined macular area was 34.3% in the right eye and 37.1% in the left eye.
The second examined parameter was the deep capillary plexus vessel density ratio of the examined macular area, which was 38.8% in the right eye and 38% in the left eye.
Fluorescein Angiography (FA) showed early hypofluorescence secondary to decreased choriocapillaris perfusion and RPE thickening, as well as patchy hyperfluorescence with dye staining, unevenly saturating the lesions (Figure 5).
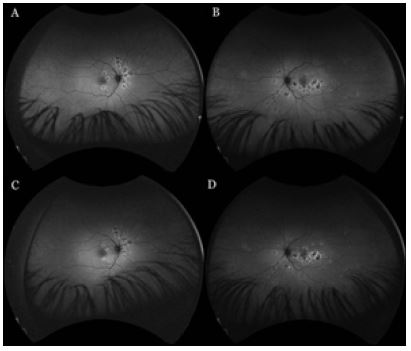
Fundus autofluorescence showed hypoautofluorescence at sites of retinal pigment epithelium damage with hyperautofluorescence at the periphery of the lesions (Figure 6).
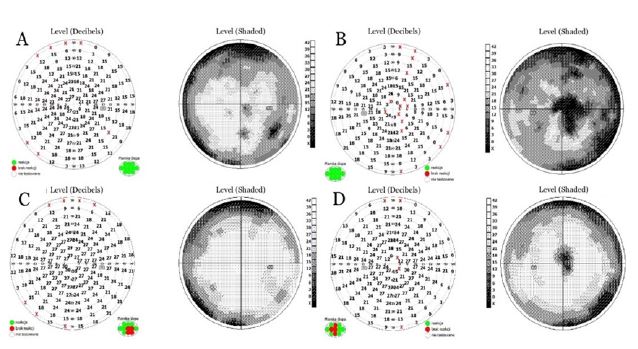
The result of the visual field test showed paracentral scotomas and confluent arcuate scotomas, narrowing the visual field lunette-like in the right eye. The left eye had a significant, generalized decrease in retinal sensitivity to light stimuli, a large central scotoma and confluent, dense, arcuate scotomas, narrowing the visual field lunette-like (Figure 7).
The Electroretinogram (ERG) consisted of slightly reduced values of the a- and b- waves’ amplitudes in the right eye, significantly reduced waves’ amplitude in the left eye, normal morphology and physiological waves’ latency (Figure 8).
A complete blood count, an erythrocyte sedimentation rate and a C-Reactive Protein (CRP) tests were performed, which results were within normal limits. Diagnostics were performed to check for active infection, which could present a similar clinical picture. Due to an upper respiratory tract infection, an antigen test was performed to detect SARS-CoV-2, Respiratory Syncytial Virus (RSV) and Influenza type A and B infection. The test result was negative.
Based on the normal level of angiotensin-converting enzyme, the physiological chest radiograph and the absence of typical clinical symptoms, sarcoidosis was excluded.
The immunogenetic test showed the presence of HLA-B15 and HLA-B35 antigens but excluded the presence of the HLA-B7 antigen.
Magnetic Resonance Imaging (MRI) of the brain was performed to exclude the accompanying intracerebral vasculitis. No perivascular inflammation or other pathological features were observed in the MRI examination. Next, a neurological consultation was performed, during which Vogt-Koyanagi- Harada syndrome was excluded.
The above tests allowed us to perform accurate differential diagnosis. The presence of sarcoidosis, tuberculosis, syphilis, Lyme disease, as well as infection with HIV1, HIV2, HBV, HCV, SARS-CoV-2 and RSV viruses were excluded.
On the day of admission, systemic steroid therapy and antiviral treatment were started. Intravenous dexamethasone was used during hospitalization. Intravenous acyclovir at a dose of 5 mg/kg/3 times per day had been used for 5 days. After the first day of treatment, a significant improvement in visual acuity in the left eye was observed. The best corrected visual acuity was then 0.9 in the right eye and 0.25 in the left eye.
