
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Spectral computed tomography (SCT) for the characterization of cardiac masses: Is magnetic resonance imaging domain over?
Franceschi P; Russo V*; Lovato L
Pediatric and Adult CardioThoracic and Vascular, Oncohematologic and Emergency Radiology Unit, IRCCS University Hospital of Bologna, Via Massarenti 9, 40138, Bologna, BO, Italy.
*Corresponding Author : Russo V
Pediatric and Adult CardioThoracic and Vascular, Oncohematologic and Emergency Radiology Unit, IRCCS University Hospital of Bologna, Via Massarenti 9, 40138, Bologna, BO, Italy.
Email: vincenzo.russo@aosp.bo.it
Received : Apr 22, 2024
Accepted : May 09, 2024
Published : May 16, 2024
Archived : www.jcimcr.org
Copyright : © Russo V (2024).
Abstract
We present a case of a patient in his seventies who experienced recurrent pericardial effusion and exertional dyspnea, initially attributed to an episode of pericarditis. Further investigation revealed marked and diffuse thickening of the right atrial walls, raising suspicion of cardiac mass. Spectral CT (SCT) coronary angiography with delayed phase, cardiac magnetic resonance, 18FDG-PET (Positron Emission Tomography) and histopathological analyses were performed. The findings were consistent with atrial pseudotumor from Erdheim-Chester disease (ECD), a rare non-Langerhans cell histiocytosis. This case highlights the added value of SCT and spectral reconstructions in characterizing cardiac masses and the importance of integrating SCT into diagnostic and therapeutic pathways.
Keywords: Spectral CT imaging; Material decomposition; Z effective; Cardiac mass; Erdheim chester disease; Magnetic resonance.
Abbreviations: CMR: Cardiac Magnetic Resonance; CT: Computed Tomography; SCT: Spectral CT; ECD: Erdheim Chester Disease; ECV: Extra-Cellular Volume; FS: Fat Saturation; LGE: Late Gadolinium Enhancement; LIE: Late Iodine Enhancement; PET: Positron Emission Tomography; SUVmax: Standardized Uptake Value Maximum.
Citation: Franceschi P, Russo V, Lovato L. Spectral computed tomography (SCT) for the characterization of cardiac masses: Is magnetic resonance imaging domain over?. J Clin Images Med Case Rep. 2024; 5(5): 3055.
Introduction
The use of dual energy and Spectral Computed Tomography (SCT) imaging for lesion characterization has been extensively reported in the literature, particularly for extracardiac regions [1]. Thanks to material decomposition reconstructions SCT provides valuable information about lesions’ vascularity through “Iodine-no-Water” and “Iodine Map” images applied to the early-phase acquisition [2]. When these reconstructions are applied to the late-phase acquisitions, they reveal Late Iodine Enhancement (LIE) within the tissues, indicating expansion of the extracellular volume due to cellular or interstitial damage, fibrosis, edema, or deposition of foreign extracellular materials [3]. “Z effective” (effective atomic number) images allow tissue characterization based on effective atomic number [4]. This case report emphasizes the utility of “dual-layer” SCT with spectral analysis for characterizing cardiac masses by comparing them with Cardiac Magnetic Resonance (CMR), currently considered the reference standard. Integrating SCT into diagnostic and therapeutic pathways can complement CMR, assisting in determining the most appropriate approach for individual patients and optimizing diagnostic and therapeutic strategies tailored to their specific needs.
