
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Ovarian cancer with umbilical metastasis: A case report and literature review
Rui Liu1; Shuang Luo1; Xi Yang3; Guowu Wang1; Meijun Liu1; Guohua Huang1; Baiyu Lu1*
1Department of Gynecology, Suining Central Hospital, Suining, Sichuan, China.
2School of Medical and Life Sciences, Chengdu University of Traditional Chinese Medicine, China.
3Suining First People’s Hospital, China.s3Suining First People’s Hospital, China.
*Corresponding Author : Baiyu Lu
Department of Gynecology, Suining Central Hospital, Suining, Sichuan, China.
Email: 29844240@qq.com
Received : Apr 22, 2024
Accepted : May 09, 2024
Published : May 16, 2024
Archived : www.jcimcr.org
Copyright : © Lu B (2024).
Abstract
Ovarian cancer with umbilical metastasis is an extremely rare clinical condition. It presents with subtle symptoms and lacks specific clinical manifestations. Early detection and standardized comprehensive treatment can effectively improve patient prognosis. We report a case of ovarian cancer with umbilical metastasis, presenting with redness, swelling, and tenderness in the umbilical region. CT scan revealed enhanced nodules in the umbilical area and soft tissue nodules in the right pararectal space. A biopsy of the umbilical nodule suggested a possibility of malignancy originating from the reproductive system. Pelvic MRI showed uneven enhancement in the bilateral adnexal region. The final diagnosis was confirmed as ovarian cancer with umbilical metastasis through surgical pathology. The patient underwent a comprehensive treatment approach involving surgery, chemotherapy, and targeted therapy, leading to a progression-free survival until now.
Keywords: Ovarian malignant tumor; Pelvic and abdominal malignant tumor; Umbilical metastasis.
Citation: Liu R, Luo S, Yang X, Wang G, Lu B, et al. Ovarian cancer with umbilical metastasis: A case report and literature review. J Clin Images Med Case Rep. 2024; 5(5): 3054.
Introduction
The common routes of metastasis in ovarian cancer include direct extension, intraperitoneal implantation, and lymphatic spread [1]. The most common distant metastatic sites are the pleura, liver, and lungs [2]. The probability of skin metastasis in ovarian cancer ranges from 0.9% to 5.8% [2,3-5]. In this case, the patient presented with redness, swelling, and tenderness in the umbilical region, and was finally diagnosed with umbilical metastasis from high-grade serous ovarian cancer, which is extremely rare. Skin metastasis is a manifestation of advanced ovarian cancer. Late-stage ovarian cancer has a poor prognosis, with a 5-year overall survival rate of 31% based on data from the SEER database. The patient in this case received a comprehensive management approach involving surgery, chemotherapy, and maintenance therapy, and has been followed up for 39 months postoperatively without any signs of tumor recurrence, indicating a good prognosis.
