
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Ectopic mediastinal parathyroid adenoma in association with metachronous intrathymic choriocarcinoma in an elderly woman: A co-existence never described before
Helen J Trihia1*; Grivas Anastasios2; Antonios Chatzimichalis3
1Department of Pathology, Consultant Pathologist, ‘Metaxas’ Cancer Hospital, Piraeus, Greece.
2Department of Medical Oncology, Consultant Medical Oncologist, Agios Savvas Anticancer Hospital, Athens, Greece.
3Head of Department of Thoracic Surgery, ‘Metaxas’ Cancer Hospital, Piraeus, Greece.
*Corresponding Author : Helen J Trihia
Department of Pathology, Consultant Pathologist, ‘Metaxas’ Cancer Hospital, Piraeus, Greece.
Tel: +30-6970-918556;
Email: eltrix@otenet.gr
Received : Apr 19, 2024
Accepted : May 07, 2024
Published : May 14, 2024
Archived : www.jcimcr.org
Copyright : © Trihia HJ (2024).
Abstract
Primary malignant germ cell tumors of the mediastinum are extremely rare among females. Primary choriocarcinoma of the mediastinum is a rare form of extragonadal germ cell tumor that has a poorer prognosis in comparison to other extragenital germ cell tumors and occurs almost exclusively in young men. Intrathymic parathyroid adenoma is a rare cause of persistent primary hyperparathyroidism. We present a unique-never reported before- case of a postmenopausal woman with a coexistent ectopic parathyroid adenoma and choriocarcinoma of the thymic area in the anterior mediastinum.
Keywords: Ectopic; Parathyroid adenoma; Intrathymic; Choriocarcinoma; Woman.
Citation: Trihia HJ, Anastasios G, Chatzimichalis A. Ectopic mediastinal parathyroid adenoma in association with metachronous intrathymic choriocarcinoma in an elderly woman: A co-existence never described before. J Clin Images Med Case Rep. 2024; 5(5): 3048.
Introduction
The parathyroid glands and the thymus have a close embryologic and anatomic relationship; however reports of co-existent ectopic mediastinal parathyroid and extragonadal germ cell tumor pathology are rare in the literature. We report on a 78-year-old woman with primary hyperparathyroidism secondary to an ectopic parathyroid adenoma in association with a metachronous choriocarcinoma of the anterior mediastinum.
Material and methods
A 76-year old woman, with a history of hypertension, hyperlipidemia, total thyroidectomy and uterus prolapse, was admitted in our hospital for the investigation of blood loss from the large bowel. She was diagnosed with diverticulosis of the large intestine. At the same time, her calcium level was 13.5 mg/dL (normal range: 8.4-10.5 mg/dL), her Parathyroid Hormone (PTH) level 477.8 pg/mL (normal range: 15-65 pg/mL) and the 24-hour-urine calcium 513 mg/24h. Renal stones were found in her right kidney. However, subsequent high resolution CT scan of chest and neck, failed to demonstrate any abnormality. The patient underwent a Technetium-99m-sestamibi SPECT CT (99mTc/99mTc-MIBI) for parathyroid lesion localization. The scan showed a focus of increased MIBI accumulation in the anteriosuperior mediastinum, at the left side of the midline and a lesion of ovoid configuration was identified, measuring 15.6 x 21.2 x 25.6 mm, consistent with ectopic anterior mediastinal parathyroid adenoma. Remarkably, the possibility of thymoma was proposed from the radiologist. The patient refused any surgical intervention and was put on medication with follow up calcium level monitoring.
One year and nine months later the woman entered the hospital with recent acute respiratory distress (shortness of breath) of 10-days duration and pulse sensation during the night hours.
Imaging investigation with chest Computerized Tomographic scan (CT-scan) and Magnetic Resonance Imaging (MRI) showed a bulky anterior mediastinal mass, of 110.3 x 109.2 x 90.8 mm, in the anteriosuperior mediastinum, expanding and encroaching on surrounding structures, including shift of the large veins to the left. Multiple nodular lesions of 1-1.5 cm were found at the periphery of the mass. There was pleural and small pericardial effusion. The mass was in contact with the visceral pleura of the right upper and median pulmonary lobes. There were no pulmonary lesions.