Case report
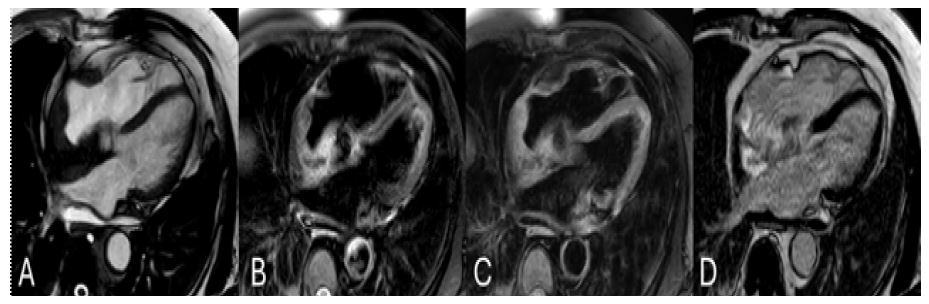
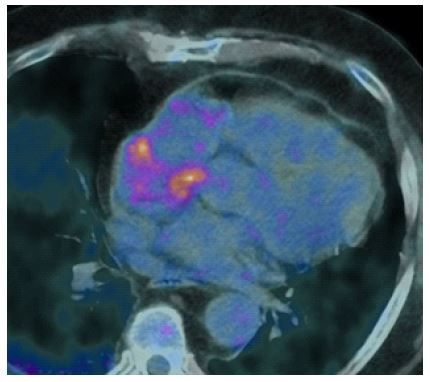
We present the case of a patient in his seventies admitted to our center due to recurrent pericardial effusion associated with exertional dyspnea, previously attributed to an episode of pericarditis and treated with medical therapy. Past medical history includes systemic arterial hypertension, obesity (BMI 30 kg/m2), and former smoking habit. Transthoracic echocardiogram highlighted mild pericardial effusion and poor visualization of the right atrial walls with a doubtful image suggestive of either thickening of the right atrial walls or signs of organization of pericardial effusion. Normal biventricular size and function, with minimal mitral regurgitation were noted (Figure 1). An ECG-gated contrast-enhanced coronary Computed Tomography (CT) angiography with late-phase acquisition for Late Iodine Enhancement (LIE) was performed using a spectral dual-layer CT scanner (SCT). The scan revealed marked and diffuse thickening of the right atrial walls, (maximum thickness 3 cm) extending to the orifices of both the superior and inferior venae cavae. Solid tissue of inhomogeneous density, due to core adipose components, was observed, demonstrating moderate contrast enhancement (Figure 2, Panel A). The spectral analysis revealed that the solid lesion appeared hypodense on “Iodine Map” and “Iodine-no-Water” images due to poor vascularity (Figure 2, Panel B,C), with a lower atomic number compared to the left and right ventricular myocardium (Z-Effective 5-8 vs 8-11) (Figure 2, Panel D), attributable to the presence of core adipose components. Delayed phase acquisition revealed minimal LIE with consistently hypodense core areas and reduced Extracellular Volume (ECV) in the thickest portions (ECV 13-15% vs myocardial normal values 25-30%) (Figure 2, Panel E,F). Findings raised suspicion of heteroformative lesion (lymphoma, angiosarcoma), inflammatory pseudotumor from Erdheim-Chester disease, or IgG4-related disease. Contrast-enhanced CMR performed on a 1.5 T scanner (Figure 3) confirmed marked solid thickening of the right atrial walls isointense to myocardium on T1w images with core areas of hyperintensity due to adipose components, and weakly hyperintense on T2w images. Heterogeneous contrast enhancement on fat-saturated (FS) T1w early and late phase images was noted. The appearance of the lesion at CMR was less suggestive of angiosarcoma, but maintained other diagnostic suspicions. 18FDG-PET (Positron Emission Tomography) scan (Figure 4) demonstrated heterogeneous tracer uptake within the atrial mass (SUVmax=7.4). No significant uptake was observed in the pericardial layers, nor in other investigated body areas. Subxiphoid pericardiocentesis was performed. Chemical, physical, and culture examinations of the aspirated serous fluid were negative. Cytological examination revealed presence of scantily cellular amorphous serous material, granulocytes, lymphocytes, histiocytes, and scattered normal/reactive mesothelial cells. No evidence of neoplastic cells was found. Tumor markers were negative. To further characterize the lesion, a myocardial biopsy via right femoral venous approach showed right atrial myocardium with areas of fibrosis, inflammatory infiltrate with partly foamy histiocytes. BRAF mutation testing was negative for V600E. Histopathological, clinical, and radiological findings were consistent with a diagnosis of atrial pseudotumor from Erdheim-Chester disease.