The patient was discharged from the hospital with a recommendation to continue using steroids. Oral methylprednisolone was recommended at a dose of 0.8 mg/kg/day with a slow reduction of steroid therapy for a period of 7 weeks. On the day of discharge from the hospital, the patient’s corrected visual acuity was 1.0 in the right eye and 0.32 in the left eye.
The first follow up visit took place nine days after the end of hospitalization. The patient reported subjective improvement in visual acuity and visual field. Best corrected visual acuity in the right eye was 0.9 and 0.5 in the left eye. There were no abnormalities in the physical examination of the anterior segment and vitreous body of both eyes. In the eye fundus of the right and left eye, light yellow, speckled inflammatory lesions with a smaller area were visible compared to the day of discharge from the hospital. Oral steroidal therapy was continued in slowly decreasing doses for a period of 7 weeks.
Three weeks after hospitalization, the patient’s BCVA was 1.0 in the right eye and 0.9 in the left eye. The patient entered the transitional phase five weeks after hospitalization. The patient’s visual acuity in both eyes was 1.0. Physical examination of the anterior segment and vitreous body of both eyes was still normal. In the eye fundus of the right and left eyes, light yellow, speckled lesions were visible, smaller in number and in area compared to previous examinations (Figure 1).
Inflammatory lesions were still visible in OCT scans, but with a smaller diameter and thickness than during hospitalization (Figures 2,3).
OCTA of the macula showed a reduction in the size and intensity of choriocapillaris lesions (Figure 4). The superficial capillary plexus vessel density of the examined macular area was 42.2% in the right eye and 38.8% in the left eye.
The deep capillary plexus vessel density of the examined macular area was 43.5% in the right eye and 40.6% in the left eye.
In the fundus autofluorescence hypoautofluorescence was observed in the areas of damage to the retinal pigment epithelium and hyperautofluorescence at the periphery of the lesions (Figure 6).
The visual field test in the right eye showed confluent arcuate defects. The visual field of the left eye showed an increase in retinal sensitivity to light stimuli, a smaller central scotoma and arcuate defects (Figure 7). The patient’s field of vision improved significantly.
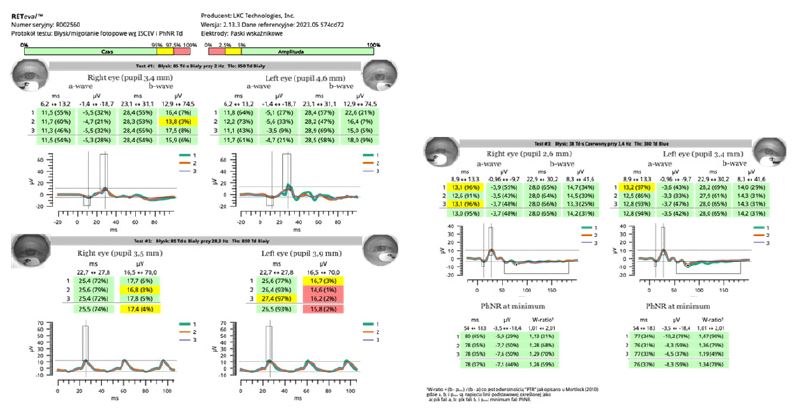
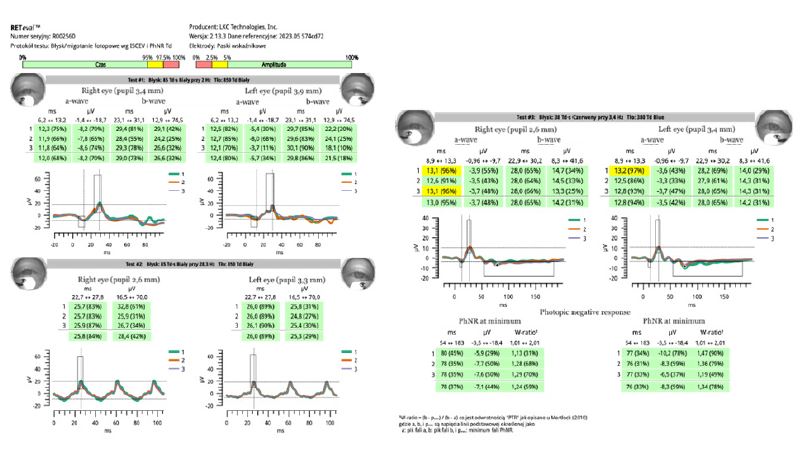
The ERG of both eyes consisted physiological values of the a- and b-waves’ amplitudes, normal waves’ latency and morphology (Figure 9).