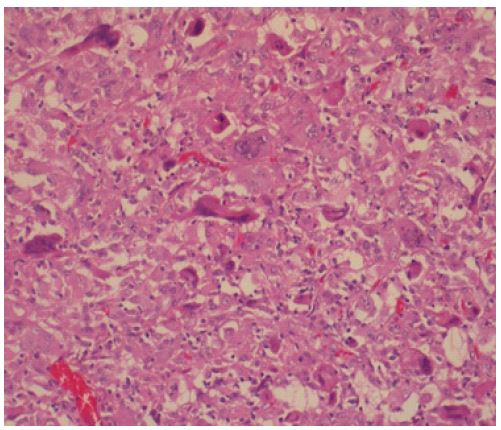
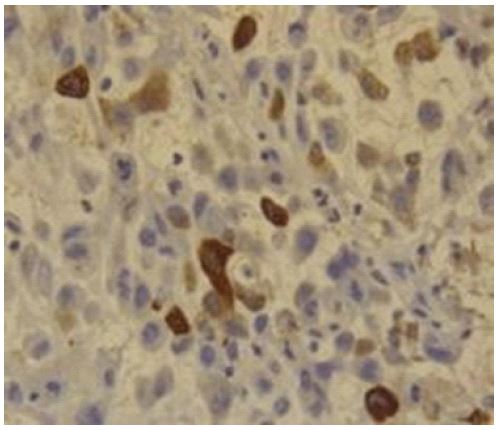
CT-guided Fine Needle Aspiration Biopsy (FNAB) was initially diagnostic of a non-specific high grade sarcoma. In the differential diagnosis were included sarcomatoid thymic carcinoma, monophasic synovial sarcoma and sarcomatoid mesothelioma. The immunohistochemical investigation was positive for VIM, CD99 (membranous), EMA (focally), calponin and negative for KerAE1/AE3, Ker5/6, Ker7, Ker19, TTF1, CD5, LCA, CD34, bcl-2, S-100, SMA, GFAP, calretinin, CD30, MPO, c-kit and galectin-3. Nevertheless, after examination of multiple serial H&E (Hematoxylin and Eosin) sections, rare large multinucleated giant cells, with dark smudged nuclei, and abundant eosinophilic cytoplasm were revealed (Figure 1). Immunohistochemically, the tumor cells were reactive for β-HCG (Figure 2). The admixture of medium-sized cells and multinucleated cells in a hemorrhagic background lead to the diagnosis of choriocarcinoma. The serum β-HCG level (beta-human chorionic gonadotrophin) at the time of diagnosis was 300 mIU/mL (normal: < 5M mIU/mL). Alpha-fetoprotein was not detected in the serum.
The patient refused chemotherapy and an attempt was made for surgical debulking of the tumor. Radical removal of the mass was not possible, because of massive involvement of the adjacent structures (infiltration of neighboring organs-great vessels, lung and chest wall) and hemorrhage. The tumor was dissected via piecemeal approach (Figure 3). The tumor was extensively necrotic and hemorrhagic. The patient died shortly after surgery.
Results
On gross examination, several fragments of a tumor mass were received, the larger of which measuring 10.5 x 10 x 6.5 cm, exhibiting tan-white to yellow appearance, with focal nodularity, necrotic and cystic areas.
