
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 5
Delirium in older adults with dementia: What is the role of electroencephalogram?
Ori Perelmutter, MD1; Ana Waitzman, MD2; Dan Justo, MD, MHA2*
1Internal Medicine C, Meir Medical Center, Kfar-Saba, Israel, Tel-Aviv University School of Medicine, Israel.
2Geriatrics Division, Sheba Medical Center, Ramat-Gan, Israel, Tel-Aviv University School of Medicine, Israel.
*Corresponding Author : Dan Justo, MD, MHA
Geriatrics Division, Sheba Medical Center, Ramat-Gan, Israel.
Tel: 972-52-6668550, Fax: 972-9-7408575;
Email: dan.justo@sheba.health.gov.il
Received : Apr 22, 2024
Accepted : May 08, 2024
Published : May 15, 2024
Archived : www.jcimcr.org
Copyright : © Justo D (2024).
Abstract
Mental status changes in older adults with dementia are a diagnosis challenge since they might be consistent with two common entities: dementia progression or delirium. Electroencephalogram (EEG) may help clinicians to diagnose delirium in coherent patients but its use in older adults with dementia is controversial due to low specificity. Mental status changes in older adults with dementia might also be consistent with non-convulsive focal seizures which are presumed rare, but there is no data concerning its actual prevalence. We present two older adults with dementia and mental status changes in whom EEG has been performed to rule out delirium, but it has revealed epileptiformic activity. Administration of anti-epileptic agents has been highly effective in both patients. We would like to increase awareness to non-convulsive focal seizures mimicking delirium in older adults with dementia, and to encourage clinicians to use EEG in these patients by suggesting a diagnosis algorithm.
Keywords: Delirium; Electroencephalogram; Older adults; Seizures.
Citation: Perelmutter O, Waitzman A, Justo D. Delirium in older adults with dementia: What is the role of electroencephalogram?. J Clin Images Med Case Rep. 2024; 5(5): 3051
Introduction
Mental status changes in older adults with dementia might be consistent with dementia progression; in Alzheimer’s disease they include apathy, agitation, irritability, delusions, and hallucinations; in vascular dementia they include apathy and delusions; in dementia with Lewy bodies and in dementia associated with Parkinson’s disease they include visual hallucinations and delusions; in frontotemporal dementia and in progressive supranuclear palsy they include apathy and disinhibition [1]. These neuropsychiatric symptoms are a diagnosis challenge since they are also common features of delirium in older adults with dementia [2]. Moreover, prolonged delirium might be consistent with dementia progression [3]. Electroencephalogram (EEG) slowing and reduced functional connectivity may help clinicians diagnose delirium in coherent patients [4], but in older adults with dementia EEG use is controversial since these findings are non-specific [5]. Herein, we present two older adults with dementia and mental status changes in whom EEG has been performed to rule out delirium, but it has revealed a surprising finding: epileptiformic activity. We would like to increase awareness to non-convulsive focal seizures mimicking delirium in older adults with dementia.
Case descriptions
Case 1
An 82-years-old female had two years history of cognitive decline, bradykinesia, rigidity, and visual hallucinations. Accordingly, dementia with Lewy bodies was suspected and Levodopa was administrated. Her medical history also included essential hypertension, urinary incontinence, and chronic legs pain due to degenerative changes causing lumbar spinal stenosis. Her medications additionally included Ramipril, Fesoterodine, Pregabalin, and Buprenorphine. She was admitted due to a three-week history of fluctuating cognitive decline, inattention, and sleepiness. The examination revealed low concentration, time disorientation, and motor dysphasia. Laboratory tests were unremarkable. A head CT scan demonstrated periventricular white matter chronic ischemic changes but no acute ischemic stroke or intracranial bleeding. Pregabalin and Buprenorphine were stopped but there was no improvement. EEG had been performed to rule out delirium, but it revealed an epileptiformic activity in the left temporal lobe. Accordingly, Carbamazepine was started, and cognitive improvement was observed a few days later; the patient was more oriented, more alert, and her speech was more fluent. A second EEG few days later showed general slowing indicating diffuse cortical dysfunction but no epileptiformic activity.
