
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
An unusual initial presentation of Klebsiella pneumoniae: Spontaneous pneumothorax
Shambhu Khanal1*; Savita Aryal2; Bibek Khanal1; Sushil Neupane1; Buddha Rayamajhi3
1Department of Internal Medicine, Lumbini Provincial Hospital, India.
2Department of Emergency, Lumbini Provincial Hospital, India.
3Department of General Medicine, Tribhuvan University Teaching Hospital, India.
*Corresponding Author : Shambhu Khanal
Department of Internal Medicine, Lumbini Provincial Hospital, India.
Email: Shambhukhanal19@gmail.com
ORCID ID: 0000-0002-1247-7389.
Received : Apr 22, 2024
Accepted : May 08, 2024
Published : May 15, 2024
Archived : www.jcimcr.org
Copyright : © Khanal S (2024).
Abstract
Spontaneous pneumothorax can be a rare presentation of Klebsiella pneumoniae in a healthy nonalcoholic young individual without prior clinical features of pneumonia in developing countries where mycobacterium tuberculosis remains primary suspicion.
Keywords: Klebsiella pneumoniae; Pneumothorax.
Citation: Khanal S, Aryal S, Khanal B, Neupane S, Rayamajhi B. An unusual initial presentation of Klebsiella pneumoniae: Spontaneous pneumothorax. J Clin Images Med Case Rep. 2024; 5(5): 3052.
Case presentation
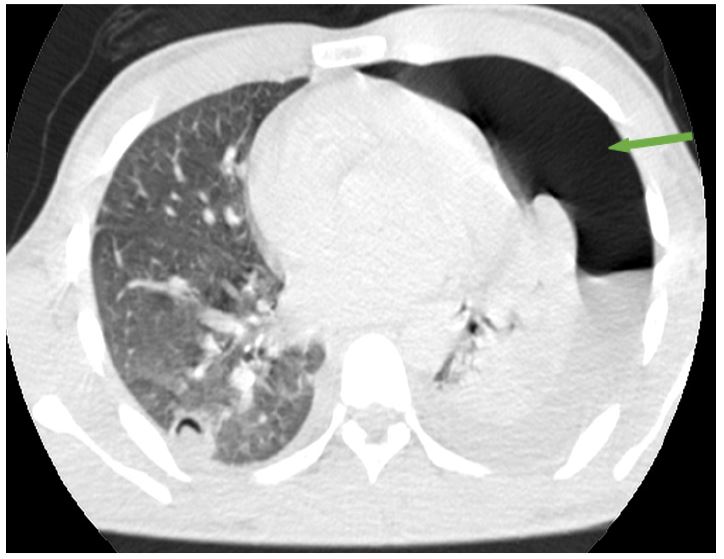
We report a case of 20 year old boy who presented to Department of Emergency with acute onset shortness of breath for 4 hours. He had fever with chills on the same day. There was no history of any past comorbidities, past admissions in hospital, prior clinical symptoms. On examination, his vital signs were stable. On systemic examination, there was decrease in breath sounds on left side of chest. His lab reports showed normal hemogram, liver function and renal function. Sputum examination for genexpert and Ziehl Neelson stain (ZN) did not detect acid fast bacilli. His chest X-ray revealed large left sided pneumothorax. On doing contrast CT chest, there were multiple cavitating nodules with pneumothorax on left side. Sputum gram stain and culture showed gram negative organism and Klebsiella pneumonia in culture sensitive to polymixin and colistin. He was managed with chest tube insertion and intravenous antibiotics.
Discussion
Collection of gas in pleural cavity is pneumothorax. The yearly occurrence rates for primary spontaneous pneumothorax and secondary spontaneous pneumothorax were 37 and 1553 per 100,000 individuals, respectively. Pulmonary Tuberculosis (TB) has emerged as the predominant reason for Secondary Spontaneous Pneumothorax (SSP) and hydropneumothorax especially in endemic areas. Chronic Obstructive Pulmonary Disease (COPD) and pneumonia are the subsequent leading causes of SSP. Acute dyspnea and chest pain are common presenting features in pneumothorax [1]. Klebsiella pneumonia presenting as pneumothorax is a rare dramatic clinical presentation. It most commonly affects right middle lobe. However, our case is a young male without prior clinical risk factors and has left lung affected [2]. Spontaneous pneumothorax in young males can have underlying bacterial pneumonia apart from tuberculosis and primary spontaneous pneumothorax despite short duration of clinical symptoms as seen in our case. Occasionally, concomitant mycobacterium tuberculosis, klebsiella and pseudomonas may be found in cases presenting as pneumothorax. Consideration of bacterial organisms other than tuberculosis is reasonable [3].
Declarations
Acknowledgements: We would like to thank everyone involved during treatment.
Conflict of interest: No conflict of interest.
Contributions: All authors contributed to the preparation of manuscript. SK and SA prepared the main manuscript text. BK, SN and BR collected the materials and prepared Figures. BR guided for whole manuscript and revised it. All authors reviewed the manuscript.
Ethical approval: The consent from the patient deemed to be enough.
Consent: Written informed consent taken from the patient.
References
- Gayatridevi Y, Usharani N, Premkumar A, Sambasivarao G, Kumari VS, Joshua S. Clinical Profile of Spontaneous Pneumothorax in Adults: A Retrospective Study. Indian J Chest Dis Allied Sci. 2015; 57(4): 219-23.
- Kim SJ, Ahn DI, Kim SK, Hong SR, Rhu NS, Cho DI, et al. Clinical Observation of Klebsiella Pneumonia in Adults. Tuberc Respir Dis [Internet]. 1986; 33(1): 55-61. Available from: https://www.e-trd.org/journal/view.php?number=4115.
- Secondary Spontaneous Pneumothorax Secondary to Tuberculosis with Klebsiella and Pseudomonas Co-Infection: A Case Report. Respirology [Internet]. 2019; 24(S2): 27-8. Available from: https://onlinelibrary.wiley.com/doi/abs/10.1111/resp.13699_80.