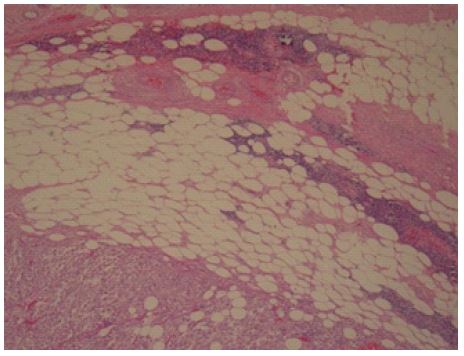
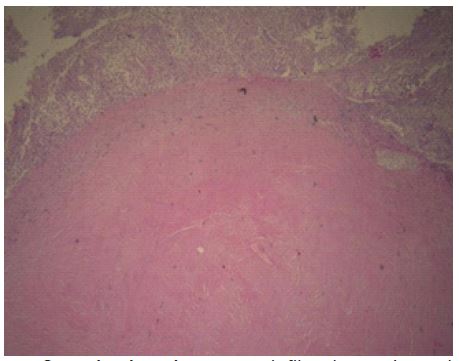
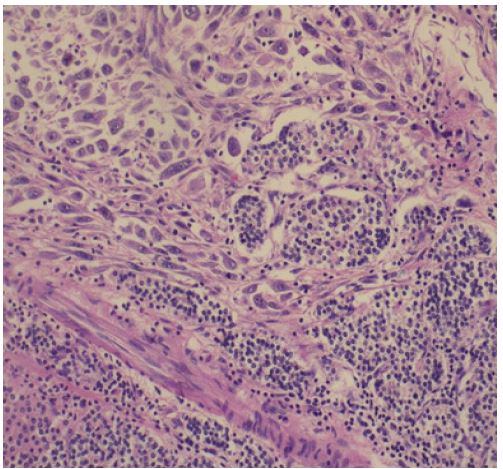
Histologically, the tumor consisted of a high grade, mitotically active, pleomorphic, epithelioid and partly spindle cell malignant tumor, extensively necrotic and hemorrhagic. The neoplastic cells were of medium size with indistinct cell borders or spindle shaped with pleomorphic nuclei and prominent nucleoli. In a few areas there were interspersed multinucleated cells with smudged dark nuclei and abundant eosinophilic cytoplasm. The tumor was infiltrating striated muscle fibres, fatty tissue with remaining islands of thymic tissue in areas (Figure 4) and interspersed psammomatous foci. There were large vessel intravascular emboli. The tumor was infiltrating in continuity the periphery of a circumscribed tumor-like, extensively collagenized fibrosclerotic, partly calcified area, of approximately 2 cm maximum diameter, with small amount of residual areas of a parathyroid tissue/neoplasm in the fibrotic rim, consistent with the known clinical history of ‘ectopic mediastinal, intrathymic parathyroid adenoma’ (Figure 5). Pulmonary parenchyma was evident focally. The two elements were separate-merging to each other- or intermingled in areas (Figure 6).
Selective immunohistochemical investigation, displayed strong staining for VIM, calponin, EMA (focally), β-HCG in the multinucleated giant cells, CD99 (membranous), WT1 and negative expression for KerAE1/AE3, Ker8-18, Ker19, SMA, desmin, S-100, CD5, CD30, CD57, calretinin, a-fet. Also, areas of residual parathyroid neoplasm were positive for PTH, KerAE1/AE3 and chromogranin.
The diagnosis was of a mediastinal intrathymic choriocarcinoma in association with ectopic mediastinal intrathymic parathyroid adenoma.

Discussion
Primary choriocarcinoma of the mediastinum, a form of extragonadal germ cell tumor, is extremely rare, occurs most exclusively in young men and is most often seen in the second and third decades of life [1].
The mediastinum is an area in which a wide range of tissue variability exists. Tumors that can occur in this area therefore can represent many different clinical entities and pathologic processes.
The presence of primary Mediastinal Germ Cell Tumors (M-GCT) has been recognized for almost 100 years [2-5]. The mediastinum is among the compartments of the body most frequently affected by Germ Cell Tumors (GCTs), secondly only to the gonads and ahead of other Extragonadal GCTs (EGGCTs) that affect the retrococcygeal region and central nervous system. Like their gonadal counterparts, mediastinal GCTs have been categorized into pure seminomas, malignant Non-Seminomatous Germ Cell Tumors (NSGCT), including embryonal carcinoma, yolk sac tumor, choriocarcinoma and mixed GCTs, and teratomas [6]. Primary choriocarcinoma of the mediastinum is extremely rare, it is commoner in men and is most often seen in the second and third decades of life [6]. The histogenesis remains obscure. It has been hypothesized that extragonadal germ cell tumors in general are a consequence of aberrant midline migration of primordial germ cells [7]. The preference of GCTs for the mediastinum has been explained by the distribution of fetal primordial germ cell precursors that migrate from the yolk sac to paired midline structures called germinal ridges which during very early development extend virtually throughout the axial dimension of the body during embryonal development. If arrested during migration, some germ cell precursors may survive and serve as cells of origin for subsequent GCT development. However, since thymic epithelial stem cells and their plasticity have only partially been characterized, a somatic stem cell derivation of at least some of mediastinal GCTs has not been excluded to date. The origin of extragenital choriocarcinoma is bound up with the origin of dermoids and teratomas. The origin of mediastinal dermoids and teratomas has been attributed by many to a branchiogenic source; such inclusions have been noted to have connections with the thymus. Hence, a derivation has been postulated from the third branchial pouch and cervical sinus [3].