Case presentation
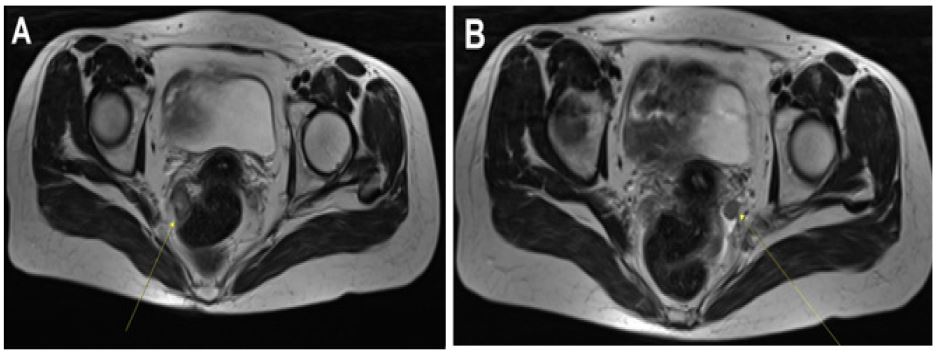
A 50-year-old woman experienced natural menopause at the age of 48, with a history of 5 pregnancies and 1 childbirth. In December 2020, the patient presented with a recurring, painful, and swollen nodule in the umbilical region measuring approximately 0.5 cm in diameter. Ultrasound suggested an inflammatory nodule, while fine-needle aspiration cytology of the umbilical mass revealed clusters of atypical cells. CT scan findings included a mild, homogeneous enhancement of the umbilical soft tissue nodule, with an unclear nature, and a soft tissue nodule in the right pararectal space. Subsequently, a surgical excision of the umbilical mass was performed, and immunophenotyping indicated a possible origin from the female reproductive system. Tumor markers were assessed with CA12-5 at 198.9 U/mL, CA19-9 at 14.01 U/mL, premenopausal Roman index at 14.22%, and postmenopausal Roman index at 52.45%. HE4, AFP, and CEA were within normal range. Pelvic MRI in January 2021 revealed slightly low-signal nodules in both adnexal regions on T1WI and T2WI, with a larger nodule measuring approximately 2.1 cm x 1.4 cm in the right adnexal region, showing significant heterogeneous enhancement and restricted diffusion (Figure 1). Electronic colonoscopy showed a local elevation in the rectum, approximately 2.0 cm in diameter, with a smooth surface and no apparent abnormalities in the mucosa. The patient denied any history of gastrointestinal malignancies, breast cancer, or ovarian cancer in the family. As the patient had previously undergone abdominal nodule resection at another hospital, and at the time of presentation to our hospital, the umbilical region was in a postoperative state. Gynecological examination revealed no abnormalities in the external genitalia, vagina, uterus, or bilateral adnexal regions.
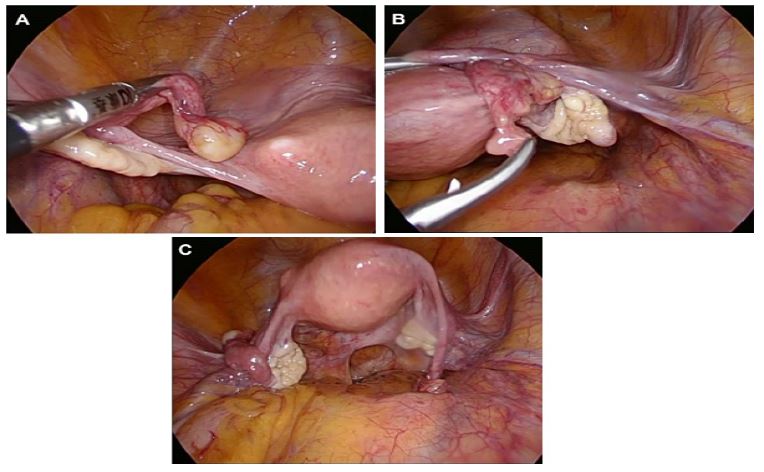
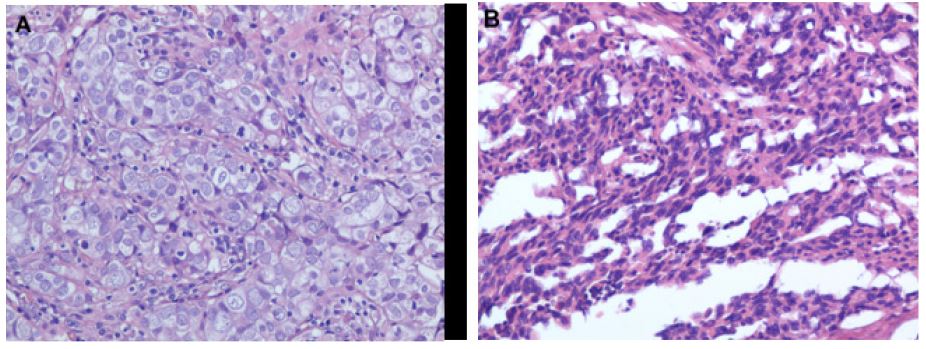
In January 2021, the patient underwent laparoscopic exploration. Intraoperatively, a yellowish, well-defined mass measuring approximately 1.5 cm x 1 cm was observed at the fimbrial end of the left fallopian tube, with no apparent abnormalities in the left ovary. Scattered granular nodules were observed on the surface of the right fallopian tube, with no apparent abnormalities in the right ovary. A poorly defined mass measuring approximately 2.5 cm x 2.0 cm was found adjacent to the rectum on the right side, with clear demarcation from the rectum (Figure 2). Intraoperative excision of bilateral adnexa and right pararectal mass were sent for cryopathological examination. Frozen result indicated poorly differentiated carcinoma in the bilateral adnexa and right pararectal mass, with the specific type to be determined by paraffin section. Based on the preoperative immunohistochemical results, the likelihood of ovarian malignancy was high. Therefore, total hysterectomy, bilateral adnexa, resection of the right pararectal mass, pelvic lymph node dissection, para-aortic lymph node dissection, appendectomy, and omentectomy were performed. Postoperative pathology confirmed high-grade serous adenocarcinoma in both adnexa, and low-differentiated adenocarcinoma of ovarian origin in the right pararectal mass. Immunohistochemistry showed positive staining for PCK, CA12-5, CK7 (partially positive), Pax8, WT-1, and Ki-67 (approximately 60% positive), and negative staining for SATB2 and P53. Lymph node metastasis was detected in 1 out of 4 para-aortic lymph nodes (Figure 3).