Fourteen weeks after hospitalization the patient was still in the transitional phase. BCVA in both eyes was 1,0. OCTA scans reveled a reduction in intensity of choriocapillaris lesions (Figure 4). After this time, the disease had not yet reached the resolution phase.
Discussion
Acute posterior multifocal placoid pigment epitheliopathy is a severe disease that affects young adults [4]. The primary cause is believed to be choriocapillaris damage leading to hypoperfusion and secondary damage to the outer retinal layers. [4,5].
In the pathophysiology of APMPPE, immune system response to an infectious agent or direct cell infection through the angiotensin converting enzyme 2 receptor is considered [3]. Cases of post- vaccination occurrence of APMPPE have been described in the literature. Jakirlic et al. [9] described the occurrence of acute posterior multifocal placoid pigment epitheliopathy after vaccination against SARS-CoV-2. Our patient’s disease was preceded by an upper respiratory tract infection of probable viral etiology. Clinical studies in patients with APMPPE indicate a higher prevalence of tissue antigens HLA-B7 and HLA-DR2 than in healthy individuals [10]. This suggests an immunogenetic predisposition to the disease, confirmed by observations of Kim et al. [11], who described recurrent APMPPE in two HLA-DR2 positive cousins. Immunogenetic testing of our patient revealed the presence of HLA-B15 and HLA-B35, while excluding the presence of HLA-B7 and HLA-DR2. HLA-B15 and HLA-B35 antigens indicate an increased risk of autoimmune diseases. Individuals with HLA-B35 have an increased risk of retinal vasculitis in idiopathic autoimmune choroiditis and kidney inflammation in IgA-associated vasculitis [12,13]. Increased occurrence of HLA-B15 has been observed in individuals with ankylosing spondylitis [14]. IgA-associated vasculitis involves leukocytoclastic inflammation of small vessels with IgA deposition [13]. Additionally, like APMPPE, it may be preceded by infection [15,16]. Ankylosing spondylitis is an inflammatory disease of unknown etiology. Potential causes of the disease include autoimmune reactions, genetic predispositions, and environmental factors [17].
The main role in the diagnosis and monitoring of APMPPE is played by optical coherence tomography angiography [7,8]. So far, changes in retinal blood vessels in APMPPE have not been described in the literature. In order to expand knowledge about the pathophysiology of the disease, we conducted additional research in this direction. The OCT manufacturer’s software allowed us to detect changes in retinal vasculature. This was possible by comparing vessel density coefficients of the superficial and deep retinal plexuses in the patient’s macular area.
The first analyzed parameter was the vessel density coefficient of the superficial plexus of the studied macular area. During hospitalization, this coefficient was 34.3% in the right eye and 37.1% in the left eye. After 5 weeks of treatment, an increase of 7.9% in the right eye and 1.2% in the left eye was observed.
The second analyzed parameter was the vessel density coefficient of the deep plexus of the studied macular area. During hospitalization, this coefficient was 38.8% in the right eye and 38% in the left eye. After 5 weeks of treatment, an increase of 4.7% in the right eye and 2.6% in the left eye was observed. These results indicate a decrease in retinal vessel density during the course of the disease, followed by an increase in vessel density in both retinal plexuses after 5 weeks of treatment, indicating retinal circulation regeneration and further confirming the effectiveness of the treatment.
To assess the severity of the disease, we performed an electrophysiological examination of ERG, the aim of which was to determine the response of retinal photoreceptors. The ERG is an objective examination [18]. In ERG performed during hospitalization, we observed the reduction of the a- and b- waves’ amplitude in both eyes. A simple reduction in amplitude is usually associated with limited loss of retinal function [18]. In the follow-up examination performed 5 weeks after hospitalization, we observed normalization of the a- and b- waves’ amplitude in both eyes, which indicates an improvement in the electrical response of the retina and resolution of the disease. The ERG was useful in monitoring the disease progression and confirming the effectiveness of the applied treatment.