Choriocarcinoma represents the least common tumor in the mediastinum and it has been reported only rarely in the literature and often as case reports or occasional series [8-12]. Primary non-gestational Mediastinal Choriocarcinoma (MC) is a germ cell malignancy that is diagnosed in the absence of a primary tumor in the gonads or metastatic disease in the retroperitoneal lymph nodes [13].
MC have been described to harbor an isochromosome I (12p) characteristic of postpubertal malignant GCTs [14]. Primary MC most often develops in young men [1]. There are only very occasional case reports of MCs described in women [15], including one recent publication of only one case in an 82-year-old woman, what appears to be the oldest patient reported to date [16]. Our case seems to be the second oldest patient reported in the literature. Elevated HCG levels typically aid in the diagnosis. Non-seminomatous germ cell tumors produce high levels of AFP, β-HCG, or both. Less than 10% of seminomatous tumors produce β-HCG, and those that do produce β-HCG, produce low levels of this marker. MC are morphologically indistinguishable from their gonadal or uterine counterparts. Most tumors are large, soft, friable and extensively hemorrhagic with foci of necrosis. Most cases present with infiltration of neighbouring organs, such as great vessels, lung and chest wall with intra- and extrathoracic metastases.
One additional issue is that often the diagnosis of M-GCT is done with a mediastinoscopic biopsy, and once a diagnosis of GCT is established, it is likely that the patient receives medical treatment before the tumor is surgically removed, thus making histopathological appraisal of the tumor very difficult as often the tumor has become necrotic. This type of practice has made histopathologic classification more difficult, as often the amount of necrosis in a given tumor far exceeds viable tumor. Also, the rarity of primary MC, the small size of tumor samples and the scarcity of syncytiotrophoblasts, make it challenging to diagnose by biopsy alone.
In our case, diagnosis of choriocarcinoma by biopsy was not easy and was not considered initially in the differential diagnosis. It was only after the examination of multiple H&E sections and the finding of rare multinucleate cells, that the true diagnosis came into consideration. After all, the diagnosis of an extragenital mediastinal choriocarcinoma in an elderly woman had not been described before in the literature at the time.
Primary hyperthyroidism usually results from excessive secretion of parathormone (PTH) from the cervical parathyroid glands. About 85% of the Primary Hyperparathyroidism (PHPT) is due to adenoma. In 10% of cases, these adenomas can be ectopic in location. Ectopic parathyroid adenomas can be located in any part of their migratory path [17]. Most common sites of ectopic location of parathyroid adenoma include thymus, tracheo-esophageal groove, carotid sheath, intra-thyroidal, para-esophageal locations, base of the skull. Also from ectopic or supernumerary parathyroid tissue within the pericardium, soft tissue adjacent to the angle of the jaw or the vagus and hypoglossal nerves [18]. The ectopic location is due to the common embryological origin of both the inferior parathyroid gland and thymus from the third pharyngeal pouch, both migrating caudally to their respective locations [19]. Though the inferior parathyroids are usually found adjacent to the inferior pole of the thyroid, they could lie within the suprasternal fossa, thyro-thymic ligament, thymus, or perithymic fat in case of an ectopic gland.
Approximately 10-20% of all parathyroid neoplasms occur in the mediastinum, most commonly in the anteriosuperior mediastinum in the vicinity of or within the thymus gland [20]. Patients usually present with symptoms due to hyperparathyroidism, but some may be found to have hypercalcaemia incidentally, as in our patient. There is often radiological evidence of a mediastinal mass.
Large tumours are ovoid in configuration and sharply separated from the surrounding tissue by a thin fibrous capsule. A rim of normal gland is commonly found. Foci of cystic degeneration and calcification are apparent in many cases. Parathyroid adenomas may exhibit considerable fibrosis, as in our case. Groups of residual adenoma cells are entrapped within the fibrotic wall. In our case, the choriocarcinoma was juxta-opposed to a rounded, circumscribed area of dense fibrosis and calcification, with remaining areas peripherally of parathyroid tissue.
The co-existence of these two elements in the mediastinum, has not been described before in the literature and it gives us a broader base for consideration concerning the histogenesis of these exceedingly rare tumors.
Also important to highlight is the continuous usage of the term mediastinal GCT, which although appropriate, perhaps does not convey that M-GCT are likely to be of thymic origin. Thus, the better nomenclature may be that of Thymic-GCT (T-GCT), just the same as we use it for thymic carcinoma or other tumors in that region.