The patient received 6 cycles of paclitaxel and cisplatin chemotherapy postoperatively. Due to a negative BRCA gene test result, the patient was treated with Niraparib as targeted maintenance therapy. As of the latest follow-up, there have been no signs of tumor recurrence.
Discussion
Ovarian cancer is the second most common gynecologic malignancy in developed countries and the third most common in developing countries [6]. According to the China Cancer Report 2022, there are about 57,000 new cases of ovarian cancer each year in China. It is often diagnosed at an advanced stage due to its insidious onset and the challenges in early detection, leading to poor treatment outcomes and prognosis with a high mortality rate. Ovarian cancer primarily spreads through direct extension to the contralateral ovary and uterus, and through intraperitoneal dissemination to the peritoneum. Distant metastases are less common and typically involve the liver, lungs, and pleura [2]. Skin metastasis is rare in ovarian cancer [3,5], with umbilical metastasis being even rarer.
Tumors that form nodules in the umbilicus as a result of pelvic and abdominal malignancies are referred to as Sister Mary Joseph’s nodules (SMJN), named in honor of Sister Mary Joseph, who first noticed them [7]. The incidence of SMJN is estimated to be around 1%-3% [8].
The exact mechanisms of SMJN formation are not fully understood. Research suggests that most SMJN patients have peritoneal metastasis, indicating direct invasion of the peritoneal lesions as the most common mechanism of SMJN formation [1]. However, in this case, the patient did not have peritoneal metastasis but showed lymph node metastasis. The umbilicus is surrounded by abundant blood vessels and lymphatics, and its fascial structure is not complete, suggesting that tumor cells may spread to the umbilicus through lymph node metastasis or direct invasion.
SMJN nodules typically do not exceed 5 cm, with some cases reaching up to 10 cm [9]. The average size of SMJN nodules reported by Barrow was between 1 cm and 1.5 cm [10]. Typical SMJN nodules are firm, irregular masses that are usually white, bluish-purple, or red in color. They may be accompanied by pain, itching, ulceration, and can produce bloody, mucous, serous, or purulent secretions. However, some patients may be asymptomatic [10]. SMJN nodules are easily overlooked or misdiagnosed during physical examinations. Previous reports have shown that 57% of umbilical nodules are benign, but almost all malignant lesions are secondary tumors [11]. Considering this case, when encountering a patient presenting with a nodule in the umbilicus, in addition to considering inflammatory diseases, the possibility of SMJN should also be considered, particularly in female patients, with a special focus on tumors originating from the ovaries.