Case 2
A 92-years-old female had several years history of dementia–probably vascular dementia. Her medical history also included transient ischemic attack a few years earlier, diabetes mellitus, essential hypertension, and colectomy due to colon cancer 10 years before. Her medications included Quetiapine, Trazodone, Metformin, and Bisoprolol. She was admitted due to three weeks history of worsening fluctuating cognitive decline, inattention, and hallucinations. Moreover, she did not recognize her son, and three days before admission she fell and hurt her head. The examination revealed low concentration, time and place disorientation, psychomotor agitation, and incoherent speech. Laboratory tests were unremarkable. A head CT scan showed brain atrophy, but no acute ischemic stroke or intracranial bleeding. Before admission Trazodone was stopped, Quetiapine dosage was increased, and Clonazepam was initiated, but there was no improvement. Following admission Quetiapine was stopped and Risperidone was initiated but still there was no improvement. EEG had been performed to rule out delirium, but it revealed an epileptiformic activity in the left temporal lobe. Accordingly, Risperidone was stopped, Levetiracetam was started, and cognitive improvement was observed a few days later; the patient was more oriented, and hallucinations did not return. A second EEG few days later showed general slowing indicating diffuse cortical dysfunction but no epileptiformic activity.
Discussion
By presenting these patients we would like to increase awareness to non-convulsive focal seizures mimicking delirium in older adults with dementia, and to encourage clinicians to use EEG in these patients. Since there is no data concerning the actual prevalence of non-convulsive focal seizures presented as mental status changes in older adults with dementia, they might be more common than presumed.
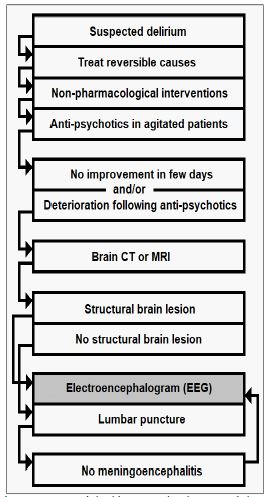
Ruling out epileptiformic activity in this population is clinically crucial since agitation, irritability, delusions, hallucinations, and disinhibition are many times treated with anti-psychotic agents, as with the second above-mentioned patient, which lower the threshold for seizures and actually provoke epilepsy [6] and might worsen mental status changes; it is possible that a paradoxical agitation induced by anti-psychotics [7] is actually the clinical presentation of non-convulsive focal seizures aggravated by anti-psychotics; it is also possible that anti-psychotics increase the risk for sudden death not only by inducing QT interval prolongation and Torsade de Pointes [8], but also by provoking seizures [9]; these theories should be studied prospectively by performing EEG in large cohorts of older adults with dementia and mental status changes, but in the meanwhile we suggest a simple algorithm concerning EEG use in older adults with dementia and suspected delirium (Figure 1). According to this algorithm, EEG should be performed when delirium does not resolve despite adequate treatment and following brain imaging showing a structural brain lesion; in case of no structural brain lesion EEG should also be performed following exclusion of meningoencephalitis.
Conclusion
In conclusion, mental status changes in older adults with dementia which do not resolve despite adequate treatment may warrant EEG not only to rule out delirium but also to rule out non-convulsive focal seizures.
Acknowledgments: None.
References
- McKeith I, Cummings J. Behavioural changes and psychological symptoms in dementia disorders. Lancet Neurol. 2005; 4: 735-742.
- Hölttä E, Laakkonen ML, Laurila JV, Strandberg TE, Tilvis R, Kautiainen H, et al. The overlap of delirium with neuropsychiatric symptoms among patients with dementia. Am J Geriatr Psychiatry. 2011; 19: 1034-1041.
- Fong TG, Davis D, Growdon ME, Albuquerque A, Inouye SK. The interface between delirium and dementia in elderly adults. Lancet Neurol. 2015; 14: 823-832.
- Boord MS, Moezzi B, Davis D, Ross TJ, Coussens S, Psaltis PJ, et al. Investigating how electroencephalogram measures associate with delirium: a systematic review. Clin Neurophysiol. 2021; 132: 246-257.
- Thomas C, Hestermann U, Walther S, Pfueller U, Hack M, Oster P, et al. Prolonged activation EEG differentiates dementia with and without delirium in frail elderly patients. J Neurol Neurosurg Psychiatry. 2008; 79: 119-125.
- Pisani F, Oteri G, Costa C, Di Raimondo G, Di Perri R. Effects of psychotropic drugs on seizure threshold. Drug Saf. 2002; 25: 91-110.
- Fond G, MacGregor A, Ducasse D, Brittner M. Paradoxical severe agitation induced by add-on high-doses quetiapine in schizo-affective disorder. Psychiatry res. 2014; 216: 286-287.
- Glassman AH, Bigger Jr JT. Antipsychotic drugs: prolonged QTc interval, torsade de pointes, and sudden death. Am J Psychiatry. 2001; 158: 1774-1782.
- Ravin DS, Levenson JW. Fatal Cardiac Event following Initiation of Risperidone Therapy. Ann Pharmacother. 1997; 31: 867-870.