Conclusion
Diagnosis of EGGCTs should always be considered when a bulky lobulated anterior mediastinal mass is present in a young male. Our case demontrates that the occurrence of a mediastinal mass in an elderly woman, cannot exclude the diagnosis of an extragenital choriocarcinoma-although a curiosity- and also offers the base of thoughts regarding the histogenesis of these tumors.
Declarations
Compliance with ethical standards: Informed consent was obtained from the family of the deceased patient.
Conflict of interest: The authors declare that they have no conflict of interest.
Funding: None.
Authors contribution: HJT: Diagnosis, study conception and design, drafting and writing of the paper, AG: Presurgical medical oncology approach, AC: Surgical approach.
First accepted and presented: At the 32nd Congress of the ESP and XXXIII International Congress of the IAP, 5-9 December 2020, Glasgow, UK, as a digital poster (physical), poster number: PS-27-006 (ESP/IAP Virtual Congress, Dec 2020).
References
- Fine G, Smith RW, Pachter MR. Primary extragenital choriocarcinoma in the male subject, a case report and review of the literature. Amer. J. Med. 1962; 32: 776-794.
- Neda Kalhor, Cesar A. Moran. Primary germ cell tumors of the mediastinum: A review. Mediastinum. 2018; 2: 4.
- MJG Lynch, GL Blewett. Choriocarcinoma arising in the male mediastinum. Thorax. 1953; 8: 157.
- Paul Jernstorm, Henry McLaughlin. Choriocarcinoma of the thymus. JAMA. 1962; 182(2): 147-151.
- S Prusty, JN Bhayana, NC Nayak, et al. Primary Mediastinal Choriocarcinoma Dis Chest. 1969; 56: 543-546.
- Moran CA, Suster S. Primary germ cell tumors of the mediastinum: I. Analysis of 322 cases with special emphasis on teratomatous lesions and a proposal for histopathologic classification and clinical staging. Cancer. 1997; 80: 681-90.
- Willis RA. The borderland of embryology and pathology. Bull N Y Acad Med. 1950; 26: 440-60.
- Sickles FA, Belliveau RF, Wiernik PH. Primary mediastinal choriocarcinoma in the male. Cancer. 1974; 33: 1196-203.
- Greenwood SM, Goodman JR, Schneider G, et al. Choriocarcinoma in a man. Am J Med. 1971; 51: 416-22.
- Hsueh YS, Tsung SH, Shamsai R, et al. Primary mediastinal choriocarcinoma in a man with an abnormal chromosome. South Med J. 1984; 77: 1466-9.
- Kathuria S, Jablokov VR. Primary choriocarcinoma of mediastinum with immunohistochemical study and review of the literature. J Surg Oncol. 1987; 34: 39-42.
- Moran CA, Suster S. Primary mediastinal choriocarcinomas: A clinicopathologic and immunohistochemical study of eight cases. Am J Surg Pathol. 1997; 21: 1007-12.
- Martini N, Golbey RB, Hajdu SI, Whiltmore WF, Beattle FJ. Primary mediastinal germ cell tumours. Cancer. 1974; 33: 763-769.
- Chaganti RS, Rodriguez E, Mathew S. Origin of adult mediastinal germ cell tumours. Lancet. 1994; 343: 1130-2.
- Samantha Batman, Terry Morgan, Marta Brunetti, et al. Primary mediastinal choriocarcinoma in a female patient: Case report and review of the literature. Gynecologic Oncology Reports. 2018; 26: 99-101.
- Shouichi Okamoto, Jun Ito, Hitomi Yoshikawa, et al. A case of primary mediastinal choriocarcinoma in an elderly woman. Japanese Journal of Lung Cancer Case Reports. 2017; 57(4): 299-303.
- Alesina PF, Moka D, Mahlstedt J, et al. Thoracoscopic removal of mediastinal hyperfunctioning parathyroid glands: personal experience and review of the literature. World J Surg. 2008; 32: 224-31.
- Pellitteri PK. Directed parathyroid exploration: Evolution and evaluation of this approach in a single-institution review of 346 patients. Laryngoscope. 2003; 113: 1857-69.
- Noussios G, Anagnostis P, Natsis K. Ectopic parathyroid glands and their anatomical, clinical and surgical implications. Exp Clin Endocrinol Diabetes. 2012; 120: 604-610.
- Clark OH. Mediastinal parathyroid tumors. Arch Surg. 1988; 123: 1096-100.