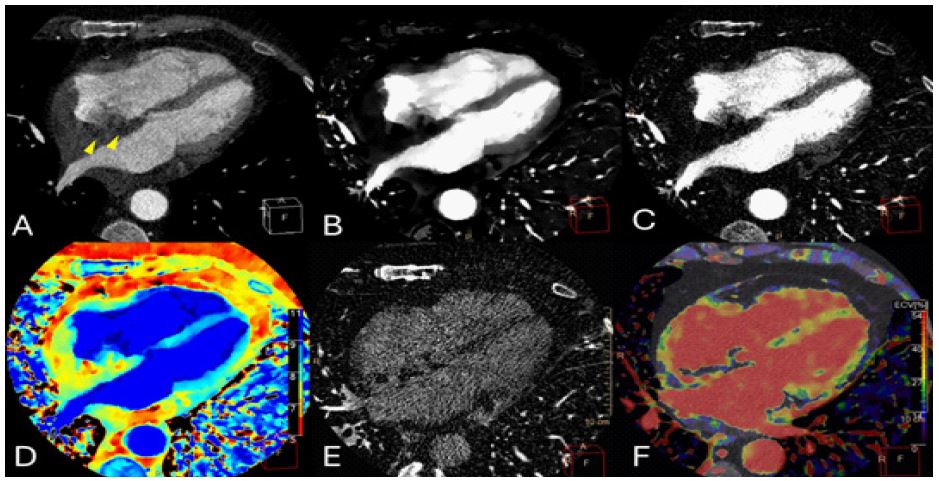
Panel A: Conventional image in arterial angiographic phase shows marked and diffuse thickening of the right atrial walls due to the presence of solid tissue of inhomogeneous density, with core adipose components (yellow arrowheads).
Panel B and C: density map (B) and Iodine no water (C) images of arterial angiographic phase: the solid thickening of the atrial wall is hypodense relating to its poor arterial vascularity.
Panel D: Z effective map of arterial angiographic phase: the solid thickening of the atrial wall has a lower atomic number compared to the left and right ventricular myocardium (Z-Effective number 5-8 vs 8-11), due to the core adipose components.
Panel E: Iodine no water image of delayed phase shows minimal Late Iodine Enhancement (LIE) with consistently hypodense core areas in relation to adipose components.
Panel F: Iodine density map of delayed phase superimposed to virtual non contrast image shows inhomogeneous appearance of the atrial lesion due to the presence of areas with reduced extra-cellular volume (ECV 13-15% vs myocardial normal values 25-30%).
Discussion
Erdheim-Chester Disease (ECD) is a rare non-Langerhans cell histiocytosis affecting multiple organ systems. The disease is characterized by xanthogranulomatous infiltration involving numerous foamy, non-Langerhans cell, lipid-laden histiocytes, which typically express CD68 and are negative for CD1a. Although cardiovascular involvement is common in ECD, it is often asymptomatic and incidentally detected by CT or CMR. One of the hallmark cardiovascular manifestations of ECD is the presence of mural pseudo-tumoral infiltration of the right atrium [5]. This clinical case underscores the added value of SCT and material decomposition reconstructions in characterizing these types of lesions and, more generally, all cardiac masses. SCT coronary angiography with delayed phase, in addition to conventional anatomical information, allows for the evaluation of various parameters. Specifically, reconstructions such as “Iodine-no-Water” and “Iodine Map” applied to the early-phase acquisition allow for assessment of the lesion’s vascularity [2], which in our specific case was poor. When these reconstructions are applied to the late-phase acquisition, they reveal Late Iodine Enhancement (LIE) within the tissues, indicating expansion of the extracellular volume (reflecting myocellular and/or interstitial damage, fibrosis, edema, and deposition of foreign extracellular materials) [3]. In our patient these reconstructions revealed heterogeneous LIE due to the presence of consistently hypodense core areas with reduced Eextracellular Volume (ECV 13-15% vs normal myocardium values of 25-30%) in relation to adipose components. Z effective images allow tissue characterization based on effective atomic number [4]. Core adipose components of the atrial lesion exhibited a lower atomic number compared to the left and right ventricular myocardium (Z-Effective 5-8 vs 8-11). These CT findings were corroborated by CMR, which demonstrated differing signal characteristics of the dual tissue components comprising the lesion, notably the fibro-inflammatory component being isointense on T1w images and heterogeneously hyperintense on T2w images, while the adipose component was hyperintense on T1w images, hypointense on FS T1w images, and hyperintense on T2w images. Heterogeneous contrast enhancement was confirmed on contrast enhanced FS T1w images, reflecting the lesion’s poor vascularity. LGE on delayed-phase T1w images, overlapping with the LIE seen on SCT, was attributed to the fibro-inflammatory component of the lesion. These findings were consistent with the final diagnosis of atrial pseudotumor from ECD [6,7]. Imaging findings and tissue characterization obtained through both SCT and CMR narrow down diagnostic possibilities and guide further diagnostic steps. The increased tracer uptake within the atrial pseudotumor demonstrated by 18FDG PET with SUVmax=7.4 indicated a lesion with heightened metabolism but did not definitely discern its inflammatory or neoplastic nature [8,9]. The absence of significant uptake in the pericardial layers ruled out the pericarditis hypothesis. Moreover, the absence of radiotracer uptake in other investigated body areas indicated the exclusive localization of the disease within the cardiac region, a rare finding for ECD [7,10]. The absence of neoplastic cells and the presence of fibrosis and mixed inflammatory infiltrate, including foamy histiocytes, highlighted by cytological and histopathological analyses, supported the diagnosis of Erdheim-Chester disease.