The treatment of APMPPE has not been clearly defined. The disease often does not require treatment due to its self-limiting course [6]. In cases involving the macula or central nervous system, systemic steroid therapy is recommended [5,19]. Treatment should be individualized to the patient’s needs, which may pose therapeutic challenges and uncertainties. Various treatment methods are described in the literature. Oliveira et al. [8] used methylprednisolone at a dose of 1 mg/kg/day in a patient with macular involvement. Other authors decided not to administer any treatment Xerii et al. [6].
Did not administer pharmacological treatment to patients with macular involvement, achieving complete patient recovery after 10 months of observation. Similarly, Jakirlic et al. [9]. initially did not administer treatment to a patient with post-vaccination APMPPE. However, after 42 days of patient observation, inflammatory changes in the vitreous body developed. Oral prednisone was then successfully administered in tapering doses over a period of 5 weeks [6].
Brydak-Godowska J et al. [20] described the case of 7 patients with APMPPE, who were treated with prednisone or acyclovir or both. The visual acuity had fully returned in 6 out of 7 people Chan A et al.
Chan A et al [21] described the case of an 18-year-old woman with macular involvement treated with intravenous acyclovir and intravitreal ganciclovir.
The patient discussed in our case presented with bilateral macular involvement, with involvement of the fovea in the left eye. A lower dose of medication 0.8 mg/kg/day of methylprednisolone, was administered compared to previously used doses in APMPPE with a similar course. Moreover, our patient was treated with intravenous acyclovir, which has been used in very few reported cases.
The patient achieved full visual acuity after 5 weeks of therapy, confirming the effectiveness of the treatment. The patient remains under close ophthalmological observation.
Cases of APMPPE with a similar course have been described in the scientific literature [8,22]. Our work additionally includes the results of OCT, OCTA, ERG, visual fields and fundus autofluorescence, which enriches the current knowledge about the disease, enables understanding of its course and provides a useful tool for its diagnosis.
Conclusion
The presented case of acute posterior multifocal placoid pigment epitheliopathy emphasizes the crucial role of optical coherence tomography angiography in the diagnosis of the disease. In severe APMPPE cases with bilateral macular involvement, the use of methylprednisolone at a dose of 0.8 mg/kg/day proved to be sufficient and effective. Adding antiviral treatment for APMPPE cases preceded by viral infection may be helpful. During treatment, functional aspects of the retina improved before anatomical repair. Performing OCTA examination and measuring retinal vessel density during APMPPE may be a useful tool in monitoring the course of the disease and in determining the effectiveness of treatment. Improvement in retinal vascularization, especially in the initially more diseased eye, suggests a response to treatment in APMPPE, although concerns about long-term vascular damage remain.
Conflicts of interest: The authors report no conflict of interest.
References
- Gass JD. Acute posterior multifocal placoid pigment epitheliopathy. Arch Ophthalmol. 1968; 80: 177-85.
- Fischer NA, Wann RC, Crosson JN. Acute posterior multifocal placoid pigment epitheliopathy following COVID-19 infection. Am J Ophthalmol Case Rep. 2023; 29:101790.
- Lund-Andersen C, Klefter ON, Schneider M. Long-term follow-up of a bilateral acute posterior multifocal placoid pigment epitheliopathy following COVID-19 infection: A case report. J Ophthalmic Inflamm Infect. 2024; 4(14): 2.
- Jones NP. Acute posterior multifocal placoid pigment epitheliopathy. Br J Ophthalmol. 1995; 79: 384-9.
- Testi I, Vermeirsch S, Pavesio C. Acute posterior multifocal placoid pigment epitheliopathy (APMPPE). J Ophthalmic Inflamm Infect. 2021; 1(11): 31.
- Xerri O, Salah S, Monnet D, Brézin AP. Untreated Acute Posterior Multifocal Placoid Pigment Epitheliopathy (APMPPE): a case series. BMC Ophthalmol. 2018; 20(18): 76.