In this case, ultrasound was not highly valuable for diagnosing SMJN, while CT or MRI scans aided in making preliminary assessments regarding the nature and origin of the nodules. For patients with a strong suspicion of SMJN based on imaging findings, pathological diagnosis should be pursued. Fine-needle aspiration cytology is a safe, rapid, minimally invasive, and cost-effective method. However, in this case, the fine-needle aspiration cytology did not provide a definitive diagnosis, likely due to the small sample size and high demand for expertise by pathologists. This makes it difficult to determine the source of the tumour. Given the superficial location of the umbilicus, we recommend local excision of the nodule for pathological examination to avoid misdiagnosis.
SMJN most commonly originates from gastrointestinal tumors, accounting for approximately 35%-65% of cases, followed by tumors of the urogenital system, accounting for approximately 12%-35% [12], and 15%-30% of cases have an unknown primary tumor [13]. The primary tumor location of SMJN is gender-dependent, with gastric and gastrointestinal origins more common in males and reproductive system origins, especially from the ovaries, more common in females [14,15]. Adenocarcinoma is the most common histological type of SMJN, accounting for approximately 75% of cases [16], followed by squamous cell carcinoma, sarcoma, melanoma, and lymphoma [17,18]. Different treatment principles and surgical approaches are required for tumors originating from different systems. Therefore, it is particularly important to accurately determine the primary tumor source through pathological examination of the umbilical nodule. Serous adenocarcinoma accounts for approximately 75%-80% of ovarian epithelial cancers, and immunohistochemistry typically shows positive staining for CK7, PAX8, and WT1, negative staining for CK20 [19]. In high-grade serous adenocarcinoma of the ovary, P53 is often mutated, whereas in low-grade serous adenocarcinomas, P53 is usually wild-type. In the present case of a female SMJN patient, after umbilical node pathology suggestive of a reproductive origin, the patient was referred to an experienced gynaecologist, who improved specialist investigations and implemented standardized specialist treatment, resulting in a good prognosis for the patient. Early and accurate identification of the primary tumor source in SMJN is crucial.
Skin metastasis is often a manifestation of advanced malignancy. Previous studies have shown that the median survival period for patients with skin metastasis from ovarian cancer is 12 months [20,21]. However, a study by Otsuka et al. showed that patients with SMJN originating from ovarian or fallopian tube cancer had longer survival periods when they underwent tumor cell eradication surgery, including SMJN excision surgery, combined with platinum-based adjuvant chemotherapy [1,3]. As for targeted therapy for ovarian epithelial cancer, PARP inhibitors and anti-angiogenic agents (such as bevacizumab) are the main options. Research indicates that the use of anti-angiogenic agents may alter the recurrence pattern and increase the incidence of brain and skin metastases in ovarian cancer [22,23]. In the case of this patient, after surgery and chemotherapy, we administered maintenance therapy with a PARP inhibitor, without the use of bevacizumab. As of the latest follow-up, 39 months after surgery, there have been no signs of tumor recurrence.
Conclusion
Umbilical metastasis from ovarian cancer is extremely rare. When encountering a patient with an umbilical mass, SMJN should be considered in addition to inflammatory diseases. For female patients, particular attention should be paid to the possibility of tumors originating from the ovaries, aiming for early detection and treatment. For patients with a high suspicion of SMJN, local excision of the nodule for pathological examination can help establish a definitive diagnosis. For SMJN originating from the ovaries or fallopian tubes, a comprehensive management approach involving surgery, chemotherapy, and targeted therapy is recommended to improve patient prognosis.
References
- Otsuka I. Cutaneous Metastases in Ovarian Cancer. Cancers (Basel). 2019; 11(9): 1292. Published 2019 Sep 2.
- Dauplat J, Hacker NF, Nieberg RK, et al. Distant metastases in epithelial ovarian carcinoma. Cancer. 1987; 60(7): 1561-1566.
- Otsuka I, Matsuura T. Skin metastases in epithelial ovarian and fallopian tube carcinoma. Medicine (Baltimore). 2017; 96(33): 7798.