Conclusion
In conclusion, our case emphasizes the utility of SCT and spectral analysis for characterization of cardiac masses. If appropriately validated, DECT integration into diagnostic pathways can overcome some limitations associated with CMR, such as availability, duration of examinations, metal artifacts, claustrophobia and complement it. The availability and utilization of both techniques can help identify the most suitable approach for each patient, aiming to structure effective diagnostic and therapeutic management tailored to individual needs.
Acknowledgements: Not applicable.
References
- Foti G, Ascenti G, Agostini A, Longo C, Lombardo F, Inno A, et al. Dual-Energy CT in Oncologic Imaging. Tomography. 23 febbraio. 2024; 10(3): 299-319.
- Böttcher B, Zsarnoczay E, Varga-Szemes A, Schoepf UJ, Meinel FG, van Assen M, et al. Dual-Energy Computed Tomography in Cardiac Imaging. Radiol Clin North Am. 1 novembre. 2023; 61(6): 995-1009.
- Oda S, Emoto T, Nakaura T, Kidoh M, Utsunomiya D, Funama Y, et al. Myocardial Late Iodine Enhancement and Extracellular Volume Quantification with Dual-Layer Spectral Detector Dual-Energy Cardiac CT. Radiol Cardiothorac Imaging. Aprile. 2019; 1(1): 180003.
- Rajiah P, Abbara S, Halliburton SS. Spectral detector CT for cardiovascular applications. Diagn Interv Radiol. Maggio. 2017; 23(3): 187-93.
- Diamond EL, Dagna L, Hyman DM, Cavalli G, Janku F, Estrada-Veras J, et al. Consensus guidelines for the diagnosis and clinical management of Erdheim-Chester disease. Blood. 24 luglio. 2014; 124(4): 483-92.
- Merli E, Savelli F, Lovato L, Zompatori M. Cardiac involvement in Erdheim-Chester disease: echocardiographic appearance and value of cardiac MRI. Eur Heart J Cardiovasc Imaging. Febbraio. 2012; 13(2): 198.
- Gianfreda D, Palumbo AA, Rossi E, Buttarelli L, Manari G, Martini C, et al. Cardiac involvement in Erdheim-Chester disease: an MRI study. Blood. 17 novembre. 2016; 128(20): 2468-71.
- Bernhard B, Gräni C. 18F-FDG PET/CT imaging in the workup of cardiac and pericardial masses. J Nucl Cardiol. Dicembre. 2022; 29(6): 3466-8.
- Rahbar K, Seifarth H, Schäfers M, Stegger L, Hoffmeier A, Spieker T, et al. Differentiation of Malignant and Benign Cardiac Tumors Using 18 F-FDG PET/CT. J Nucl Med. giugno 2012; 53(6): 856-63.
- Mahoozi H, Zittermann A, Hakim Meibodi K, Burchert W, Gummert J, Mirow N. Erdheim-Chester Disease in a Female Cardiac Surgery Patient. Thorac Cardiovasc Surg. 18 maggio. 2011; 60(06): 428-30.