- Burke TR, Chu CJ, Salvatore S, Bailey C, Dick AD, et al. Medscape. Application of OCT-angiography to characterise the evolution of chorioretinal lesions in acute posterior multifocal placoid pigment epitheliopathy. Eye (Lond). 2017; 31: 1399-1408.
- Oliveira MA, Simão J, Martins A, Farinha C. Management of Acute Posterior Multifocal Placoid Pigment Epitheliopathy (APMPPE): Insights from Multimodal Imaging with OCTA. Case Rep Ophthalmol Med. 2020; 13(2020): 7049168.
- Jakirlic N, Harris T. Case Report: Acute Posterior Multifocal Placoid Pigment Epitheliopathy after SARS-CoV-2 Vaccination. Optom Vis Sci. 2022; 1(99): 534-539.
- Wolf MD, Folk JC, Panknen CA, Goeken NE. HLA-B7 and HLA-DR2 antigens and acute posterior multifocal placoid pigment epitheliopathy. Arch Ophthalmol. 1990; 108: 698-700.
- Kim RY, Holz FG, Gregor Z, Bird AC. Recurrent acute multifocal placoid pigment epitheliopathy in two cousins. Am J Ophthalmol. 1995; 119: 660-662.
- Visalakshy J, Surendran S, Ganu S, Shah K, Mithun CB, et al. Describing the Clinical and Laboratory Features and HLA-B Pattern of Adult-Onset Idiopathic Autoimmune Uveitis at a Tertiary Hospital in South India: A Cross-Sectional Study. ScientificWorldJournal. 2022; 8(2022): 5032881.
- Amoli MM, Thomson W, Hajeer AH, Calviño MC, Garcia-Porrua C, et al. Gonzalez-Gay MA. HLA-B35 association with nephritis in Henoch-Schönlein purpura. J Rheumatol. 2002; 29: 948- 949.
- Londono J, Santos AM, Rueda JC, Calvo-Paramo E, Burgos-Vargas R, et al. Association of ERAP2 polymorphisms in Colombian HLA-B27+ or HLA-B15+ patients with SpA and its relationship with clinical presentation: axial or peripheral predominance. RMD Open. 2020; 6: e001250.
- Chang MK, Chang L, Kuo HY, Arango CA. A Rare Complication of Henoch-Schönlein Purpura/IgA Vasculitis in an Adult Woman after COVID-19 Infection. Cureus. 2023; 18(15): 42063.
- Asiri A, Alzahrani F, Alshehri S, Hassan AbdelQadir Y. New-Onset Henoch-Schonlein Purpura after COVID-19 Infection: A Case Report and Review of the Literature. Case Rep Pediatr. 2022; 29: 1712651.
- Dakwar E, Reddy J, Vale FL, Uribe JS. A review of the pathogenesis of ankylosing spondylitis. Neurosurg Focus. 2008; 24: E2.
- R Rejdak, M Rękas. Retinal physiology and psychophysical response. Basic and Clinical Science Course, Section 12, Retina and Vitreou. Wrocław, Edra Urban & Partner. 2020; 47-57.
- O’Halloran HS, Berger JR, Lee WB, Robertson DM, Giovannini JA, et al. Acute multifocal placoid pigment epitheliopathy and central nervous system involvement: Nine new cases and a review of the literature. Ophthalmology. 2001; 108: 861-868.
- Brydak-Godowska J, Gołębiewska J, Turczyńska M, Moneta-Wielgoś J, Samsel A, et al. Observation and Clinical Pattern in Patients with White Dot Syndromes: The Role of Color Photography in Monitoring Ocular Changes in Long-Term Observation. Med Sci Monit. 2017; 2(23): 1106-1115.
- Chan A, Blumenkranz MS, Sanislo SR. An extensive case of acute posterior multifocal placoid pigment epitheliopathy. Retin Cases Brief Rep. 2010; 4: 336-8. doi: 10.1097/ICB.0b013e3181aff47e.
- Wilkos-Kuc A, Biziorek B, Zarnowski T. Ostra tylna wieloogniskowa plackowata epiteliopatia barwnikowa (APMPPE)-opis trzech przypadków. Acute posterior multifocal placoid pigment epitheliopathy (APMPPE)-a report of three cases. Klin Oczna. 2012; 114: 286-91.