- Cormio G, Capotorto M, Di Vagno G, et al. Skin metastases in ovarian carcinoma: a report of nine cases and a review of the literature. Gynecol Oncol. 2003; 90(3): 682-685.
- Cheng B, Lu W, Xiaoyun W, et al. Extra-abdominal metastases from epithelial ovarian carcinoma: an analysis of 20 cases. Int J Gynecol Cancer. 2009; 19(4): 611-614.
- Torre LA, Bray F, Siegel RL, et al. Global cancer statistics, 2012. CA Cancer J Clin. 2015; 65(2): 87-108.
- Nie X, Chen X, Jiang Y, et al. Sister Mary Joseph nodule as cutaneous manifestations of metastatic ovarian cancer: A case report and review of the literature. Medicine (Baltimore). 2022; 101(6): 28712.
- Piura B, Meirovitz M, Bayme M, et al. Sister Mary Joseph’s nodule originating from endometrial carcinoma incidentally detected during surgery for an umbilical hernia: a case report. Arch Gynecol Obstet. 2006; 274(6): 385-388.
- Gracia-Darder I, Del Pozo Hernando LJ. Sister Mary Joseph’s Nodule. J Cutan Med Surg. 2022; 26(2): 221.
- Barrow MV. Metastatic tumors of the umbilicus. J Chronic Dis. 1966; 19(10): 1113-1117.
- Segovis CM, Dyer RB. The “Sister Mary Joseph Nodule”. Abdom Radiol (NY). 2017; 42(5): 1610-1611.
- Gabriele R, Conte M, Egidi F, et al. Umbilical metastases: current viewpoint. World J Surg Oncol. 2005; 3(1): 13. Published 2005 Feb 21.
- Gabriele R, Borghese M, Conte M, et al. Sister Mary Joseph’s nodule as a first sign of cancer of the cecum: report of a case. Dis Colon Rectum. 2004; 47(1): 115-117.
- Palaniappan M, Jose WM, Mehta A, et al. Umbilical metastasis: a case series of four Sister Joseph nodules from four different visceral malignancies. Curr Oncol. 2010; 17(6): 78-81.
- Li Y, Guo P, Wang B, et al. Sister Mary Joseph’s nodule in endometrial carcinoma: A case report. World J Clin Cases. 2019; 7(20): 3358-3363.
- Poparic S, Prohic A, Kuskunovic-Vlahovljak S, et al. Sister Mary Joseph Nodule in an Ovary Adenocarcinoma. Med Arch. 2017; 71(2): 154-157.
- Panaro F, Andorno E, Di Domenico S, et al. Sister Joseph’s nodule in a liver transplant recipient: Case report and mini-review of literature. World J Surg Oncol. 2005; 3(1): 4. Published 2005 Jan 14.
- Tam C, Turner H, Hicks RJ, et al. Diffuse large B-cell non-Hodgkin’s lymphoma presenting as Sister Joseph’s nodule. Leuk Lymphoma. 2002; 43(10): 2055-2057.
- Kossaï M, Leary A, Scoazec JY, et al. Ovarian Cancer: A Heterogeneous Disease. Pathobiology. 2018; 85(1-2): 41-49.
- Dauplat J, Hacker NF, Nieberg RK, et al. Distant metastases in epithelial ovarian carcinoma. Cancer. 1987; 60(7): 1561-1566.
- Majmudar B, Wiskind AK, Croft BN, et al. The Sister (Mary) Joseph nodule: its significance in gynecology. Gynecol Oncol. 1991; 40(2): 152-159.
- Pàez-Ribes M, Allen E, Hudock J, et al. Antiangiogenic therapy elicits malignant progression of tumors to increased local invasion and distant metastasis. Cancer Cell. 2009; 15(3): 220-231.
- Robinson WR, Beyer J, Griffin S, et al. Extraperitoneal metastases from recurrent ovarian cancer. Int J Gynecol Cancer. 2012; 22(1): 43-46.